PREMARIN Coated tablet Ref.[8089] Active ingredients: Estrogens, conjugated
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2016 Publisher: Pfizer Limited, Ramsgate Road, Sandwich, Kent, CT13 9NJ, United Kingdom
Pharmacodynamic properties
ATC Code: G03C A57
Conjugated Estrogens
The active ingredients are primarily the sulfate esters of estrone, equilin sulfates, 17α-estradiol and 17β-estradiol. These substitute for the loss of estrogen production in menopausal women, and alleviate menopausal symptoms. Estrogens prevent bone loss following menopause or ovariectomy.
Mechanism of Action
Endogenous estrogens are largely responsible for the development and maintenance of the female reproductive system and secondary sexual characteristics. Although circulating estrogens exist in a dynamic equilibrium of metabolic interconversions, estradiol is the principal intracellular human estrogen and is substantially more potent than its metabolites, estrone and estriol, at the receptor level.
The primary source of estrogen in normally cycling adult women is the ovarian follicle, which secretes 70 to 500 mcg of estradiol daily, depending on the phase of the menstrual cycle. After menopause, most endogenous estrogen is produced by conversion of androstenedione, which is secreted by the adrenal cortex, to estrone in the peripheral tissues. Thus, estrone and the sulfate-conjugated form, estrone sulfate, are the most abundant circulating estrogens in postmenopausal women.
Estrogens act through binding to nuclear receptors in estrogen-responsive tissues. To date, two estrogen receptors have been identified. These vary in proportion from tissue to tissue. Circulating estrogens modulate the pituitary secretion of the gonadotropins, luteinizing hormone (LH) and follicle stimulating hormone (FSH), through a negative feedback mechanism. Estrogens act to reduce the elevated levels of these gonadotropins seen in postmenopausal women.
Effects on estrogen-deficiency (vasomotor) symptoms
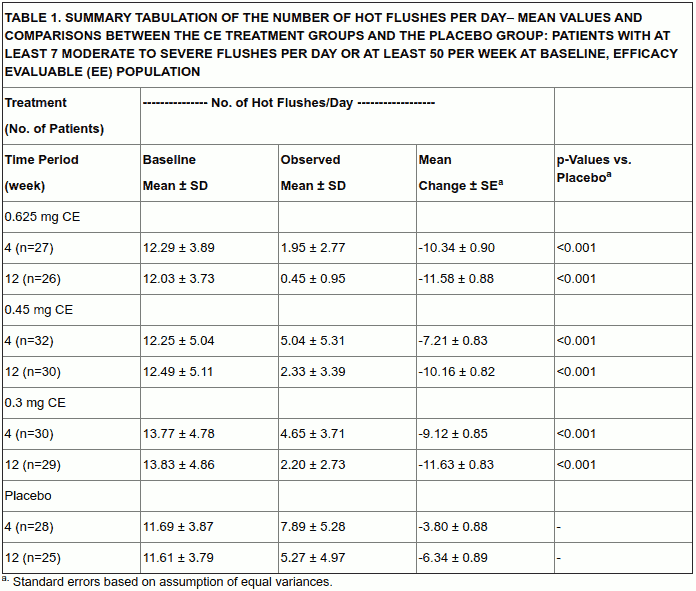
In the first year of the Health and Osteoporosis, Progestin and Estrogen (HOPE) Study, a total of 2,805 postmenopausal women (average age 53.3 ± 4.9 years) were randomly assigned to one of eight treatment groups, receiving either placebo or conjugated estrogens, with or without medroxyprogesterone acetate. Efficacy for vasomotor symptoms was assessed during the first 12 weeks of treatment in a subset of symptomatic women (n = 241) who had at least seven moderate-to-severe hot flushes daily, or at least 50 moderate-to-severe hot flushes during the week before randomization. With conjugated estrogen (0.3 mg, 0.45 mg, and 0.625 mg tablets), the decrease of both the frequency and severity of moderate-to-severe vasomotor symptoms was shown to be statistically improved compared with placebo at weeks 4 and 12.
