REDEMPLO Injection for solution Ref.[116088] Active ingredients: Plozasiran
Source: FDA, National Drug Code (US) Revision Year: 2025
12.1. Mechanism of Action
Plozasiran is a siRNA conjugated with GalNAc that degrades the apoC-III mRNA through the RNA interference mechanism resulting in reduced levels of hepatic and serum apoC-III protein. Reduction of apoC-III protein leads to increased clearance of serum triglycerides.
12.2. Pharmacodynamics
In Trial 1 [see Clinical Studies (14)], following the recommended dose of 25 mg administered every 3 months in patients with FCS, REDEMPLO reduced median fasting serum apoC-III protein. The placebo-corrected median percent change in fasting serum apoC-III protein from baseline was -90% at 1 month, -93% at 3 months, -82% at 6 months, -91% at 10 months, and -87% at 12 months.
Cardiac Electrophysiology:
At a dose 4 times the recommended dose of 25 mg administered every 3 months, clinically significant QTc interval prolongation was not observed.
12.3. Pharmacokinetics
REDEMPLO exhibited linear and time-invariant pharmacokinetics following subcutaneous injections within the dose range of 10 mg to 100 mg. The following pharmacokinetic parameters were observed in healthy adults after receiving a 25 mg dose of REDEMPLO.
Absorption
Plozasiran peak plasma concentration (Cmax) is 68.5 ng/mL. The median time to reach Cmax (Tmax) is 6 hours.
Distribution
Plozasiran is 78% protein bound in vitro at the clinically relevant plasma concentrations. Following subcutaneous multiple administration of 25 mg plozasiran, the apparent volume of distribution is approximately 146 L. Plozasiran is distributed in plasma and extracellular body water before its uptake by hepatocytes to decrease apoC-III mRNA expression and reduce serum triglycerides.
Elimination
The terminal elimination half-life of plozasiran in plasma is approximately 3 to 4 hours. The mean apparent systemic clearance is 33.8 L/hour.
Metabolism
Plozasiran is primarily metabolized by nucleases to shorter oligonucleotides of varying lengths.
Excretion
Approximately 16 to 19% of REDEMPLO dose is excreted in urine.
Specific Populations
No clinically significant differences in plozasiran pharmacokinetics based on age, sex, race, mild and moderate renal impairment (eGFR ≥30 to <90 mL/min), or mild hepatic impairment (total bilirubin ≤1 times ULN and AST >1 times ULN, or total bilirubin >1.0 to 1.5 times ULN and any AST) were found in the population pharmacokinetic analysis. The impact of severe renal impairment, end-stage renal impairment, or moderate to severe hepatic impairment is not known.
Drug Interaction Studies
In Vitro Assessment of Drug Interactions
CYP450 Enzymes:
Plozasiran is not a substrate, inhibitor, or inducer of CYP450 enzymes at clinically relevant concentrations.
Transporter Systems:
Plozasiran is not a substrate or an inhibitor of P-gp, BCRP, OAT1, OAT3, OCT1, OCT2, OATP1B1, OATP1B3, MATE1, or MATE2-K.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a 26-week study in RasH2Tg mice, plozasiran was administered subcutaneously once every 8 weeks at dose levels of 30, 60, and 120 mg/kg. Plozasiran was not carcinogenic up to the highest tested dose of 120 mg/kg (23-times MRHD based on BSA).
Mutagenesis
Plozasiran was not mutagenic or clastogenic in a standard battery of genetic toxicity assays, including a bacterial mutation (Ames) assay, and in vitro and in vivo mouse micronucleus assays.
Impairment of Fertility
In a fertility and early embryonic-development study, male and female rats were administered subcutaneously with vehicle or plozasiran at the doses of 12.5, 25 or 50 mg/kg or rat specific surrogate at 25 mg/kg. Males were treated once weekly before and throughout cohabitation, while females received treatment either once every 3 days or once weekly before and through mating until gestation day 6. There were no adverse effects on mating and fertility in males or females up to 50 mg/kg corresponding to 19-times the MRHD, based on BSA.
