Source: FDA, National Drug Code (US) Revision Year: 2020
Endogenous estrogens are largely responsible for the development and maintenance of the female reproductive system and secondary sexual characteristics. Although circulating estrogens exist in a dynamic equilibrium of metabolic interconversions, estradiol is the principal intracellular human estrogen and is substantially more potent than its metabolites, estrone and estriol, at the receptor level.
The primary source of estrogen in normally cycling adult women is the ovarian follicle, which secretes 70 to 500 mcg of estradiol daily, depending on the phase of the menstrual cycle. After menopause, most endogenous estrogen is produced by conversion of androstenedione, secreted by the adrenal cortex, to estrone in the peripheral tissues. Thus, estrone and the sulfate-conjugated form, estrone sulfate, are the most abundant circulating estrogens in postmenopausal women.
Estrogens act through binding to nuclear receptors in estrogen-responsive tissues. To date, two estrogen receptors have been identified. These vary in proportion from tissue to tissue.
Circulating estrogens modulate the pituitary secretion of the gonadotropins, luteinizing hormone (LH) and FSH, through a negative feedback mechanism. Estrogens act to reduce the elevated levels of these gonadotropins seen in postmenopausal women.
There are no pharmacodynamic data for PREMARIN.
Conjugated estrogens are water-soluble and are absorbed from the gastrointestinal tract after release from the drug formulation. The PREMARIN tablet releases conjugated estrogens slowly over several hours. Table 2 summarizes the mean pharmacokinetic parameters for unconjugated and conjugated estrogens following administration of 1 × 0.625 mg and 1 × 1.25 mg tablets to healthy postmenopausal women.
Food effect: The pharmacokinetics of PREMARIN 0.45 mg and 1.25 mg tablets were assessed following a single dose with a high-fat breakfast and with fasting administration. The Cmax and AUC of estrogens were altered approximately 3–13%. The changes to Cmax and AUC are not considered clinically meaningful, therefore PREMARIN may be taken without regard to meals.
Table 2. Pharmacokinetic Parameters for Premarin:
| Pharmacokinetic Profile of Unconjugated Estrogens Following a Dose of 1 × 0.625 mg | ||||
|---|---|---|---|---|
| PK Parameter Arithmetic Mean (%CV) | Cmax (pg/mL) | tmax (h) | t1/2 (h) | AUC (pg∙h/mL) |
| Estrone | 87 (33) | 9.6 (33) | 50.7 (35) | 5557 (59) |
| Baseline-adjusted estrone | 64 (42) | 9.6 (33) | 20.2 (40) | 1723 (52) |
| Equilin | 31 (38) | 7.9 (32) | 12.9 (112) | 602 (54) |
| Pharmacokinetic Profile of Conjugated Estrogens Following a Dose of 1 × 0.625 mg | ||||
| PK Parameter Arithmetic Mean (%CV) | Cmax (ng/mL) | tmax (h) | t1/2 (h) | AUC (ng∙h/mL) |
| Total Estrone | 2.7 (43) | 6.9 (25) | 26.7 (33) | 75 (52) |
| Baseline-adjusted total estrone | 2.5 (45) | 6.9 (25) | 14.8 (35) | 46 (48) |
| Total Equilin | 1.8 (56) | 5.6 (45) | 11.4 (31) | 27 (56) |
| Pharmacokinetic Profile of Unconjugated Estrogens Following a Dose of 1 × 1.25 mg | ||||
| PK Parameter Arithmetic Mean (%CV) | Cmax (pg/mL) | tmax (h) | t1/2 (h) | AUC (pg∙h/mL) |
| Estrone | 124 (30) | 10.0 (32) | 38.1 (37) | 6332 (44) |
| Baseline-adjusted estrone | 102 (35) | 10.0 (32) | 19.7 (48) | 3159 (53) |
| Equilin | 59 (43) | 8.8 (36) | 10.9 (47) | 1182 (42) |
| Pharmacokinetic Profile of Conjugated Estrogens Following a Dose of 1 × 1.25 mg | ||||
| PK Parameter Arithmetic Mean (%CV) | Cmax (ng/mL) | tmax (h) | t1/2 (h) | AUC (ng∙h/mL) |
| Total Estrone | 4.5 (39) | 8.2 (58) | 26.5 (40) | 109 (46) |
| Baseline-adjusted total estrone | 4.3 (41) | 8.2 (58) | 17.5 (41) | 87 (44) |
| Total equilin | 2.9 (42) | 6.8 (49) | 12.5 (34) | 48 (51) |
The distribution of exogenous estrogens is similar to that of endogenous estrogens. Estrogens are widely distributed in the body and are generally found in higher concentration in the sex hormone target organs. Estrogens circulate in the blood largely bound to sex hormone-binding globulin (SHBG) and albumin.
