PEDIPPI Powder for oral suspension Ref.[27782] Active ingredients: Omeprazole
Source: Health Products Regulatory Authority (IE) Revision Year: 2019 Publisher: Xeolas Pharmaceuticals Limited, Hamilton Building, DCU, Glasnevin, Dublin 9, Ireland
4.1. Therapeutic indications
Omeprazole Oral Suspension is indicated for:
Adults
- Treatment of duodenal ulcers
- Prevention of relapse of duodenal ulcers
- Treatment of gastric ulcers
- Prevention of relapse of gastric ulcers
- In combination with appropriate antibiotics, Helicobacter pylori (H. pylori) eradication in peptic ulcer disease
- Treatment of NSAID-associated gastric and duodenal ulcers
- Prevention of NSAID-associated gastric and duodenal ulcers in patients at risk
- Treatment of reflux esophagitis
- Long-term management of patients with healed reflux esophagitis
- Treatment of symptomatic gastro-esophageal reflux disease
Paediatric use
Children over 1 month of age
- Treatment of reflux esophagitis
- Symptomatic treatment of heartburn and acid regurgitation in gastro-esophageal reflux disease
Children over 4 years of age and adolescents
In combination with antibiotics in treatment of duodenal ulcer caused by H. pylori.
4.2. Posology and method of administration
Omeprazole 2 mg/ml Oral Suspension is suitable for doses of ≤15mg. For doses of 20 mg or greater, Omeprazole 4 mg/ml Oral Suspension is suitable.
Posology in adults
Treatment of duodenal ulcers
The recommended dose in patients with an active duodenal ulcer is Omeprazole 20 mg once daily. In most patients healing occurs within two weeks. For those patients who may not be fully healed after the initial course, healing usually occurs during a further two weeks treatment period. In patients with poorly responsive duodenal ulcer Omeprazole 40 mg once daily is recommended and healing is usually achieved within four weeks.
Prevention of relapse of duodenal ulcers
For the prevention of relapse of duodenal ulcer in H. pylori negative patients or when H. pylori eradication is not possible the recommended dose is Omeprazole 20 mg once daily. In some patients a daily dose of 10 mg may be sufficient. In case of therapy failure, the dose can be increased to 40 mg.
Treatment of gastric ulcers
The recommended dose is Omeprazole 20 mg once daily. In most patients healing occurs within four weeks. For those patients who may not be fully healed after the initial course, healing usually occurs during a further four weeks treatment period. In patients with poorly responsive gastric ulcer Omeprazole 40 mg once daily is recommended and healing is usually achieved within eight weeks.
Prevention of relapse of gastric ulcers
For the prevention of relapse in patients with poorly responsive gastric ulcer the recommended dose is Omeprazole 20 mg once daily. If needed the dose can be increased to Omeprazole 40 mg once daily.
H. pylori eradication in peptic ulcer disease
For the eradication of H. pylori the selection of antibiotics should consider the individual patient's drug tolerance, and should be undertaken in accordance with national, regional and local resistance patterns and treatment guidelines.
- Omeprazole 20 mg + clarithromycin 500 mg + amoxicillin 1,000 mg, each twice daily for one week, or
- Omeprazole 20 mg + clarithromycin 250 mg (alternatively 500 mg) + metronidazole 400 mg (or 500 mg or tinidazole 500 mg), each twice daily for one week or
- Omeprazole 40 mg once daily with amoxicillin 500 mg and metronidazole 400 mg (or 500 mg or tinidazole 500 mg), both three times a day for one week.
In each regimen, if the patient is still H. pylori positive, therapy may be repeated.
Treatment of NSAID-associated gastric and duodenal ulcers
For the treatment of NSAID-associated gastric and duodenal ulcers, the recommended dose is Omeprazole 20 mg once daily. In most patients healing occurs within four weeks. For those patients who may not be fully healed after the initial course, healing usually occurs during a further four weeks treatment period.
Prevention of NSAID-associated gastric and duodenal ulcers in patients at risk
For the prevention of NSAID-associated gastric ulcers or duodenal ulcers in patients at risk (age> 60, previous history of gastric and duodenal ulcers, previous history of upper GI bleeding) the recommended dose is Omeprazole 20 mg once daily.
Treatment of reflux esophagitis
The recommended dose is Omeprazole 20 mg once daily. In most patients healing occurs within four weeks. For those patients who may not be fully healed after the initial course, healing usually occurs during a further four weeks treatment period. In patients with severe esophagitis Omeprazole 40 mg once daily is recommended and healing is usually achieved within eight weeks.
Long-term management of patients with healed reflux esophagitis
For the long-term management of patients with healed reflux esophagitis the recommended dose is Omeprazole 10 mg once daily. If needed, the dose can be increased to Omeprazole 20-40 mg once daily.