Table 1 shows the observed mean number of hot flushes in the CE 0.3 mg, 0.45 mg, and 0.625 mg and placebo treatment groups over the initial 12-week period.
Prevention of osteoporosis
At present there is no established screening programme for determining women at risk of developing osteoporotic fracture. Epidemiological studies suggest a number of individual risk factors which contribute to the development of postmenopausal osteoporosis. These include: early menopause; family history of osteoporosis; thin, small frame; cigarette use; recent prolonged systemic corticosteroid use.
Estrogen deficiency at menopause is associated with an increasing bone turnover and decline in bone mass. The effect of estrogens on the bone mineral density is dose-dependent. Protection appears to be effective for as long as treatment is continued. After discontinuation of HRT, bone mass is lost at a rate similar to that in untreated women.
Evidence from the WHI trial and meta-analysed trials shows that current use of HRT, alone or in combination with a progestogen–given to predominantly healthy women–reduces the risk of hip, vertebral and other osteoporotic fractures. HRT may also help prevent fractures in women with low bone density and/or established osteoporosis, but the evidence for that is limited.
Effect on bone mineral density
Health and Osteoporosis, Progestin and Estrogen (HOPE) Study
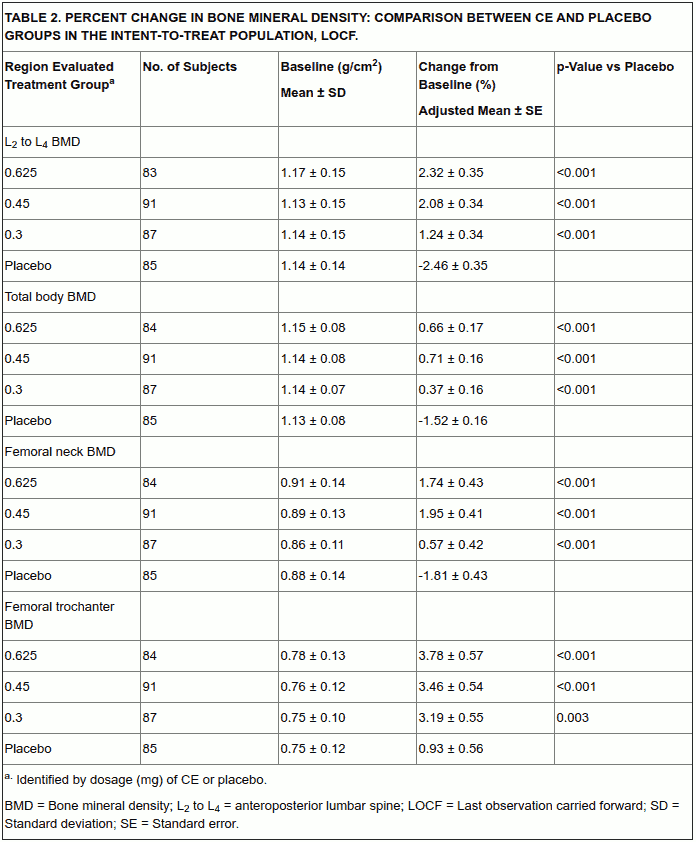
The HOPE study was a double-blind, randomized, placebo/active-drug-controlled, multicenter study of healthy postmenopausal women with an intact uterus. Subjects (mean age 53.3 ± 4.9 years) were 2.3 ± 0.9 years on average since menopause and took one 600 mg tablet of elemental calcium (Caltrate) daily. Subjects were not given Vitamin D supplements. They were treated with conjugated estrogen 0.625 mg, 0.45 mg, 0.3 mg, or placebo. Prevention of bone loss was assessed by measurement of bone mineral density (BMD), primarily at the anteroposterior lumbar spine (L2 to L4). Secondarily, BMD measurements of the total body, femoral neck, and trochanter were also analyzed. Serum osteocalcin, urinary calcium, and N telopeptide were used as bone turnover markers (BTM) at cycles 6, 13, 19, and 26.
Intent-to-treat subjects
All active treatment groups showed significant differences from placebo in each of the four BMD endpoints at cycles 6, 13, 19, and 26. The percent changes from baseline to final evaluation are shown in Table 2.