Exogenous estrogens are metabolized in the same manner as endogenous estrogens. Circulating estrogens exist in a dynamic equilibrium of metabolic interconversions. These transformations take place mainly in the liver. Estradiol is converted reversibly to estrone, and both can be converted to estriol, which is a major urinary metabolite. Estrogens also undergo enterohepatic recirculation via sulfate and glucuronide conjugation in the liver, biliary secretion of conjugates into the intestine, and hydrolysis in the intestine followed by reabsorption. In postmenopausal women, a significant portion of the circulating estrogens exists as sulfate conjugates, especially estrone sulfate, which serves as a circulating reservoir for the formation of more active estrogens.
Estradiol, estrone, and estriol are excreted in the urine, along with glucuronide and sulfate conjugates.
No pharmacokinetic studies were conducted with Premarin in specific populations, including patients with renal or hepatic impairment.
Long-term continuous administration of natural and synthetic estrogens in certain animal species increases the frequency of carcinomas of the breast, uterus, cervix, vagina, testis, and liver.
In the first year of the Health and Osteoporosis, Progestin and Estrogen (HOPE) Study, a total of 2,805 postmenopausal women (average age 53.3 ± 4.9 years) were randomly assigned to one of eight treatment groups of either placebo or conjugated estrogens, with or without medroxyprogesterone acetate. Efficacy for vasomotor symptoms was assessed during the first 12 weeks of treatment in a subset of symptomatic women (n=241) who had at least seven moderate to severe hot flushes daily, or at least 50 moderate to severe hot flushes during the week before randomization. PREMARIN (0.3 mg, 0.45 mg, and 0.625 mg tablets) was shown to be statistically better than placebo at weeks 4 and 12 for relief of both frequency and severity of moderate to severe vasomotor symptoms. Table 3 shows the adjusted mean number of hot flushes in the PREMARIN 0.3 mg, 0.45 mg, and 0.625 mg and placebo groups during the initial 12-week period.
Table 3. Summary Tabulation of the Number of Hot Flushes Per Day – Mean Values and Comparisons Between the Active Treatment Groups and the Placebo Group: Patietns With at Least 7 Moderate to Severe Flushes Per Day or at Least 50 Per Week at Baseline, Last Observation Carried Forward (LOCF):
| Treatment (No. of Patients) | No. of Hot Flushes/Day | |||
|---|---|---|---|---|
| Time Period (week) | Baseline Mean ± SD | Observed Mean ± SD | Mean Change ± SD | p-Values vs Placebo* |
| 0.625 mg CE (n=27) | ||||
| 4 | 12.29 ± 3.89 | 1.95 ± 2.77 | -10.34 ± 4.73 | <0.001 |
| 12 | 12.29 ± 3.89 | 0.75 ± 1.82 | -11.54 ± 4.62 | <0.001 |
| 0.45 mg CE (n=32) | ||||
| 4 | 12.25 ± 5.04 | 5.04 ± 5.31 | -7.21 ± 4.75 | <0.001 |
| 12 | 12.25 ± 5.04 | 2.32 ± 3.32 | -9.93 ± 4.64 | <0.001 |
| 0.3 mg CE (n=30) | ||||
| 4 | 13.77 ± 4.78 | 4.65 ± 3.71 | -9.12 ± 4.71 | <0.001 |
| 12 | 13.77 ± 4.78 | 2.52 ± 3.23 | -11.25 ± 4.60 | <0.001 |
| Placebo (n=28) | ||||
| 4 | 11.69 ± 3.87 | 7.89 ± 5.28 | -3.80 ± 4.71 | - |
| 12 | 11.69 ± 3.87 | 5.71 ± 5.22 | -5.98 ± 4.60 | - |
* Based on analysis of covariance with treatment as factor and baseline as covariate.
