Source: European Medicines Agency (EU) Revision Year: 2022 Publisher: Global Blood Therapeutics Netherlands B.V., Strawinskylaan 3051, 1077ZX Amsterdam, Netherlands
Pharmacotherapeutic group: Other haematological agents
ATC code: B06AX03
Voxelotor is a haemoglobin S (HbS) polymerisation inhibitor that binds to HbS with a 1:1 stoichiometry and exhibits preferential partitioning to red blood cells (RBCs). By increasing the affinity of Hb for oxygen, voxelotor demonstrates dose-dependent inhibition of HbS polymerisation. Voxelotor inhibits RBC sickling and improves RBC deformability.
The pharmacodynamic effect of voxelotor treatment demonstrated a dose-dependent increase in Hb oxygen affinity as determined by the change in p20 and p50 (partial pressure of oxygen at which Hb oxygen saturation of 20% or 50% is achieved) that was linearly correlated with voxelotor exposure leading to inhibition of HbS polymerisation. The impact of the anti-polymerisation effect is to reduce measures of haemolysis (indirect bilirubin) with a concomitant decrease in percent reticulocyte count and an increase in Hb consistent with improvement in haemolytic anaemia.
At plasma concentrations approximately 2-fold above therapeutic concentrations, voxelotor does not prolong QT interval to any clinically relevant extent.
The efficacy and safety of voxelotor in patients with SCD was evaluated in a randomised, double-blind, placebo-controlled, multicentre study (EudraCT2016-003370-40). In this study, 274 patients were randomised to daily oral administration of voxelotor 1,500 mg (N=90), voxelotor 900 mg (N=92), or placebo (N=92). Patients were included if they had baseline Hb ≥5.5 g/dL (3.41 mmol/L) to ≤10.5 g/dL (6.52 mmol/L) and 1 to 10 vaso-occlusive crisis (VOC) events within 12 months prior to enrolment. Otherwise eligible patients on stable doses of hydroxycarbamide for at least 90 days were allowed to continue hydroxycarbamide therapy throughout the study. Randomization was stratified by patients already receiving hydroxycarbamide (yes, no), geographic region (North America, Europe, Other), and age (12 to <18 years, 18 to 65 years). Key exclusion criteria included patients who (1) were receiving regular RBC transfusions, (2) received RBC transfusions within 60 days, (3) received erythropoietin within 28 days of enrolment, (4) had known active hepatitis A, B, or C or who were known to be human immunodeficiency virus (HIV) positive (5) had severe renal insufficiency, (6) had uncontrolled liver disease, (7) were pregnant, or (8) were breast-feeding.
Seventy-five percent of patients had HbSS genotype, 15% had HbS/β0 - thalassemia, 4% HbS/β+ - thalassemia, 3% HbSC, and 3% other sickle cell variants. The majority were receiving hydroxycarbamide therapy (65%). The median age was 24 years (range: 12 to 64 years); 46 (17%) patients were 12 to <18 years of age. Median baseline Hb was 8.5 g/dL (5.28 mmol/L) (5.9 to 10.8 g/dL [3.66 to 6.70 mmol/L]). One hundred and fifteen (42%) had 1 VOC event and 159 (58%) had 2 to 10 events within 12 months prior to enrolment. Of the 274 patients, 75 (27.4%) discontinued the study early. The main reasons for discontinuation were withdrawal of consent (10.2%) and adverse events (8.4%).