Treatment of symptomatic gastro-esophageal reflux disease
The recommended dose is Omeprazole 20 mg daily. Patients may respond adequately to 10 mg daily, and therefore individual dose adjustment should be considered. If symptom control has not been achieved after four weeks treatment with Omeprazole 20 mg daily, further investigation is recommended.
Paediatric population
Children over 1 month of age
Treatment of reflux esophagitis
Symptomatic treatment of heartburn and acid regurgitation in gastro-esophageal reflux disease
The posology recommendations are as follows*:
| Age | Weight | Posology |
|---|---|---|
| 1 month to 1 year of age | - | 1 mg/kg once daily. Doses above 1.5 mg/kg/day have not been studied. |
| ≥1 year of age | 10-20 kg | 10 mg once daily. The dose can be increased to 20 mg once daily if needed. |
| ≥2 years of age | >20 kg | 20 mg once daily. The dose can be increased to 40 mg once daily if needed. |
* Individual dose measurements ≤2ml are not indicated
** The 2 mg/ml and 4 mg/ml strengths are equivalent with respect to buffering capacity (same amount of buffer on a ml basis). For doses of ≤15 mg, the 2 mg/ml strength is recommended. The 2 mg/ml strength is indicated for age 1 month to 1 year for administering up to 15 mg and ≥1 year of age for administering 10 mg, to provide sufficient buffering capacity and absorption. For doses of 20 mg or 40 mg, the 4 mg/ml strength is suitable. The 4 mg/ml strength is indicated for administration of 20 mg or 40 mg so that a maximum of 2 doses are required.
Reflux esophagitis: The treatment time is 4-8 weeks.
Symptomatic treatment of heartburn and acid regurgitation in gastro-esophageal reflux disease: The treatment time is 2-4 weeks. If symptom control has not been achieved after 2-4 weeks the patient should be investigated further.
Children over 4 years of age and adolescents
Treatment of duodenal ulcer caused by H. pylori
When selecting appropriate combination therapy, consideration should be given to official national, regional and local guidance regarding bacterial resistance, duration of treatment (most commonly 7 days but sometimes up to 14 days), and appropriate use of antibacterial agents.
The treatment should be supervised by a specialist.
The posology recommendations are as follows:
| Weight | Posology |
|---|---|
| 15-30 kg | Combination with two antibiotics: Omeprazole 10 mg, amoxicillin 25 mg/kg body weight and clarithromycin 7.5 mg/kg body weight are all administrated together two times daily for one week. |
| 31-40 kg | Combination with two antibiotics: Omeprazole 20 mg, amoxicillin 750 mg and clarithromycin 7.5 mg/kg body weight are all administrated two times daily for one week. |
| >40 kg | Combination with two antibiotics: Omeprazole 20 mg, amoxicillin 1 g and clarithromycin 500 mg are all administrated two times daily for one week. |
Special populations
Renal impairment
Dose adjustment is not needed in patients with impaired renal function (see section 5.2).
Hepatic impairment
In patients with impaired hepatic function a daily dose of 10-20 mg may be sufficient (see section 5.2).
Elderly (>65 years old)
Dose adjustment is not needed in the elderly (see section 5.2).
Method of administration
Omeprazole Oral Suspension should be taken on an empty stomach, at least 30 minutes before a meal.
Precautions to be taken before handling or administering the medicinal product
Omeprazole powder for oral suspension requires reconstitution prior to oral administration. For instructions on reconstitution of the medicinal product before administration, see section 6.6.
For instruction for administration via nasogastric (NG) or percutaneous endoscopic gastrostomy (PEG) tubes, see section 6.6.
4.9. Overdose
There is limited information available on the effects of overdoses of omeprazole in humans. In the literature, doses of up to 560 mg have been described, and occasional reports have been received when single oral doses have reached up to 2,400 mg omeprazole (120 times the usual recommended clinical dose). Nausea, vomiting, dizziness, abdominal pain, diarrhoea and headache have been reported. Also apathy, depression and confusion have been described in single cases.
The symptoms described have been transient, and no serious outcome has been reported. The rate of elimination was unchanged (first order kinetics) with increased doses. Treatment, if needed, is symptomatic.
6.3. Shelf life
Dry Powders: 24 months.
Constituted suspension: 28 days.
The constituted suspension should be stored in a refrigerator (2°C-8°C). Store in the original container in order to protect from light. Keep the bottle tightly closed. For up to 2 days it may be stored below 25°C.
6.4. Special precautions for storage
Dry Powders: Do not store above 25°C. Store in the original foil pouch in order to protect from light and moisture.
For storage conditions after reconstitution of the medicinal product, see section 6.3.
6.5. Nature and contents of container
Amber plastic (PET) bottle with powder fitted with a red Polypropylene (PP) closure cap containing powder, all enclosed in an aluminium foil pouch.
