OXYTROL Transdermal system Ref.[10892] Active ingredients: Oxybutinin
Source: FDA, National Drug Code (US) Revision Year: 2017
12.1. Mechanism of Action
The free base form of oxybutynin is pharmacologically equivalent to oxybutynin hydrochloride. Oxybutynin acts as a competitive antagonist of acetylcholine at postganglionic muscarinic receptors, resulting in relaxation of bladder smooth muscle. In patients with conditions characterized by involuntary detrusor contractions, cystometric studies have demonstrated that oxybutynin increases maximum urinary bladder capacity and increases the volume to first detrusor contraction.
Oxybutynin is a racemic (50:50) mixture of R- and S-isomers. Antimuscarinic activity resides predominantly in the R-isomer. The active metabolite, N-desethyloxybutynin, has pharmacological activity on the human detrusor muscle that is similar to that of oxybutynin in in vitro studies.
12.3. Pharmacokinetics
Absorption
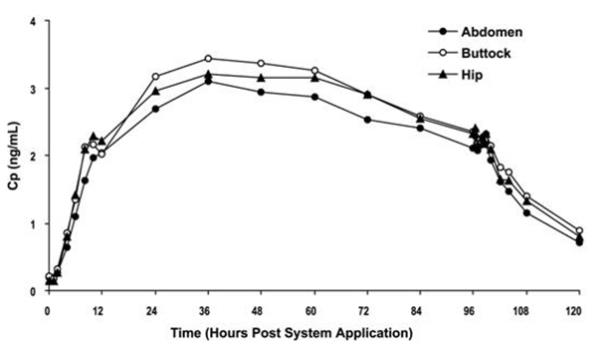
Oxybutynin is transported across intact skin and into the systemic circulation by passive diffusion across the stratum corneum. The average daily dose of oxybutynin absorbed from the 39 cm² OXYTROL system is 3.9 mg. The average (SD) nominal dose, 0.10 (0.02) mg oxybutynin per cm² surface area, was obtained from analysis of residual oxybutynin content of systems worn over a continuous 4-day period during 303 separate occasions in 76 healthy volunteers. Following application of the first OXYTROL 3.9 mg/day system, oxybutynin plasma concentrations increase for approximately 24 to 48 hours, reaching average maximum concentrations of 3 to 4 ng/mL. Thereafter, steady concentrations are maintained for up to 96 hours. Absorption of oxybutynin is bioequivalent when OXYTROL is applied to the abdomen, buttocks, or hip. Average plasma concentrations measured during a randomized, crossover study of the three recommended application sites in 24 healthy men and women are shown in Figure 2.
Figure 2. Average plasma oxybutynin concentrations (Cp) in 24 healthy male and female volunteers during single-dose application of OXYTROL 3.9 mg/day to the abdomen, buttock, and hip (System removal at 96 hours):
Steady-state conditions are reached during the second OXYTROL application. Average steady-state plasma concentrations were 3.1 ng/mL for oxybutynin and 3.8 ng/mL for N-desethyloxybutynin (Figure 3). Table 3 provides a summary of pharmacokinetic parameters of oxybutynin in healthy volunteers after single and multiple applications of OXYTROL.
Figure 3. Average (SEM) steady-state oxybutynin and N-desethyloxybutynin plasma concentrations (Cp) measured in 13 healthy volunteers following the second transdermal system application in a multiple-dose, randomized, crossover study:
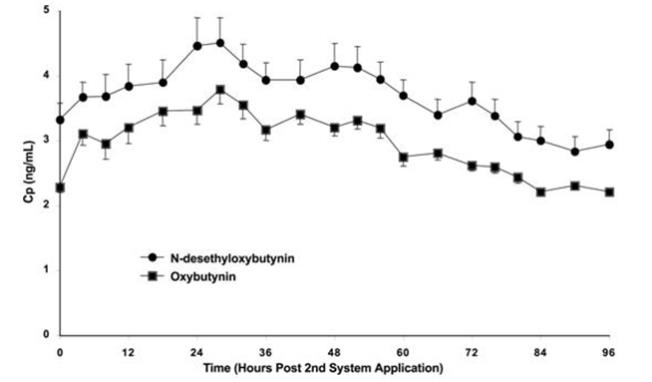
Table 3. Mean (SD) oxybutynin pharmacokinetic parameters from single and multiple dose studies in healthy men and women volunteers after application of OXYTROL on the abdomen:
| Dosing | Oxybutynin | |||
|---|---|---|---|---|
| Cmax (SD) (ng/mL) | Tmax‡ (hr) | Cavg (SD) (ng/mL) | AUC (SD) (ng/mLxh) | |
| Single | 3.0 (0.8) | 48 | - | 245 (59)§ |
| 3.4 (1.1) | 36 | - | 279 (99)§ | |
| Multiple | 6.6 (2.4) | 10 | 4.2 (1.1) | 408 (108)¶ |
| 4.2 (1.0) | 28 | 3.1 (0.7) | 259 (57)#Þ | |
‡ Tmax given as median
§ AUCinf
¶ AUC0-96
#Þ AUC0-84
Distribution
Oxybutynin is widely distributed in body tissues following systemic absorption. The volume of distribution was estimated to be 193 L after intravenous administration of 5 mg oxybutynin chloride.