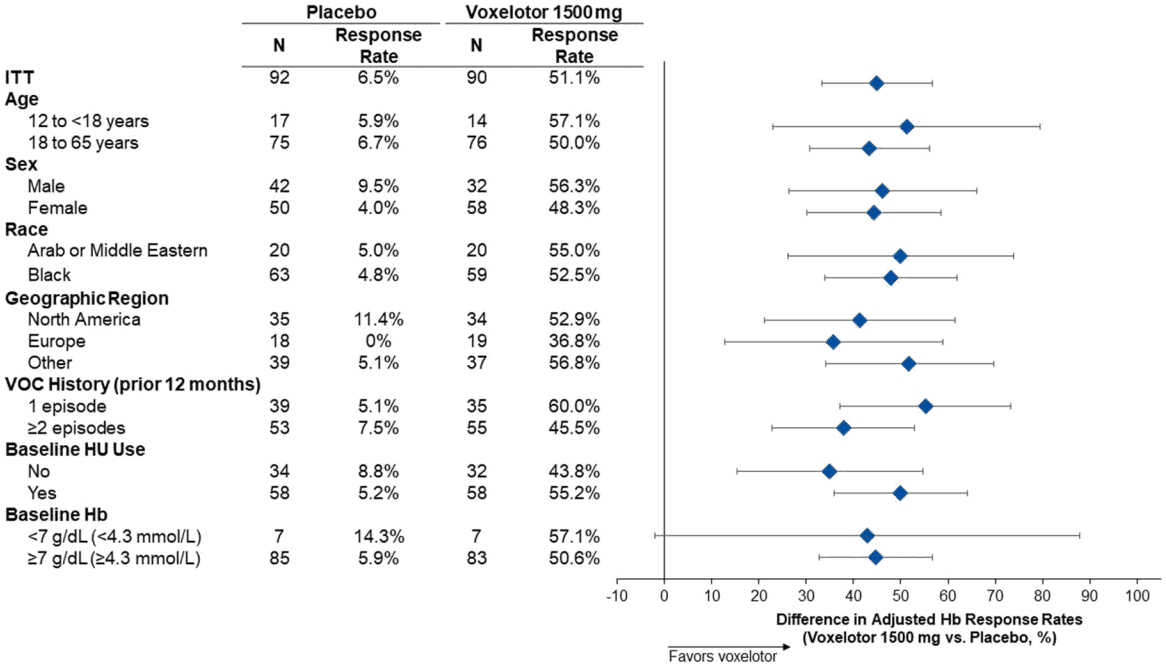
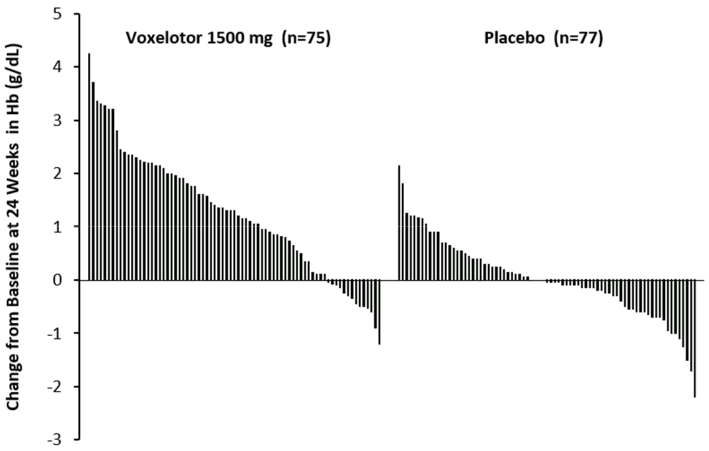
Efficacy was based on the following primary endpoint: Hb response rate defined as a Hb increase of >1 g/dL (0.62 mmol/L) from baseline to Week 24 in patients treated with voxelotor 1,500 mg versus placebo. The response rate for voxelotor 1,500 mg was 51.1% (46/90) compared to 6.5% (6/92) in the placebo group (p<0.001). No outlier subgroups were observed (Figure 1). The increase in Hb was observed beginning at Week 2 and maintained through Week 72. The distribution of Hb change from baseline for individual patients completing 24 weeks of treatment with voxelotor 1,500 mg or placebo is depicted in Figure 2.
Figure 1. Haemoglobin response at Week 24 by subgroup (voxelotor 1,500 mg vs placebo) (intent-to-treat [ITT] population):
Figure 2. Subject-level change from baseline in haemoglobin at Week 24 in patients who completed 24 weeks of treatmenta,b:
Additional efficacy evaluation included change in Hb and percent change in indirect bilirubin and percent reticulocyte count from baseline to Week 24 and Week 72 (Table 2).