Results of vaginal maturation indexes at cycles 6 and 13 showed that the differences from placebo were statistically significant (p<0.001) for all treatment groups. (conjugated estrogens alone and conjugated estrogens/medroxyprogesterone acetate treatment groups).
The HOPE study was a double-blind, randomized, placebo/active-drug-controlled, multicenter study of healthy postmenopausal women with an intact uterus. Subjects (mean age 53.3 ± 4.9 years) were 2.3 ± 0.9 years on average since menopause and took one 600 mg tablet of elemental calcium (Caltrate) daily. Subjects were not given Vitamin D supplements. They were treated with PREMARIN 0.625 mg, 0.45 mg, 0.3 mg, or placebo. Prevention of bone loss was assessed by measurement of bone mineral density (BMD), primarily at the anteroposterior lumbar spine (L2 to L4). Secondarily, BMD measurements of the total body, femoral neck, and trochanter were also analyzed. Serum osteocalcin, urinary calcium, and N-telopeptide were used as bone turnover markers (BTM) at cycles 6, 13, 19, and 26.
All active treatment groups showed significant differences from placebo in each of the four BMD endpoints at cycles 6, 13, 19, and 26. The mean percent increases in the primary efficacy measure (L2 to L4 BMD) at the final on-therapy evaluation (cycle 26 for those who completed and the last available evaluation for those who discontinued early) were 2.46 percent with 0.625 mg, 2.26 percent with 0.45 mg, and 1.13 percent with 0.3 mg. The placebo group showed a mean percent decrease from baseline at the final evaluation of 2.45 percent. These results show that the lower dosages of PREMARIN were effective in increasing L2 to L4 BMD compared with placebo, and therefore support the efficacy of the lower doses.
The analysis for the other three BMD endpoints yielded mean percent changes from baseline in femoral trochanter that were generally larger than those seen for L2 to L4, and changes in femoral neck and total body that were generally smaller than those seen for L2 to L4. Significant differences between groups indicated that each of the PREMARIN treatments was more effective than placebo for all three of these additional BMD endpoints. With regard to femoral neck and total body, the active treatment groups all showed mean percent increases in BMD, while placebo treatment was accompanied by mean percent decreases. For femoral trochanter, each of the PREMARIN dose groups showed a mean percent increase that was significantly greater than the small increase seen in the placebo group. The percent changes from baseline to final evaluation are shown in Table 4.