The bone turnover markers serum osteocalcin and urinary N-telopeptide significantly decreased (p < 0.001) in all active-treatment groups at cycles 6, 13, 19, and 26 compared with the placebo group. Larger mean decreases from baseline were seen with the active groups than with the placebo group. Significant differences from placebo were seen less frequently in urine calcium.
WHI Estrogen-Alone Substudy
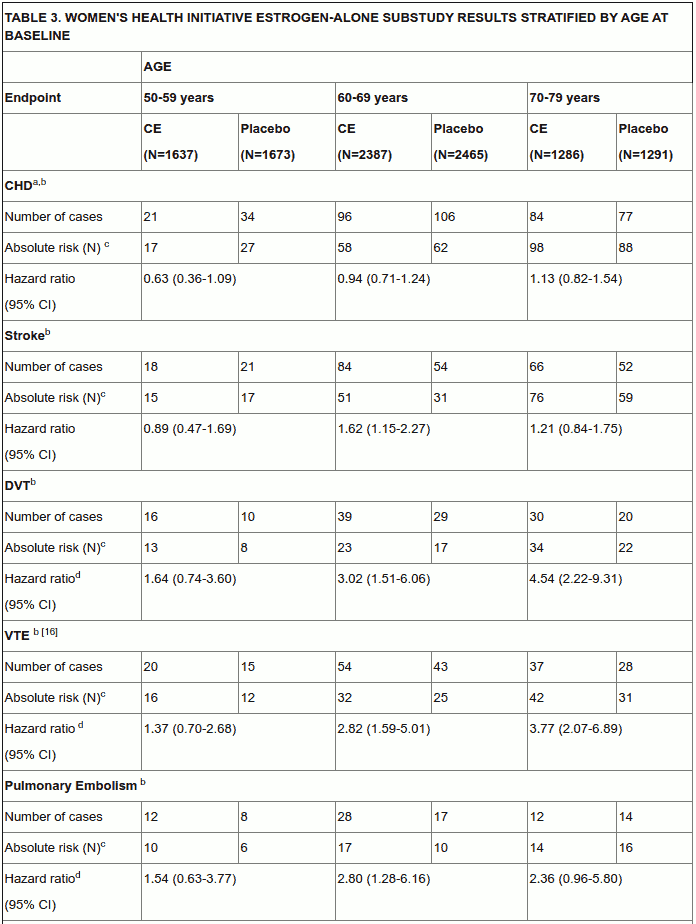
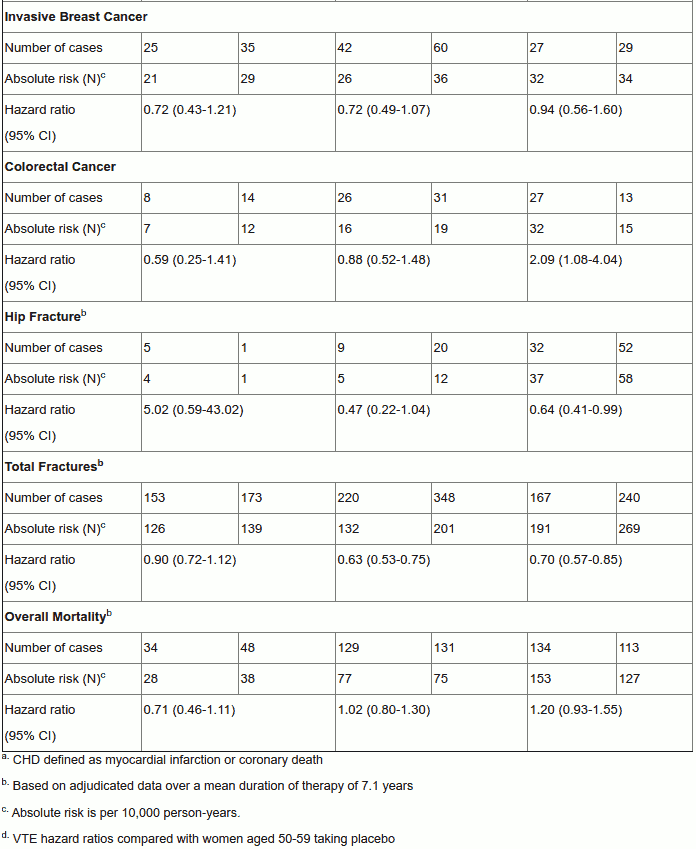
Timing of the initiation of estrogen therapy relative to the start of menopause may affect the overall risk benefit profile. The WHI estrogen-alone substudy stratified by age showed in women 50-59 years of age, a non-significant trend towards reduced risk for CHD and overall mortality compared with placebo in women who initiated hormone therapy closer to menopause than those initiating therapy more distant from menopause.