Table 2. Adjusted mean (SE) change from baseline to Weeks 24 and 72 in haemoglobin and clinical measures of haemolysis (ITT population):
| Week 24 | Week 72 | |||
|---|---|---|---|---|
| Oxbryta 1,500 mg QD (N=90) | Placebo (N=92) | Oxbryta 1,500 mg QD (N=90) | Placebo (N=92) | |
| Haemoglobin g/dL mmol/L | 1.13 (0.13) 0.70 (0.08) | -0.10 (0.13) -0.06 (0.08) | 1.02 (0.15) 0.63 (0.09) | 0.02 (0.15) 0.01 (0.09) |
| P-value | <0.001 | <0.001 | ||
| Indirect Bilirubin % | -29.1 (3.5) | -2.8 (3.5) | -23.9 (4.9) | 2.7 (4.9) |
| Percent Reticulocyte Count % | -18.0 (4.7) | 6.8 (4.7) | -7.6 (5.5) | 11.0 (5.5) |
SE = standard error
The total number and annualized incidence rate (IR) of on-treatment VOCs were as follows: 219 events with adjusted IR of 2.4 events/year in the voxelotor 1,500 mg group and 293 events with adjusted IR of 2.8 events/year in the placebo group. No statistically significant difference was observed between the treatment groups; however, the study was not designed to detect a difference.
In the pivotal study leg ulcers were observed at baseline: 4 in the voxelotor 1,500 mg group, 3 in the placebo group. In the voxelotor group, all 4 patients with leg ulcers at baseline improved after treatment (3 patients had resolution by Week 72 and 1 patient with moderate severity at baseline improved to mild). One patient developed new leg ulcers during treatment. In contrast, in the placebo group, only 1 of the 3 patients with leg ulcers at baseline had improvement and 5 patients developed new leg ulcers.
The European Medicines Agency has waived the obligation to submit the results of studies with voxelotor in paediatric population from birth to <6 months of age in the treatment of haemolytic anaemia due to SCD. See section 4.2 for information on paediatric use.
The European Medicines Agency has deferred the obligation to submit the results of studies with voxelotor in paediatric population from 6 months of age to < 12 years of age in the treatment of haemolytic anaemia due to SCD, as well as further data from studies in the paediatric population less than 18 years of age. See section 4.2 for information on paediatric use.
Study GBT440 007 is an ongoing Phase 2, multicentre, open-label single- and multiple-dose study designed to evaluate the safety, tolerability, PK, and efficacy of voxelotor in paediatric patients with SCD. Efficacy and safety data from the completed multiple-dose part in patients 12 to <18 years of age with SCD (HbSS or HbS/β0 - thalassemia) who received voxelotor 900 mg or 1,500 mg for 24 weeks are discussed here.
In total, 25 patients received voxelotor 900 mg and 15 patients received voxelotor 1,500 mg. The median age in the voxelotor 1,500 mg group was 14 years (range: 12-17 years), 33% were male and 73% were Black. Most patients in the 1,500 mg group had HbSS genotype (80%) and all used hydroxycarbamide at baseline. Thirty-three percent (33%) had no history of VOC within the 12 months prior to screening and 33% had 1 or 2 VOCs in the 12 months prior to screening. Median baseline Hb level was 8.8 g/dL (5.46 mmol/L). Eighty-eight percent (88.0%) of patients in the voxelotor 900 mg group and 80.0% of patients in the voxelotor 1,500 mg group completed the study with 24 weeks of dosing. One patient in the voxelotor 1,500 mg group discontinued due to an adverse reaction (Grade 1 diarrhoea).
Efficacy assessments included clinical measures of anaemia (Hb) and haemolysis (percent reticulocyte count and indirect bilirubin). Consistent with the results of the Phase 3 Study of voxelotor, improvements in Hb were observed as early as Week 2 and were maintained through Week 24: median change in Hb from baseline to Week 20/Week 24 average was 0.7 g/dL (0.43 mmol/L) for the 1,500 mg group, decrease in percent reticulocyte count at 24 weeks was -17.4% (-35.6, -36.5) and decrease in indirect bilirubin was -42.8% (-50.5, -15.4) in the voxelotor 1,500 mg group. The safety profile was consistent with that observed in the Phase 3 Study.
The median plasma and whole blood Tmax of voxelotor after oral administration is 2 hours. The mean peak concentrations in whole blood and RBCs are observed between 6 and 18 hours after oral administration. The PK are linear over the dose range of 100 mg to 2,800 mg. Steady-state after repeated administration is reached within 8 days and exposures of voxelotor plasma and whole blood (Table 3) are consistent with accumulation predicted based on single dose data in patients with SCD.