Table 4. Percent Change in Bone Mineral Density: Comparison Between Active and Placebo Groups in the Intent-to-Treat Population, LOCF:
| Region Evaluated Treatment Group* | No. of Subjects | Baseline (g/cm²) Mean ± SD | Change from Baseline (%) Adjusted Mean ± SE | p-Value vs. Placebo |
|---|---|---|---|---|
| L2 to L4 BMD | ||||
| 0.625 | 83 | 1.17 ± 0.15 | 2.46 ± 0.37 | <0.001 |
| 0.45 | 91 | 1.13 ± 0.15 | 2.26 ± 0.35 | <0.001 |
| 0.3 | 87 | 1.14 ± 0.15 | 1.13 ± 0.36 | <0.001 |
| Placebo | 85 | 1.14 ± 0.14 | -2.45 ± 0.36 | |
| Total Body BMD | ||||
| 0.625 | 84 | 1.15 ± 0.08 | 0.68 ± 0.17 | <0.001 |
| 0.45 | 91 | 1.14 ± 0.08 | 0.74 ± 0.16 | <0.001 |
| 0.3 | 87 | 1.14 ± 0.07 | 0.40 ± 0.17 | <0.001 |
| Placebo | 85 | 1.13 ± 0.08 | -1.50 ± 0.17 | |
| Femoral Neck BMD | ||||
| 0.625 | 84 | 0.91 ± 0.14 | 1.82 ± 0.45 | <0.001 |
| 0.45 | 91 | 0.89 ± 0.13 | 1.84 ± 0.44 | <0.001 |
| 0.3 | 87 | 0.86 ± 0.11 | 0.62 ± 0.45 | <0.001 |
| Placebo | 85 | 0.88 ± 0.14 | -1.72 ± 0.45 | |
| Femoral Trochanter BMD | ||||
| 0.625 | 84 | 0.78 ± 0.13 | 3.82 ± 0.58 | <0.001 |
| 0.45 | 91 | 0.76 ± 0.12 | 3.16 ± 0.56 | 0.003 |
| 0.3 | 87 | 0.75 ± 0.10 | 3.05 ± 0.57 | 0.005 |
| Placebo | 85 | 0.75 ± 0.12 | 0.81 ± 0.58 | |
* Identified by dosage (mg) of PREMARIN or placebo.
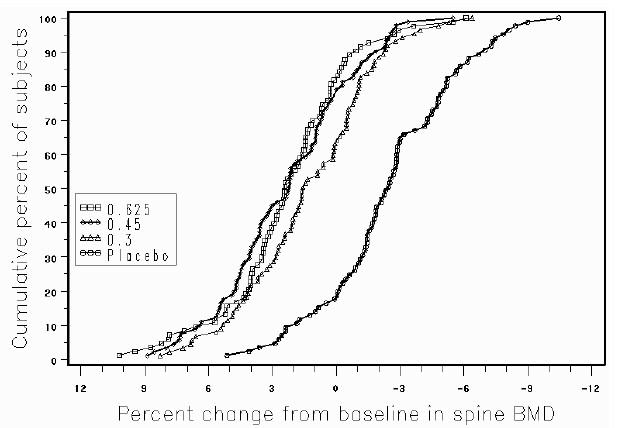
Figure 1 shows the cumulative percentage of subjects with changes from baseline equal to or greater than the value shown on the x-axis.
Figure 1. Cumulative Percent of Subjects With Changes From Baseline in Spine BMD of Given Magnitude or Greater in Premarin and Placebo Groups:
The mean percent changes from baseline in L2 to L4 BMD for women who completed the bone density study are shown with standard error bars by treatment group in Figure 2. Significant differences between each of the PREMARIN dosage groups and placebo were found at cycles 6, 13, 19, and 26.
Figure 2. Adjusted Mean (SE) Percent Change from Baseline at Each Cycle in Spine BMD: Subjects Completing in Premarin Groups and Placebo:
The bone turnover markers, serum osteocalcin and urinary N-telopeptide, significantly decreased (p<0.001) in all active-treatment groups at cycles 6, 13, 19, and 26 compared with the placebo group. Larger mean decreases from baseline were seen with the active groups than with the placebo group. Significant differences from placebo were seen less frequently in urine calcium.
In clinical studies of delayed puberty due to female hypogonadism, breast development was induced by doses as low as 0.15 mg. The dosage may be gradually titrated upward at 6-to 12 month intervals as needed to achieve appropriate bone age advancement and eventual epiphyseal closure. Clinical studies suggest that doses of 0.15 mg, 0.3 mg, and 0.6 mg are associated with mean ratios of bone age advancement to chronological age progression (ΔBA/ΔCA) of 1.1, 1.5, and 2.1, respectively. (PREMARIN in the dose strength of 0.15 mg is not available commercially). Available data suggest that chronic dosing with 0.625 mg is sufficient to induce artificial cyclic menses with sequential progestin treatment and to maintain bone mineral density after skeletal maturity is achieved.
