Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Sun Pharmaceutical Industries Europe B.V., Polarisavenue 87, 2132JH Hoofddorp, Netherlands
Pharmacotherapeutic group: Antineoplastic agents, other antineoplastic agents
ATC code: L01XX48
Sonidegib is an orally bioavailable inhibitor of the Hh signalling pathway. It binds to Smoothened (Smo), a G protein-coupled receptor-like molecule that positively regulates the Hh pathway and eventually activates and releases glioma-associated oncogene (GLI) transcription factors which induces the transcription of Hh target genes involved in proliferation, differentiation and survival. Aberrant Hh signalling has been linked to the pathogenesis of several types of cancer, including basal cell carcinoma (BCC). Sonidegib binding to Smo will inhibit Hh signalling and consequently block signal transduction.
The sonidegib plasma concentration-QTc analysis showed that the upper bound of one-sided 95% confidence interval for QTc increase was below 5 msec at steady-state Cmax for 800 mg daily doses, which provide 2.3-fold plasma exposure compared with the recommended 200 mg dose. Therefore, therapeutic doses of Odomzo are not expected to cause clinically significant QTc prolongation. Further, sonidegib plasma concentrations above those achieved with the therapeutic doses were not associated with life-threatening arrhythmias or torsades de pointes.
Tumour response was independent of Odomzo dose or plasma concentration in the dose range of 200 mg to 800 mg.
A phase II, randomised double-blind study of two dose levels (200 mg or 800 mg once daily) of Odomzo was conducted in 230 patients with either locally advanced basal cell carcinoma (laBCC) (n=194) or metastatic basal cell carcinoma (mBCC) (n=36). Of the 230 patients, 16 had a diagnosis of Gorlin Syndrome (15 laBCC and 1 mBCC). Adult (≥18 years of age) patients with laBCC or mBCC who were not candidates for radiotherapy, surgery or other local therapies, were randomised to receive Odomzo at either 200 mg or 800 mg daily until disease progression or unacceptable toxicity.
The primary efficacy endpoint of the study was objective response rate according to modified Response Evaluation Criteria in Solid Tumours (mRECIST) in patients with laBCC and RECIST 1.1 in patients with mBCC as determined by central review. The secondary endpoints included duration of response, time to tumour response and progression free survival (PFS) according to mRECIST in patients with laBCC and RECIST 1.1 in patients with mBCC as determined by central review.
For patients with laBCC, the Independent Review Committee (IRC) Composite Overall Response was integrated from centrally evaluated MRI scans, digital clinical photographs and histopathology according to mRECIST. For LaBCC, multiple punch biopsies were taken each time a response assessment was confounded by presence of lesion ulceration, cyst, and or scarring/fibrosis. MRI tumour response was evaluated by RECIST 1.1. Response by digital clinical photograph was evaluated by World Health Organization (WHO) adapted criteria [partial response (PR): ≥50% decrease in the sum of the product of perpendicular diameters (SPD) of a lesion; complete response (CR): disappearance of all lesions; progressive disease: ≥25% increase in the SPD of lesions]. For a composite Complete Response, all modalities used for assessment had to demonstrate absence of tumour.
Of the 230 patients randomised, 79 patients were assigned to Odomzo 200 mg. Of these 79 patients, 66 (83.5%) were laBCC patients (37 [46.8%] with aggressive histology and 29 [36.7%] with non-aggressive histology) and 13 (16.5%) were mBCC patients. The median age of all patients receiving Odomzo 200 mg was 67 years (59.5% were >65 years of age), 60.8% were male and 89.9% Caucasian.
The majority of patients (laBCC 74%, mBCC 92%) had undergone prior therapies including surgery (laBCC 73%, mBCC 85%), radiotherapy (laBCC 18%, mBCC 54%) and antineoplastic therapies (laBCC 23%, mBCC 23%).
The key efficacy results per central review and local investigator assessment are presented in Table 4.