Table 3. Pharmacokinetics parameters of voxelotor in plasma and whole blood (Subjects with SCD):
| PK parameter | Voxelotor 1,500 mg Geometric mean (%CV) |
|---|---|
| AUC0-24h (microgram∙hr/mL) | 278 (28.4) |
| Cmax (microgram/mL) | 14 (24.5) |
| Half-life (hours) | 38.7 (30.2) |
| AUC0-24h (microgram∙hr/mL) | 3830 (33.5) |
| Cmax (microgram/mL) | 180 (31) |
In healthy subjects, administration of a single 900 mg dose of Oxbryta with a high-fat meal resulted in a 45% and 42% increase in whole blood Cmax and AUC, respectively, compared to fasted conditions.
In clinical studies, subjects with SCD took voxelotor without instructions with respect to food intake and had plasma and whole blood voxelotor exposures similar to subjects with SCD who took voxelotor after an overnight fast. The difference is less than 20% for any of the parameters and not considered to be clinically significant. Therefore, voxelotor can be taken with or without food.
Voxelotor is absorbed into plasma and is then distributed predominantly into RBCs due to its preferential binding to Hb. Voxelotor apparent volume of distribution of the central compartment and peripheral compartment in patients with SCD are 333 L and 72.3 L in plasma, respectively. Protein binding is 99.8% in vitro. The blood-to-plasma ratio is approximately 15:1 in patients with SCD.
The pharmacokinetics of voxelotor in healthy subjects is different from patients with SCD due to the differences in blood-to-plasma partitioning (ratio 32:1). The volume of distribution in healthy subjects is approximately 754 L.
In vitro and in vivo studies indicate that voxelotor is extensively metabolized through Phase I (oxidation and reduction), Phase II (glucuronidation) and combinations of Phase I and II metabolism. Oxidation of voxelotor is mediated primarily by CYP3A4, with minor contribution from CYP2C19, CYP2B6, and CYP2C9. Sulfatation of voxelotor is mediated primarily by SULT1B1 and SULT1C4 and direct glucuronidation of voxelotor is mediated by UGT1A1 and UGT1A9. The major plasma metabolite results from O-dealkylation-sulfation and represents 16.8% of voxelotor-related material in plasma. Five further metabolites accounted for a total of 23% of voxelotor-related material in plasma, with individual contributions up to 9%. All other metabolites were less than 5%.
The major route of elimination of voxelotor is by metabolism with subsequent excretion of metabolites into urine and faeces. The excretion of unchanged voxelotor is minimal (< 1% of dose in urine). The geometric mean (CV) terminal elimination half-life of voxelotor in patients with SCD is 38.7 hours (30.2) with concentrations in plasma, and whole blood declining in parallel. The apparent oral clearance of voxelotor was estimated as 6.1 L/h in plasma in patients with SCD.
There was no clinically significant effect of renal function on the excretion of voxelotor in subjects without SCD and patients with SCD. Following a single 900 mg dose of voxelotor, whole blood exposures in subjects with severe renal impairment (eGFR <30 mL/min/1.73 m²) were 25% lower compared to healthy controls. The unbound plasma concentrations were comparable. In patients with SCD, a trend for higher voxelotor exposure was observed with lower Cystatin C levels. Higher levels of Cystatin C typically observed with renal impairment were not associated with higher voxelotor exposure.
Voxelotor has not been evaluated in patients with ESRD requiring dialysis.
In plasma, the Cmax was 1.2-fold higher in subjects with mild hepatic impairment (Child Pugh A), 1.5-fold higher in subjects with moderate hepatic impairment (Child Pugh B) and 1.4-fold higher in subjects with severe hepatic impairment (Child Pugh C), and the AUCinf was 1.1-fold higher in subjects with mild hepatic impairment, 1.2-fold higher in subjects with moderate hepatic impairment and 1.9-fold higher in subjects with severe hepatic impairment. In whole blood, increase in exposure was similar to that in plasma. No dose adjustment is warranted in subjects with mild to moderate hepatic impairment, but it is recommended to reduce the daily dose of voxelotor to 1,000 mg in subjects with severe hepatic impairment (see section 4.2). The plasma and whole blood Cmax values in patients with severe hepatic impairment after dose adjustment are expected to be similar to those in patients with normal hepatic function treated at the recommended dose of 1,500 mg daily. The plasma and whole blood AUC are expected to be ~25% higher in subjects with severe hepatic impairment after dose adjustment compared to those in patients with normal hepatic function treated at the recommended dose of 1,500 mg daily.