The WHI enrolled approximately 27,000 predominantly healthy postmenopausal women in two substudies to assess the risks and benefits of daily oral CE (0.625 mg)-alone or in combination with MPA (2.5 mg) compared to placebo in the prevention of certain chronic diseases. The primary endpoint was the incidence of CHD (defined as nonfatal MI, silent MI and CHD death), with invasive breast cancer as the primary adverse outcome. A “global index” included the earliest occurrence of CHD, invasive breast cancer, stroke, PE, endometrial cancer (only in the CE plus MPA substudy), colorectal cancer, hip fracture, or death due to other causes. These substudies did not evaluate the effects of CE-alone or CE plus MPA on menopausal symptoms.
The WHI estrogen-alone substudy was stopped early because an increased risk of stroke was observed, and it was deemed that no further information would be obtained regarding the risks and benefits of estrogen alone in predetermined primary endpoints.
Results of the estrogen-alone substudy, which included 10,739 women (average 63 years of age, range 50 to 79; 75.3 percent White, 15.1 percent Black, 6.1 percent Hispanic, 3.6 percent Other) after an average follow-up of 7.1 years, are presented in Table 5.
Table 5. Relative and Absolute Risk Seen in the Estrogen Alone Substudy of WHI:
| Event | Relative Risk CE vs. Placebo | CE n=5,310 | Placebo n=5,429 |
|---|---|---|---|
| (95% nCI†) | Absolute Risk per 10,000 Women-Years | ||
| CHD events‡ | 0.95 (0.78–1.16) | 54 | 57 |
| Non-fatal MI‡ | 0.91 (0.73–1.14) | 40 | 43 |
| CHD death‡ | 1.01 (0.71–1.43) | 16 | 16 |
| All Stroke‡ | 1.33 (1.05–1.68) | 45 | 33 |
| Ischemic stroke‡ | 1.55 (1.19–2.01) | 38 | 25 |
| Deep vein thrombosis‡,§ | 1.47 (1.06–2.06) | 23 | 15 |
| Pulmonary embolism‡ | 1.37 (0.90–2.07) | 14 | 10 |
| Invasive breast cancer‡ | 0.80 (0.62–1.04) | 28 | 34 |
| Colorectal cancer¶ | 1.08 (0.75–1.55) | 17 | 16 |
| Hip fracture‡ | 0.65 (0.45–0.94) | 12 | 19 |
| Vertebral fractures‡,§ | 0.64 (0.44–0.93) | 11 | 18 |
| Lower arm/wrist fractures‡,§ | 0.58 (0.47–0.72) | 35 | 59 |
| Total fractures‡,§ | 0.71 (0.64–0.80) | 144 | 197 |
| Death due to other causes¶,# | 1.08 (0.88–1.32) | 53 | 50 |
| Overall mortality‡,§ | 1.04 (0.88–1.22) | 79 | 75 |
| Global IndexÞ | 1.02 (0.92–1.13) | 206 | 201 |
* Adapted from numerous WHI publications. WHI publications can be viewed at www.nhlbi.nih.gov/whi.
† Nominal confidence intervals unadjusted for multiple looks and multiple comparisons.
‡ Results are based on centrally adjudicated data for an average follow-up of 7.1 years.
§ Not included in “global index”.
¶ Results are based on an average follow-up of 6.8 years.
# All deaths, except from breast or colorectal cancer, definite/probable CHD, PE or cerebrovascular disease.
Þ A subset of the events was combined in a “global index” defined as the earliest occurrence of CHD events, invasive breast cancer, stroke, pulmonary embolism, colorectal cancer, hip fracture, or death due to other causes.