Table 4. Efficacy overview per central review and local investigator assessment by FASa:
| Odomzo 200 mg | ||
|---|---|---|
| laBCC N=66 | laBCC N=66 | |
| Objective response rate, n (%) | 37 (56.1) | 47 (71.2) |
| 95% CI | (43.3, 68.3) | (58.7, 81.7) |
| Best overall response, n (%) | ||
| Complete response | 3 (4.5)b | 6 (9.1) |
| Partial response | 34 (51.5) | 41 (62.1) |
| Disease stabilisation | 23 (34.8) | 13 (19.7) |
| Disease progression | 1 (1.5) | 1 (1.5) |
| Unknown | 5 (7.6) | 5 (7.6) |
| Time to tumour response (months) | ||
| Median | 4.0 | 2.5 |
| 95% CI | (3.8, 5.6) | (1.9, 3.7) |
| Duration of response | ||
| No. of events* | 11 | 22 |
| No. censored | 26 | 25 |
| Median (months) | 26.1 | 15.7 |
| 95% CI | (NE) | (12.0, 20.2) |
| Event-free probability (%), (95% CI) | ||
| 6 months | 86.4 (67.7, 94.7) | 89.8 (74.8, 96.1) |
| 9 months | 74.9 (54.4, 87.2) | 80.7 (63.5, 90.4) |
| 12 months | 64.9 (42.3, 80.4) | 71.4 (53.1, 83.6) |
| Progression-free survival | ||
| No. of events* | 16 | 28 |
| No. censored | 50 | 38 |
| Median (months) | 22.1 | 19.4 |
| 95% CI | (NE) | (16.6, 23.6) |
| Progression-free survival probability (%), (95% CI) | ||
| 6 months | 94.8 (84.6, 98.3) | 94.7 (84.5, 98.3) |
| 12 months | 82.0 (66.7, 90.7) | 76.0 (60.7, 85.4) |
a Full analysis set included all randomised patients (intent-to-treat population).
b Using only negative histology to define CR among patients who have at least a PR from other modalities (MRI or photography) resulted in a CR rate of 21.2%.
* Event refers to disease progression or death due to any reason.
FAS: Full analysis set
CI: confidence interval
NE: not estimable
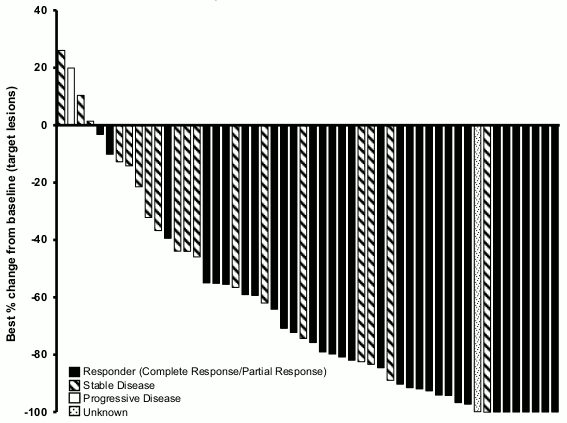
Figures 1 shows the best change in target lesion size for each patient with laBCC at the dose of 200 mg per central review.
Figure 1. Best change from baseline in the target lesions of laBCC patients per central review assessment by FAS:
Patient-reported outcomes were evaluated as an exploratory endpoint using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and its associated head and neck cancer specific module (H&N35).
The majority of patients experienced maintenance and/or improvement in their disease-related symptoms, functioning, and health status. Time to deterioration in the pre-specified PRO scales (corresponding to >10-point worsenings without subsequent improvement) essentially mirrored the estimated PFS.
In the pivotal study, 29.1% of patients discontinued due to adverse events, which were mostly mild or moderate (see section 4.8).
The European Medicines Agency has waived the obligation to submit the results of studies with Odomzo in all subsets of the paediatric population in basal cell carcinoma (see section 4.2 for information on paediatric use).
Efficacy and safety of sonidegib have been studied in two clinical studies involving a total of 62 paediatric patients. Study CLDE225X2104 was a Phase I/II study of sonidegib in paediatric patients with recurrent or refractory medulloblastoma or other tumours potentially dependent on the Hedgehog (Hh) signalling pathway and adult patients with recurrent or refractory medulloblastoma. Study CLDE225C2301 was a Phase II, multi-centre, open-label, single-arm study of the efficacy and safety of oral sonidegib in patients with Hh-activated relapsed medulloblastoma. Results show a lack of significant efficacy despite the enrichment strategy focussed on Hh-activated medulloblastoma.
Following the administration of a single dose of Odomzo (100 mg to 3000 mg) without food in patients with cancer, the median time-to-peak concentration (Tmax) was 2 to 4 hours. Sonidegib exhibited dose-proportional increases in AUC and Cmax over the dose range from 100 mg to 400 mg, but less than dose-proportional increases above 400 mg. There was no evidence of clearance change with repeated dosing based on the population pharmacokinetic analysis and estimated accumulation at steady state was 19-fold irrespective of dose. Steady state was reached approximately 4 months after starting sonidegib. The average steady state Ctrough for 200 mg was 830 ng/ml (range 200 to 2400 ng/ml) in cancer patients. Compared to the fasted state, the Cmax and AUC of Odomzo 800 mg was increased 7.8- and 7.4-fold, respectively when the dose was given with a high-fat meal. Compared to the fasted state, the Cmax and AUC of Odomzo 200 mg was increased 2.8- and 3.5-fold, respectively, when the dose was given with a light meal. Compared to the fasted state, the Cmax and AUC of Odomzo 200 mg increased 1.8- and 1.6-fold, respectively, when a moderate meal was taken 2 hours before the administration. A moderate meal taken 1 hour after the administration of Odomzo 200 mg provided similar exposures compared to the fasted state.