No clinically significant differences in the pharmacokinetics of voxelotor were observed based on gender, race, and body weight (28 to 135 kg).
No clinically significant differences in the pharmacokinetics of voxelotor were observed based on age (12 to 59 years).
The blood-to-plasma partitioning of voxelotor increases with increasing haematocrit. As haematocrit increased from 30.5% in SCD patients (median at 1,500 mg daily) to the maximum haematocrit measured at 1,500 mg daily (35.1%), the blood-to-plasma partitioning increased from 14.8 to 16.4 (11% increase).
Voxelotor steady state whole blood AUC and Cmax were 50% and 45% higher in HbSC genotype patients (n=11) compared to HbSS genotype (n=220) patients and voxelotor steady state plasma AUC and Cmax were 23% and 15% higher in HbSC genotype patients compared to HbSS genotype patients.
CYP enzymes: In vitro, voxelotor is an inhibitor and inducer of CYP2B6 and an inhibitor of CYP2C8, CYP2C9, CYP2C19 and CYP3A4. The clinical relevance is currently unknown (see section 4.5).
UGT enzymes: In vitro data indicate that voxelotor is not an inhibitor of UGT1A1, UGT1A9 and UGT2B7 at maximal systemic concentration. Due to solubility issues, no concentrations up to maximal intestinal concentrations could be investigated for UGT1A1. No inhibition was observed towards UGT1A1 up to 100 micromol (the highest concentration investigated).
Transporter-mediated interactions: Voxelotor is not an inhibitor of P-gp, BCRP, OATP1B3, OCT2, OAT1, MATE2-K, or BSEP. Voxelotor act as an inhibitor of OATP1B1, OAT3 and MATE1 transporters (see section 4.5). Voxelotor is not a substrate of P-gp, BCRP, OATP1A2, OATP1B1, OATP1B3, or BSEP.
Adverse reactions not observed in clinical studies, but seen in animals at exposure levels similar to clinical exposure levels and with possible relevance to clinical use were as follows.
The major findings associated with repeat-dose administration of voxelotor was compensatory erythropoiesis, manifested as increased red blood cell mass (↑ RBC, HCT, Hb, RET) correlated microscopically with hypercellular bone marrow and splenic red pulp and increased splenic weight in rats, mice and cynomolgus monkeys. In monkeys, early stages of this effect were seen at dose levels comparable with clinical exposure (exposure multiple of ~0.6 based on the plasma Cmax values). Voxelotor also caused GI intolerance attributed to local irritation. Other findings attributed to voxelotor include induction of CYP enzymes in the liver of mice and rats, altered T cell-dependent antigen response in rodents and monkeys and prolongation of corrected QT (QTc) intervals in monkeys. Following the immunization with keyhole limpet hemocyanin (KLH), voxelotor caused the significantly reduced IgG (rats, monkeys) and IgM (monkeys) titres, a delayed peak in the antibody response (monkeys) and the changes in the relative lymphocyte distribution (rats). These effects were seen at the exposure multiple of the anticipated clinical exposure ~0.6 in monkeys and ~4.0 in rats based on plasma Cmax value. Treatment with voxelotor at the exposure multiple ~2.5 of the anticipated clinical exposure led to the QT and QTc intervals prolongation in monkeys.
Treatment of rats with voxelotor at exposure multiple ~4 of the anticipated clinical exposure caused a reduced sperm motility and an increased percentage of abnormal sperm, as well as an increased testicular and prostate weight and reduced seminal vesicles weight. These effects did not, however, affect the reproductive performance. Voxelotor was not teratogenic in rats and rabbits at exposure levels causing maternal toxicity (exposure multiple based on blood AUC of 2.8 in rats and 0.3 in rabbits). Voxelotor is excreted in milk of lactating rats. Milk exposure was up to 0.4-fold plasma exposure of the dams, leading to subsequent plasma exposure in pups. In the pre- and postnatal developmental toxicity study, adverse effects on the progeny, manifested as reduced pup viability index and persistently lower pup weight, were seen at the predicted exposure multiple of ~2.6 of the anticipated human exposure.
Environmental risk assessment studies have shown that voxelotor is not bioaccumulative and toxic to the environment; however, it has the potential to be persistent in sediments (see section 6.6).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.