Source: FDA, National Drug Code (US) Revision Year: 2019
In vitro studies and in vivo pharmacologic studies have demonstrated that albuterol has a preferential effect on beta2-adrenergic receptors compared with isoproterenol. While it is recognized that beta2-adrenergic receptors are the predominant receptors on bronchial smooth muscle, data indicate that there is a population of beta2-receptors in the human heart existing in a concentration between 10% and 50% of cardiac beta-adrenergic receptors. The precise function of these receptors has not been established. (See WARNINGS, Cardiovascular Effects section.)
Activation of beta2-adrenergic receptors on airway smooth muscle leads to the activation of adenylcyclase and to an increase in the intracellular concentration of cyclic-3',5'-adenosine monophosphate (cyclic AMP). This increase of cyclic AMP leads to the activation of protein kinase A, which inhibits the phosphorylation of myosin and lowers intracellular ionic calcium concentrations, resulting in relaxation. Albuterol relaxes the smooth muscles of all airways, from the trachea to the terminal bronchioles. Albuterol acts as a functional antagonist to relax the airway irrespective of the spasmogen involved, thus protecting against all bronchoconstrictor challenges. Increased cyclic AMP concentrations are also associated with the inhibition of release of mediators from mast cells in the airway.
Albuterol has been shown in most clinical trials to have more effect on the respiratory tract, in the form of bronchial smooth muscle relaxation, than isoproterenol at comparable doses while producing fewer cardiovascular effects. Controlled clinical studies and other clinical experience have shown that inhaled albuterol, like other beta-adrenergic agonist drugs, can produce a significant cardiovascular effect in some patients, as measured by pulse rate, blood pressure, symptoms, and/or electrocardiographic changes.
Intravenous studies in rats with albuterol sulfate have demonstrated that albuterol crosses the blood-brain barrier and reaches brain concentrations amounting to approximately 5% of the plasma concentrations. In structures outside the blood-brain barrier (pineal and pituitary glands), albuterol concentrations were found to be 100 times those in the whole brain.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when beta2-agonist and methylxanthines were administered concurrently. The clinical significance of these findings is unknown.
Propellant HFA-134a is devoid of pharmacological activity except at very high doses in animals (380-1300 times the maximum human exposure based on comparisons of AUC values), primarily producing ataxia, tremors, dyspnea, or salivation. These are similar to effects produced by the structurally related chlorofluorocarbons (CFCs), which have been used extensively in metered dose inhalers.
In animals and humans, propellant HFA-134a was found to be rapidly absorbed and rapidly eliminated, with an elimination half-life of 3 to 27 minutes in animals and 5 to 7 minutes in humans. Time to maximum plasma concentration (Tmax) and mean residence time are both extremely short, leading to a transient appearance of HFA-134a in the blood with no evidence of accumulation.
In a single-dose bioavailability study which enrolled six healthy, male volunteers, transient low albuterol levels (close to the lower limit of quantitation) were observed after administration of two puffs from both PROVENTIL HFA Inhalation Aerosol and a CFC 11/12 propelled albuterol inhaler. No formal pharmacokinetic analyses were possible for either treatment, but systemic albuterol levels appeared similar.
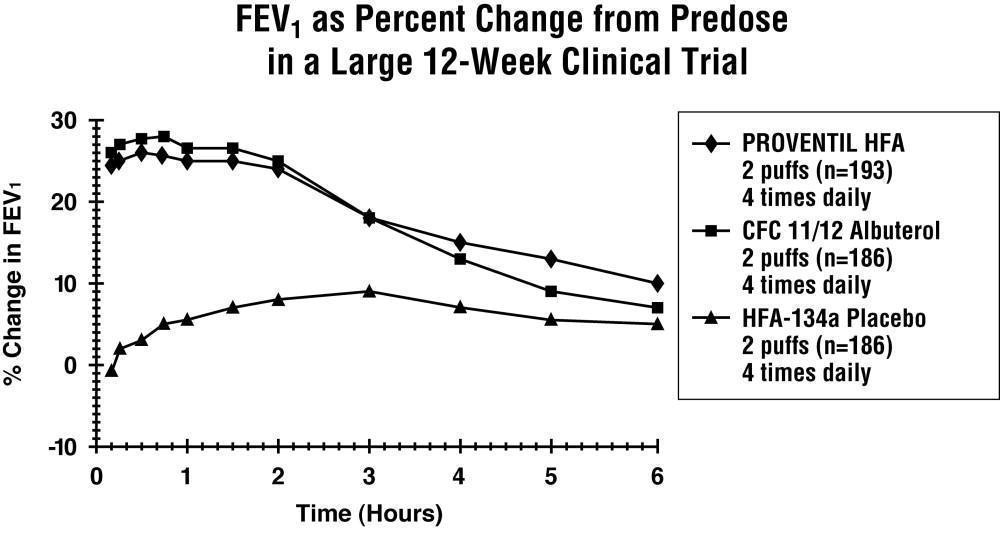
In a 12-week, randomized, double-blind, double-dummy, active- and placebo-controlled trial, 565 patients with asthma were evaluated for the bronchodilator efficacy of PROVENTIL HFA Inhalation Aerosol (193 patients) in comparison to a CFC 11/12 propelled albuterol inhaler (186 patients) and an HFA-134a placebo inhaler (186 patients).