Based on a population pharmacokinetic analysis of 351 patients who received oral doses of Odomzo in the dose range of 100 mg to 3000 mg, the apparent steady-state volume of distribution (Vss/F) was 9170 litres. Steady-state level of sonidegib in the skin was 6-fold higher than in plasma.
Sonidegib was highly bound to human plasma proteins (human serum albumin and alpha-1 acid glycoprotein) in vitro (>97%), and binding was not concentration-dependent from 1 ng/ml to 2500 ng/ml.
Based on in vitro data, sonidegib is not a substrate of P-gp, BCRP or multi-resistance protein 2 (MRP2). Sonidegib did not inhibit apical efflux transporters, P-gp or MRP2, hepatic uptake transporters OATP1B1 or OATP1B3, renal organic anion uptake transporters OAT1 and OAT3, or the organic cation uptake transporters OCT1 or OCT2 at clinically relevant concentrations.
Sonidegib is primarily metabolised by CYP3A4. Unchanged sonidegib represented 36% of circulating radioactivity and the major circulating metabolite (45% of parent exposure) identified in plasma is the hydrolysis product of sonidegib and is pharmacologically inactive. All the metabolites were deemed 4 to 90 times less potent than sonidegib.
Sonidegib and its metabolites are eliminated primarily by the hepatic route with 93.4% of the administered dose recovered in the faeces and 1.95% recovered in urine. Unchanged sonidegib in faeces represented 88.7% of the administered dose and was not detectable in urine. The elimination half-life (t1/2) of sonidegib estimated from population pharmacokinetic modeling was approximately 28 days.
The pharmacokinetics of sonidegib were examined in subjects with mild (Child-Pugh class A; n=8), moderate (Child-Pugh class B; n=8) or severe (Child-Pugh class C; n=9) hepatic impairment and in 8 healthy subjects with normal hepatic function. Cmax of sonidegib after a single oral 800 mg dose was 20%, 21% and 60% lower in mild, moderate and severe hepatic impairment, respectively, compared to normal hepatic function. AUC inf of sonidegib was 40%, 22% and 8% lower, respectively. AUClast was 35% lower in mild hepatic impairment, 14% higher in moderate hepatic impairment and 23% lower in severe hepatic impairment. No dose adjustment is necessary in patients with hepatic impairment.
The effect of renal impairment on the systemic exposure of sonidegib has not been studied. Since sonidegib is not renally excreted, no change in systemic exposure is anticipated in patients with renal impairment. A population pharmacokinetic analysis did not find significant influence of renal function (creatinine clearance >27 ml/min) on the apparent clearance (CL/F) of sonidegib suggesting that dose adjustment is not necessary in patients with renal impairment.
Population pharmacokinetic analyses showed that there are no clinically relevant effects of age (range tested from 20-93 years, mean 61 years), body weight (range tested 42-181 kg, mean 77 kg), gender, or creatinine clearance (range tested 27.3-290 ml/min, mean 92.9 ml/min) on the systemic exposure of sonidegib.
The Cmax and AUCinf of sonidegib in Japanese healthy subjects were 1.56 and 1.68-fold higher, respectively, than those seen in Western healthy subjects for a single dose of 200 mg.
Sonidegib was evaluated in rats and dogs.
The majority of adverse effects of sonidegib can be attributed to its pharmacological mechanism of action on developmental pathways and effects in rats and dogs were similar. Most effects occurred close to the intended human exposures. These effects observed at clinically relevant exposures include closure of bone growth plates, effects on growing teeth, effects on the male and female reproductive tract, atrophy of the hair follicles with alopecia, gastrointestinal toxicity with body weight loss and effects on lymph nodes. At exposures well above the clinical exposure, an additional target organ was the kidney.
Carcinogenicity studies have not been performed with sonidegib, but sonidegib was not genotoxic in studies conducted in vitro and in vivo.
Sonidegib was shown to be foetotoxic in rabbits, as evidenced by abortion and/or complete resorption of foetuses and teratogenic resulting in severe malformations at very low exposure. Teratogenic effects included vertebral, distal limb and digit malformations, severe craniofacial malformations and other severe midline defects. Foetotoxicity in rabbits was also seen at very low maternal exposure. There was reduced fertility at low exposure in female rats. For sonidegib-treated male rats, exposure at approx. 2-fold the clinical exposure did not impact male fertility.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.