For those outcomes included in the WHI “global index” that reached statistical significance, the absolute excess risk per 10,000 women-years in the group treated with CE-alone was 12 more strokes while the absolute risk reduction per 10,000 women-years was 7 fewer hip fractures. 9 The absolute excess risk of events included in the “global index” was a non-significant 5 events per 10,000 women-years. There was no difference between the groups in terms of all-cause mortality.
No overall difference for primary CHD events (nonfatal MI, silent MI and CHD death) and invasive breast cancer incidence in women receiving CE-alone compared with placebo was reported in final centrally adjudicated results from the estrogen-alone substudy, after an average follow up of 7.1 years. See Table 5.
Centrally adjudicated results for stroke events from the estrogen-alone substudy, after an average follow-up of 7.1 years, reported no significant difference in distribution of stroke subtype or severity, including fatal strokes, in women receiving CE-alone compared to placebo. Estrogen-alone increased the risk for ischemic stroke, and this excess risk was present in all subgroups of women examined. 10
Timing of the initiation of estrogen-alone therapy relative to the start of menopause may affect the overall risk benefit profile. The WHI estrogen-alone substudy stratified by age showed in women 50–59 years of age, a non-significant trend toward reduced risk for CHD [hazard ratio (HR) 0.63 (95 percent CI 0.36–1.09)] and overall mortality [HR 0.71 (95 percent CI 0.46–1.11)].
The WHI estrogen plus progestin substudy was stopped early. According to the predefined stopping rule, after an average follow-up of 5.6 years of treatment, the increased risk of invasive breast cancer and cardiovascular events exceeded the specified benefits included in the “global index.” The absolute excess risk of events included in the “global index” was 19 per 10,000 women-years.
For those outcomes included in the WHI “global index” that reached statistical significance after 5.6 years of follow-up, the absolute excess risks per 10,000 women-years in the group treated with CE plus MPA were 7 more CHD events, 8 more strokes, 10 more PEs, and 8 more invasive breast cancers, while the absolute risk reductions per 10,000 women-years were 6 fewer colorectal cancers and 5 fewer hip fractures.
Results of the estrogen plus progestin substudy, which included 16,608 women (average 63 years of age, range 50 to 79; 83.9 percent White, 6.8 percent Black, 5.4 percent Hispanic, 3.9 percent Other) are presented in Table 6. These results reflect centrally adjudicated data after an average follow-up of 5.6 years.
Table 6. Relative and Absolute Risk Seen in the Estrogen Plus Progestin Substudy of WHI at an Average of 5.6 Years*,†:
| Relative Risk CE/MPA vs. Placebo | CE/MPA n=8,506 | Placebo n=8,102 | |
|---|---|---|---|
| Event | (95% nCI‡) | Absolute Risk per 10,000 Women-Years | |
| CHD events | 1.23 (0.99–1.53) | 41 | 34 |
| Non-fatal MI | 1.28 (1.00–1.63) | 31 | 25 |
| CHD death | 1.10 (0.70–1.75) | 8 | 8 |
| All Strokes | 1.31 (1.03–1.68) | 33 | 25 |
| Ischemic stroke | 1.44 (1.09–1.90) | 26 | 18 |
| Deep vein thrombosis§ | 1.95 (1.43–2.67) | 26 | 13 |
| Pulmonary embolism | 2.13 (1.45–3.11) | 18 | 8 |
| Invasive breast cancer¶ | 1.24 (1.01–1.54) | 41 | 33 |
| Colorectal cancer | 0.61 (0.42–0.87) | 10 | 16 |
| Endometrial cancer§ | 0.81 (0.48–1.36) | 6 | 7 |
| Cervical cancer§ | 1.44 (0.47–4.42) | 2 | 1 |
| Hip fracture | 0.67 (0.47–0.96) | 11 | 16 |
| Vertebral fractures§ | 0.65 (0.46–0.92) | 11 | 17 |
| Lower arm/wrist fractures§ | 0.71 (0.59–0.85) | 44 | 62 |
| Total fractures§ | 0.76 (0.69–0.83) | 152 | 199 |
| Overall Mortality# | 1.00 (0.83–1.19) | 52 | 52 |
| Global IndexÞ | 1.13 (1.02–1.25) | 184 | 165 |
* Adapted from numerous WHI publications. WHI publications can be viewed at www.nhlbi.nih.gov/whi.