Serial FEV1 measurements (shown below as percent change from test-day baseline) demonstrated that two inhalations of PROVENTIL HFA Inhalation Aerosol produced significantly greater improvement in pulmonary function than placebo and produced outcomes which were clinically comparable to a CFC 11/12 propelled albuterol inhaler.
The mean time to onset of a 15% increase in FEV1 was 6 minutes and the mean time to peak effect was 50 to 55 minutes. The mean duration of effect as measured by a 15% increase in FEV1 was 3 hours. In some patients, duration of effect was as long as 6 hours.
In another clinical study in adults, two inhalations of PROVENTIL HFA Inhalation Aerosol taken 30 minutes before exercise prevented exercise-induced bronchospasm as demonstrated by the maintenance of FEV1 within 80% of baseline values in the majority of patients.
In a 4-week, randomized, open-label trial, 63 children, 4 to 11 years of age, with asthma were evaluated for the bronchodilator efficacy of PROVENTIL HFA Inhalation Aerosol (33 pediatric patients) in comparison to a CFC 11/12 propelled albuterol inhaler (30 pediatric patients).
Serial FEV1 measurements as percent change from test-day baseline demonstrated that two inhalations of PROVENTIL HFA Inhalation Aerosol produced outcomes which were clinically comparable to a CFC 11/12 propelled albuterol inhaler.
The mean time to onset of a 12% increase in FEV1 for PROVENTIL HFA Inhalation Aerosol was 7 minutes and the mean time to peak effect was approximately 50 minutes. The mean duration of effect as measured by a 12% increase in FEV1 was 2.3 hours. In some pediatric patients, duration of effect was as long as 6 hours.
In another clinical study in pediatric patients, two inhalations of PROVENTIL HFA Inhalation Aerosol taken 30 minutes before exercise provided comparable protection against exercise-induced bronchospasm as a CFC 11/12 propelled albuterol inhaler.
In a 2-year study in SPRAGUE-DAWLEY rats, albuterol sulfate caused a dose-related increase in the incidence of benign leiomyomas of the mesovarium at the above dietary doses of 2 mg/kg (approximately 15 times the maximum recommended daily inhalation dose for adults on a mg/m² basis and approximately 6 times the maximum recommended daily inhalation dose for children on a mg/m² basis). In another study this effect was blocked by the coadministration of propranolol, a nonselective beta-adrenergic antagonist. In an 18-month study in CD-1 mice, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 500 mg/kg (approximately 1700 times the maximum recommended daily inhalation dose for adults on a mg/m² basis and approximately 800 times the maximum recommended daily inhalation dose for children on a mg/m² basis). In a 22-month study in Golden Hamsters, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 50 mg/kg (approximately 225 times the maximum recommended daily inhalation dose for adults on a mg/m² basis and approximately 110 times the maximum recommended daily inhalation dose for children on a mg/m² basis).
Albuterol sulfate was not mutagenic in the Ames test or a mutation test in yeast. Albuterol sulfate was not clastogenic in a human peripheral lymphocyte assay or in an AH1 strain mouse micronucleus assay.
Reproduction studies in rats demonstrated no evidence of impaired fertility at oral doses up to 50 mg/kg (approximately 340 times the maximum recommended daily inhalation dose for adults on a mg/m² basis).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.