Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2021 Publisher: Bayer plc, 400 South Oak Way, Reading, RG2 6AD
Pharmacotherapeutic group: Natural and semisynthetic oestrogens, plain
ATC code: G03CA03
Progynova TS contains synthetic 17ß-estradiol, which is chemically and biologically identical to endogenous human estradiol. It substitutes for the loss of oestrogen production in menopausal women, and alleviates menopausal symptoms. Oestrogens prevent bone loss following menopause or ovariectomy.
Relief of menopausal symptoms was achieved during the first few weeks of treatment.
Oestrogen deficiency at menopause is associated with an increasing bone turnover and decline in bone mass. The effect of oestrogens on the bone mineral density is dose-dependent. However, in clinical trials, the efficacy of Progynova TS 100 was not significantly better than the efficacy of Progynova TS 50 for the prevention of postmenopausal osteoporosis. Protection appears to be effective for as long as treatment is continued. After discontinuation of HRT, bone mass is lost at a rate similar to that in untreated women.
Evidence from the WHI trial and meta-analysed trials shows that current use of HRT alone or in combination with a progestogen – given to predominantly healthy women – reduces the risk of hip, vertebral, and other osteoporotic fractures. HRT may also prevent fractures in women with low bone density and/or established osteoporosis, but the evidence for that is limited.
Two clinical trial studies in osteoporosis prevention have been conducted with Progynova TS, one in the US and one in Europe.
After two years of treatment, the increase in lumbar spine bone mineral density (BMD) was 6.91% (95% confidence interval (CI) 4.90-8.91) and 4.09% (95%-CI 2.01-6.17) in the European and US study, respectively. In the US study, responder rates were also evaluated. The percentage of women who maintained or gained BMD in the lumbar spine zone during treatment was 94%.
Progynova TS 50 also had an effect on femoral neck BMD. The increase after 2 years at the femoral neck was 5.73% (95%-CI 4.25-7.21) and 1.61% (95%-CI 0.09-3.13) in the European and US study, respectively. In the US study, responder rates were also evaluated. The percentage of women who maintained or gained BMD at the femoral neck during treatment was 78%.
After two years of treatment, the increase in lumbar spine (BMD) was 8.43% (95% CI 6.93-9.93) and 4.70% (95%-CI 2.98-6.42) in the European and US study, respectively. In the US study, responder rates were also evaluated. The percentage of women who maintained or gained BMD in the lumbar spine zone during treatment was 90%.
Progynova TS 100 also had an effect on femoral neck BMD. The increase after two years at the femoral neck was 5.63% (95%-CI 3.87-7.38) and 1.53% (95%-CI 0.66-3.72) in the European and US study, respectively. In the US study, responder rates were also evaluated. The percentage of women who maintained or gained BMD at the femoral neck during treatment was 68%.
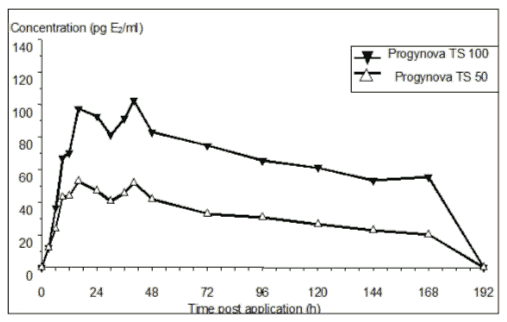
After dermal application of Progynova TS, estradiol is continuously released and transported across intact skin leading to sustained circulating levels of estradiol during a 7-day treatment period as shown in Figure 1. The systemic availability of estradiol after transdermal administration is about 20 times higher than that after oral administration. This difference is due to the absence of first pass metabolism when estradiol is given by the transdermal route. The major pharmacokinetic parameters of estradiol are summarised in the following table:
| Transdermal Delivery System | Daily Delivery Rate, mg/day | Application Site | AUC(0-tlast) ngxh/mL / nmolxh/L | Cmax pg/mL / pmol/L | Cavg pg/mL / pmol/L | tmax h | Cmin pg/mL / pmol/L |
|---|---|---|---|---|---|---|---|
| Progynova TS 50 | 0.050 | Abdomen | 5.44 / 20 | 55 / 202 | 35 / 129 | 26 | 30 / 110 |
| Progynova TS 100 | 0.100 | Abdomen | 11.5 / 42 | 110 / 404 | 70 / 257 | 31 | 56 / 206 |
Figure 1. Mean baseline uncorrected serum 17 β-estradiol concentrations vs. time profile following application of Progynova TS 50 and Progynova TS 100:
The distribution of exogenous oestrogens is similar to that of endogenous oestrogens. The apparent volume of distribution of estradiol after single intravenous administration is about 1 l/kg. Oestrogens circulate in the blood largely bound to serum proteins. About 61% of estradiol is bound non-specifically to serum albumin and about 37% specifically to sex hormone binding globulin (SHBG).
After transdermal administration, the biotransformation of estradiol leads to concentrations of estrone and of the respective conjugates within the range as seen during the early follicular phase in the reproductive life period, indicated by an estradiol/estrone serum level ratio of approximately 1. Unphysiologically high estrone levels as a result of the intensive “first pass” metabolism during oral estradiol hormone replacement therapy, reflected in estradiol/estrone ratios as low as 0.1, are avoided.
The biotransformation of the transdermally administered estradiol is the same as that of the endogenous hormone: Estradiol is mainly metabolized in the liver but also extrahepatically e.g. in gut, kidney, skeletal muscles and target organs. These processes involve the formation of estrone, estriol, catecholoestrogens and sulfate and glucuronide conjugates of these compounds, which are less oestrogenic or even nonoestrogenic.
The total serum clearance of estradiol following single intravenous administration shows high variability in the range of 10-30 ml/min/kg. Estradiol and its metabolites are excreted in the bile and undergo a so-called enterohepatic circulation. Ultimately estradiol and its metabolites are mainly excreted as sulfates and glucuronides with the urine.
Accumulation of estradiol and estrone was not observed following multiple 1-week patch applications. Accordingly, steady-state serum levels of estradiol and estrone correspond to those observed after a single application.
The toxicity profile of estradiol is well known. There are no preclinical data of relevance to the prescriber which are additional to that already included in other sections of the SPC.
In primary dermal irritation studies, application of Progynova TS patches resulted in mild irritation related to mechanical trauma at removal. Progynova TS patches had no dermal sensitising potential.
Studies on the components (adhesive matrix, backing and release liner) did not indicate any risk related to the use of the Progynova TS patch.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.