† Results are based on centrally adjudicated data.
‡ Nominal confidence intervals unadjusted for multiple looks and multiple comparisons.
§ Not included in "global index."
¶ Includes metastatic and non-metastatic breast cancer, with the exception of in situ cancer.
# All deaths, except from breast or colorectal cancer, definite or probable CHD, PE or cerebrovascular disease.
Þ A subset of the events was combined in a “global index” defined as the earliest occurrence of CHD events, invasive breast cancer, stroke, pulmonary embolism, colorectal cancer, hip fracture, or death due to other causes.
Timing of the initiation of estrogen therapy relative to the start of menopause may affect the overall risk benefit profile. The WHI estrogen plus progestin substudy stratified by age showed in women 50–59 years of age, a non-significant trend toward reduced risk for overall mortality [HR 0.69 (95 percent CI 0.44–1.07)].
The WHIMS estrogen-alone ancillary study of WHI enrolled 2,947 predominantly healthy hysterectomized postmenopausal women 65 to 79 years of age (45 percent were 65 to 69 years of age; 36 percent were 70 to 74 years of age; 19 percent were 75 years of age and older) to evaluate the effects of daily CE (0.625 mg)- alone on the incidence of probable dementia (primary outcome) compared to placebo.
After an average follow-up of 5.2 years, the relative risk of probable dementia for CE-alone versus placebo was 1.49 (95 percent CI 0.83–2.66). The absolute risk of probable dementia for CE-alone versus placebo was 37 versus 25 cases per 10,000 women-years. Probable dementia as defined in this study included Alzheimer’s disease (AD), vascular dementia (VaD) and mixed types (having features of both AD and VaD). The most common classification of probable dementia in the treatment group and the placebo groups was AD. Since the ancillary study was conducted in women 65 to 79 years of age, it is unknown whether these findings apply to younger postmenopausal women [see Warnings and Precautions (5.3), and Use in Specific Populations (8.5)].
The WHIMS estrogen plus progestin ancillary study enrolled 4,532 predominantly healthy postmenopausal women 65 years of age and older (47 percent were 65 to 69 years of age; 35 percent were 70 to 74 years; 18 percent were 75 years of age and older) to evaluate the effects of daily CE (0.625 mg) plus MPA (2.5 mg) on the incidence of probable dementia (primary outcome) compared to placebo.
After an average follow-up of 4 years, the relative risk of probable dementia for CE plus MPA was 2.05 (95 percent CI, 1.21–3.48). The absolute risk of probable dementia for CE (0.625 mg) plus MPA (2.5 mg) versus placebo was 45 versus 22 per 10,000 women-years. Probable dementia as defined in this study included AD, VaD and mixed types (having features of both AD and VaD). The most common classification of probable dementia in both the treatment and placebo groups was AD. Since the ancillary study was conducted in women 65 to 79 years of age, it is unknown whether these findings apply to younger postmenopausal women [see Warnings and Precautions (5.3), and Use in Specific Populations (8.5)].
When data from the two populations were pooled as planned in the WHIMS protocol, the reported overall relative risk for probable dementia was 1.76 (95 percent CI 1.19–2.60). Differences between groups became apparent in the first year of treatment. It is unknown whether these findings apply to younger postmenopausal women [see Warnings and Precautions (5.3), and Use in Specific Populations (8.5)].
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.