Table 3 describes the primary results of the Estrogen-alone substudy stratified by age at baseline.
Pharmacokinetic properties
Absorption
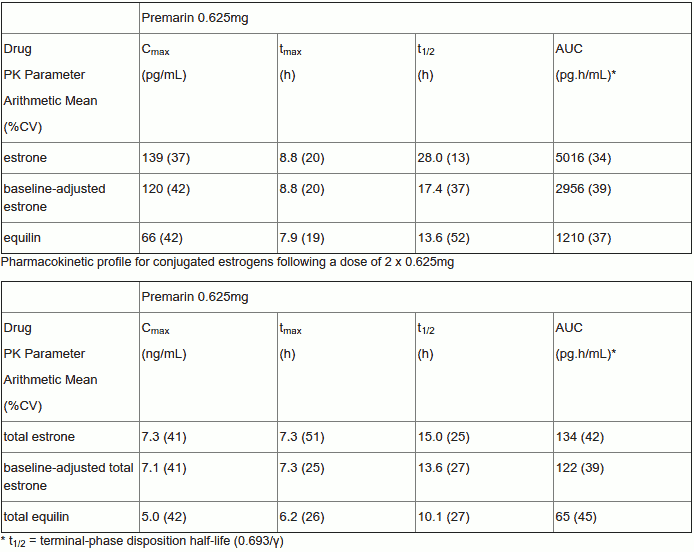
Conjugated estrogens are soluble in water and are well absorbed from the gastrointestinal tract after release from the drug formulation. Premarin tablets release conjugated estrogens slowly over several hours. Maximum plasma concentrations are achieved approximately 6-10 hours following administration. The estrogens are generally eliminated in near-parallel fashion, with half-lives ranging from 10-20 hours, when corrected for endogenous concentrations as needed.
The pharmacodynamic profile of unconjugated and conjugated estrogens following a dose of 2 x 0.625mg is provided in Table 1.
Table 1. Pharmacokinetic parameters for Premarin:
Pharmacokinetic profile for unconjugated estrogens following a 2 x 0.625mg
Distribution
The distribution of exogenous estrogens is similar to that of endogenous estrogens. Estrogens are widely distributed in the body and are generally found in higher concentrations in the sex hormone target organs. Estrogens circulate in the blood largely bound to sex hormone binding globulin (SHBG) and albumin.
Biotransformation
Exogenous estrogens are metabolised in the same manner as endogenous estrogens. Circulating estrogens exist in dynamic equilibrium of metabolic interconversions. These transformations take place mainly in the liver. Estradiol is converted reversibly to estrone, and both can be converted to estriol, which is the major urinary metabolite. Estrogens also undergo enterohepatic recirculation via sulfate and glucuronide conjugation in the liver, biliary secretion of conjugates into the intestine, and hydrolysis in the gut following reabsorption. In post-menopausal women a significant proportion of the circulating estrogens exists as sulfate conjugates, especially estrone sulfate, which serves as a circulating reservoir for the formation of more active estrogens.
Elimination
Estriol, estrone and estradiol are excreted in the urine along with glucuronide and sulfate conjugates.
Special Populations
No pharmacokinetic studies were conducted in special populations, including patients with renal or hepatic impairment.
Preclinical safety data
Long-term continuous administration of natural and synthetic estrogens in certain animal species increases the frequency of carcinoma of the breast, cervix, vagina and liver.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.