Metabolism
Oxybutynin is metabolized primarily by the cytochrome P450 enzyme systems, particularly CYP3A4, found mostly in the liver and gut wall. Metabolites include phenylcyclohexylglycolic acid, which is pharmacologically inactive, and N-desethyloxybutynin, which is pharmacologically active.
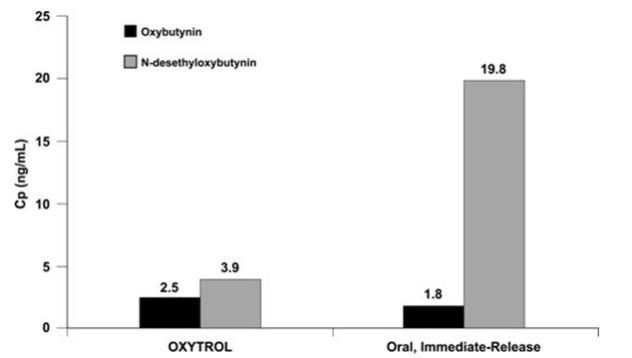
After oral administration of oxybutynin, pre-systemic first-pass metabolism results in an oral bioavailability of approximately 6% and higher plasma concentration of the N-desethyl metabolite compared to oxybutynin (see Figure 4). The plasma concentration area under the time-concentration curve (AUC) ratio of N-desethyl metabolite to parent compound following a single 5 mg oral dose of oxybutynin chloride was 11.9:1.
Transdermal administration of oxybutynin bypasses first-pass gastrointestinal and hepatic metabolism, reducing the formation of the N-desethyl metabolite (see Figure 4). Only small amounts of CYP3A4 are found in skin, limiting pre-systemic metabolism during transdermal absorption. The resulting plasma concentration AUC ratio of N-desethyl metabolite to parent compound following multiple OXYTROL applications was 1.3:1.
Figure 4. Average plasma concentrations (Cp) measured after a single, 96-hour application of the OXYTROL 3.9 mg/day system (AUCinf/96) and a single, 5 mg, oral immediate-release dose of oxybutynin chloride (AUCinf/8) in 16 healthy male and female volunteers:
Following intravenous administration, the elimination half-life of oxybutynin is approximately 2 hours. Following removal of OXYTROL, plasma concentrations of oxybutynin and N-desethyloxybutynin decline with an apparent half-life of approximately 7 to 8 hours.
Excretion
Oxybutynin is extensively metabolized by the liver, with less than 0.1% of the administered dose excreted unchanged in the urine. Also, less than 0.1% of the administered dose is excreted as the metabolite N-desethyloxybutynin.
Specific Populations
Geriatric
The pharmacokinetics of oxybutynin and N-desethyloxybutynin were similar in older and younger patients.
Pediatric
The pharmacokinetics of oxybutynin and N-desethyloxybutynin were not evaluated in individuals younger than 18 years of age.
Gender
There were no significant differences in the pharmacokinetics of oxybutynin in healthy male and female volunteers following application of OXYTROL.
Race
Available data suggest that there are no significant differences in the pharmacokinetics of oxybutynin based on race in healthy volunteers following administration of OXYTROL. Japanese volunteers demonstrated a somewhat lower metabolism of oxybutynin to N-desethyloxybutynin compared to Caucasian volunteers.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
A 24-month study in rats at dosages of oxybutynin chloride of 20, 80 and 160 mg/kg showed no evidence of carcinogenicity. These doses are approximately 6, 25 and 50 times the maximum exposure in humans taking an oral dose based on body surface area.
Oxybutynin chloride showed no increase of mutagenic activity when tested in Schizosaccharomyces pompholiciformis, Saccharomyces cerevisiae, and Salmonella typhimurium test systems. Reproduction studies with oxybutynin chloride in the mouse, rat, hamster, and rabbit showed no definite evidence of impaired fertility.
14. Clinical Studies
The efficacy and safety of OXYTROL were evaluated in patients with urge urinary incontinence in two controlled studies and one open-label extension. Study 1 was a placebo controlled study, comparing the safety and efficacy of OXYTROL at dose levels of 1.3, 2.6, and 3.9 mg/day to placebo in 520 patients. Open-label treatment was available for patients completing the study. Study 2 was a study comparing the safety and efficacy of OXYTROL 3.9 mg/day versus active and placebo controls in 361 patients.