Each bottle contains 47 g of powder for oral suspension. Once constituted the bottle contains 90 ml of oral suspension, of which 75 ml is intended for dosing and administration.
Each pack also contains an opaque PP oral dosing syringe (5 ml, graduated at each 1ml and intermediate marks every 0.1ml) with white HDPE plunger, colourless, transparent LDPE bottle adaptor and grey PP replacement cap.
Pack: 1 or 2 bottles.
Not all pack sizes may be marketed
6.6. Special precautions for disposal and other handling
It is recommended that a pharmacist constitutes Omeprazole Oral Suspension prior to its dispensing to the patient.
Preparing and taking the suspension
The container is two compartment system containing powder both in the cap and in the bottle. The two powders first need to be combined and are then to be constituted in water. A red mixing disk will drop into the medicine to help mix the powders and also mix the constituted suspension after addition of the water. It should remain in the bottle. The red cap is replaced by a grey cap after constitution.
Instructions for initial constitution.
Combination of powder in cap and bottle
- Shake the bottle for 10 seconds to loosen the powder.
- Twist the red cap anti-clockwise (see arrow on cap) until the seal is broken to release the powder in the red cap into the bottle.
- Twist the red cap back to the original position, securely fastening the red cap onto the bottle.
Constitution of the powder
- Shake the bottle vigorously for ten seconds to mix the powders.
- Tap the base of the bottle three times on a hard horizontal surface to make sure all powder is in the bottle and not in the cap.
- Remove the red cap from the bottle.
- Add 64ml of water by using a suitable measuring device up to the line on the label.
- Securely fasten the red cap onto the bottle and shake vigorously for 30 seconds.
Placement of syringe adaptor
- Remove the red cap and red ring and throw away.
- Insert the colourless, transparent Bottle Adaptor and replace the red cap with the grey plastic screw-cap.
- Leave for fifteen minutes for product to reach final consistency.
The reconstituted suspension will be a white/off-white/brownish suspension. It may contain dark specks due to the sweetener.
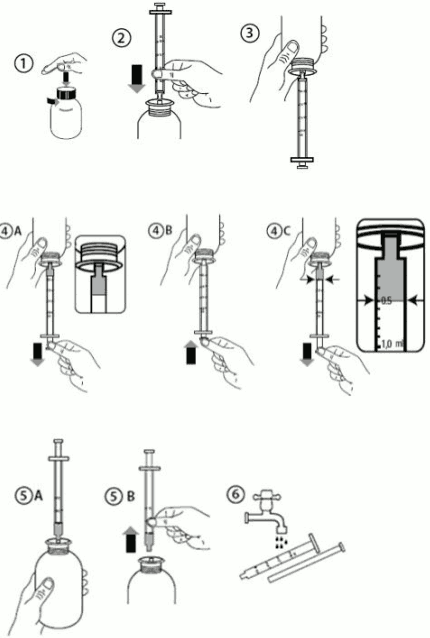
Measuring your dose
Instructions for use of the syringe
- Shake for 20 seconds immediately prior to each use
- To open the bottle, press the grey cap down and turn it anti-clockwise (Figure 1). Do not remove the white cap portion.
- Take the syringe and put it into the adaptor opening (Figure 2).
- Turn the bottle upside down (Figure 3).
- Fill the syringe with a small amount of suspension by pulling the plunger down (Figure 4A). Then push the plunger upward in order to remove any possible bubbles (Figure 4B). Finally, pull the plunger down to the graduation mark corresponding to the quantity in millilitres (ml) prescribed by your doctor. The top flat edge of the piston should be in line with the graduation mark you are measuring to (Figure 4C).
- Turn the bottle the right way up (Figure 5A).
- Remove the syringe from the adaptor (Figure 5B).
- Put the end of the syringe into the mouth of the patient and push the plunger slowly back in to take the medicine. The suspension will be released slowly while the last portion will be released faster due to reduced resistance in the tip of the syringe.
- Wash the syringe with water and let it dry before you use it again (Figure 6).
- Close the bottle with the grey plastic screw cap - leave the bottle adaptor in the bottle.
Note: It is normal to have the red plastic disc in the suspension during use; do not attempt to remove it.
Instruction for administration via nasogastric (NG) or percutaneous endoscopic gastrostomy (PEG) tubes
Ensure that the enteral feeding tube is free from obstruction before administration.
- Flush the enteral tube with 5 mL of water
- Administer the required dose of Omeprazole Oral Suspension with a suitable measuring device.
- Flush the enteral tube with 5 mL of water
This product is compatible for use with Polyurethane and PVC nasogastric (NG) and percutaneous endoscopic gastrostomy (PEG) tubes of size 6 Fr to 16 Fr. For the smallest diameter tubes (6 Fr) a smaller flush volume of 2 ml may be used to support the use in very young children where fluid intake restriction may be of relevance.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.