Study 1 was a randomized, double-blind, placebo-controlled, parallel group study of three dose levels of OXYTROL conducted in 520 patients. The 12-week double-blind treatment included an OXYTROL dose of 3.9 mg/day or matching placebo. An open-label, dose titration treatment extension allowed continued treatment for up to an additional 40 weeks for patients completing the double-blind period. The majority of patients were Caucasian (91%) and female (92%) with a mean age of 61 years (range, 20 to 88 years). Entry criteria required that patients have urge or mixed incontinence (with a predominance of urge), urge incontinence episodes of ≥10 per week, and ≥8 micturitions per day. The patient's medical history and a urinary diary during the treatment-free baseline period confirmed the diagnosis of urge incontinence. Approximately 80% of patients had no prior pharmacological treatment for incontinence. Changes in weekly incontinence episodes, urinary frequency, and urinary void volume between placebo and active treatment groups are summarized in Table 4.
Table 4. Mean and median change from baseline to end of treatment (Week 12 or last observation carried forward) in incontinence episodes, urinary frequency, and urinary void volume in patients treated with OXYTROL 3.9 mg/day or placebo for 12 weeks (Study 1):
| Parameter | Placebo (N=127) | Oxytrol 3.9 mg/day (N=120) | ||
|---|---|---|---|---|
| Mean (SD) | Median | Mean (SD) | Median | |
| Weekly Incontinence Episodes | ||||
| Baseline | 37.7 (24.0) | 30 | 34.3 (18.2) | 31 |
| Reduction | 19.2 (21.4) | 15 | 21.0 (17.1) | 19 |
| p value vs. placebo | - | 0.0265ß | ||
| Daily Urinary Frequency | ||||
| Baseline | 12.3 (3.5) | 11 | 11.8 (3.1) | 11 |
| Reduction | 1.6 (3.0) | 1 | 2.2 (2.5) | 2 |
| p value vs. placebo | - | 0.0313ß | ||
| Urinary Void Volume (mL) | ||||
| Baseline | 175.9 (69.5) | 166.5 | 171.6 (65.1) | 168 |
| Increase | 10.5 (56.9) | 5.5 | 31.6 (65.6) | 26 |
| p value vs. placebo | - | 0.0009à | ||
ß Comparison significant if p<0.05
à Comparison significant if p≤0.0167
Study 2 was a randomized, double-blind, study of OXYTROL 3.9 mg/day versus active and placebo controls conducted in 361 patients. The 12-week double-blind treatment included an OXYTROL dose of 3.9 mg/day, an active comparator, and placebo. The majority of patients were Caucasian (95%) and female (93%) with a mean age of 64 years (range, 18 to 89 years). Entry criteria required that all patients have urge or mixed incontinence (with a predominance of urge) and had achieved a beneficial response from the anticholinergic treatment they were using at the time of study entry. The average duration of prior pharmacological treatment was greater than 2 years. The patient's medical history and a urinary diary during the treatment-free baseline period confirmed the diagnosis of urge incontinence. Changes in daily incontinence episodes, urinary frequency, and urinary void volume between placebo and active treatment groups are summarized in Table 5.
Table 5. Mean and median change from baseline to end of treatment (Week 12 or last observation carried forward) in incontinence episodes, urinary frequency, and urinary void volume in patients treated with OXYTROL 3.9 mg/day or placebo for 12 weeks (Study 2):
| Parameter | Placebo (N=117) | OXYTROL 3.9 mg/day (N=121) | ||
|---|---|---|---|---|
| Mean (SD) | Median | Mean (SD) | Median | |
| Daily Incontinence Episodes | ||||
| Baseline | 5.0 (3.2) | 4 | 4.7 (2.9) | 4 |
| Reduction | 2.1 (3.0) | 2 | 2.9 (3.0) | 3 |
| p value vs. placebo | - | 0.0137£ | ||
| Daily Urinary Frequency | ||||
| Baseline | 12.3 (3.3) | 12 | 12.4 (2.9) | 12 |
| Reduction | 1.4 (2.7) | 1 | 1.9 (2.7) | 2 |
| p value vs. placebo | - | 0.1010£ | ||
| Urinary Void Volume (mL) | ||||
| Baseline | 175.0 (68.0) | 171.0 | 164.8 (62.3) | 160 |
| Increase | 9.3 (63.1) | 5.5 | 32.0 (55.2) | 24 |
| p value vs. placebo | - | 0.0010£ | ||
£ Comparison significant if p<0.05
Adhesion
Adhesion was periodically evaluated during the pivotal studies. Of the 4,746 OXYTROL evaluations in the trials, 20 (0.4%) were observed at clinic visits to have become completely detached and 35 (0.7%) became partially detached during routine clinic use. Similar to the pharmacokinetic studies, >98% of the systems evaluated in the pivotal studies were assessed as being ≥75% attached and thus would be expected to perform as anticipated.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.