14. Clinical Studies
The efficacy of REDEMPLO was demonstrated in a randomized, placebo-controlled, double-blind trial in adult patients with genetically confirmed or clinically diagnosed FCS maintained on a low-fat diet(≤20 grams fat per day) (Trial 1; NCT05089084). Patients were randomized to receive four total doses of REDEMPLO 25 mg (n=26) or matching placebo (n=25), injected subcutaneously once every 3 months over a 12-month treatment period
The diagnosis of FCS was based on adults with a screening fasting TG ≥880 mg/dL refractory to lipid-lowering therapy, with a history of elevated triglycerides (in excess of 1,000 mg/dL at least three times), and evidence of FCS by known genotypes, evidence of low lipoprotein lipase activity, or a clinical diagnosis. In this trial, for patients with clinically diagnosed FCS, the inclusion criteria specified at least one of the following: recurrent episodes of acute pancreatitis not caused by alcohol or cholelithiasis; recurrent hospitalizations for severe abdominal pain without other explainable cause; childhood pancreatitis; or family history of hypertriglyceridemia-induced pancreatitis.
Patient demographics were generally similar across the treatment groups [see Adverse Reactions (6.1)]. At enrollment, the percentage of patients with genetic confirmation of FCS was 46% in the REDEMPLO 25 mg group compared with 56% in the placebo group; diabetes was 15% in the REDEMPLO 25 mg group compared with 32% in the placebo group; and a history of documented acute pancreatitis in the prior 5 years was 54% in the REDEMPLO 25 mg group compared with 68% in the placebo group. Patients in the REDEMPLO 25 mg and placebo groups were treated with statins (43%), omega-3 fatty acids (29%), fibrates (69%), or no background TG lowering therapies (25%) at study entry. Mean (SD) and median fasting TG levels at baseline were 2,311 (1,258) mg/dL and 2,030 mg/dL, respectively (range of 747 to 5,596 mg/dL).
The primary efficacy endpoint was percent change in fasting triglycerides from baseline at Month 10 (average of 2 assessments, 2 to 7 days apart). The median difference between REDEMPLO 25 mg and the placebo group in percent change in fasting triglyceride levels from baseline to Month 10 was -58.7% (95% CI: -89.6, -27.9; p<0.0001). For additional results see Table 2.
Table 2. Baseline and Percent Changes from Baseline in Lipid/Lipoprotein Parameters in Patients with FCS at Month 10 in Trial 1:
| REDEMPLO 25 mg N=26 | Placebo (pooled) N=25 | REDEMPLO 25 mg vs. Placebo | |||
| Parameter (mg/dL) | BL | % change at Month 10 | BL | % change at Month 10 | Treatment Difference % change (95% CI) at Month 10 |
| Triglyceridesb b | 2008 | -80 | 2053 | -17 | -59 a (-90, -28) |
| Non-HDL-Cc | 279 | -39 | 268 | 4 | -42 (-67, -18) |
| LDL-Cc | 24 | 112 | 28 | 20 | 92 (4, 180) |
| Total ApoBc | 72 | 27 | 79 | 12 | 15 (-16, 46) |
| ApoB-48c | 10 | -61 | 11 | 45 | -106 (-180, -33) |
Abbreviations: ApoB = apolipoprotein B; CI = confidence interval; BL = baseline; FCS = familial chylomicronemia syndrome; non-HDL-C = non-high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol.
a Reached statistical significance (p value ˂ 0.0001).
b Median; Hodges-Lehmann method was used to estimate the median difference (location shift) and its corresponding 95% confidence interval for percent changes. Missing data were imputed using washout imputation.
c Mean; Analysis of covariance (ANCOVA) model was used to estimate the mean difference and its corresponding 95% confidence interval for percent changes. Missing data were imputed using washout imputation.
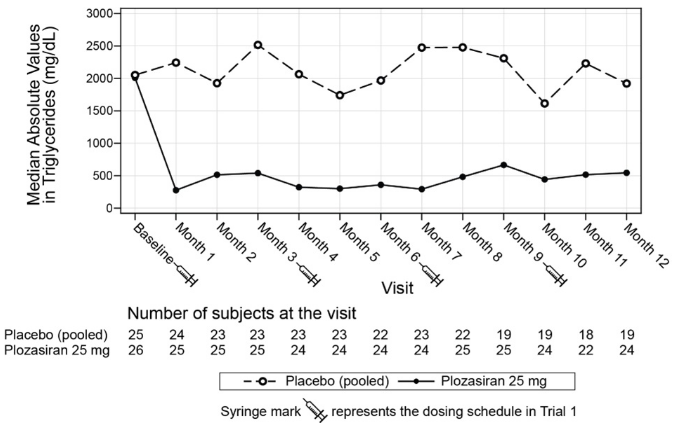
Median percent change in TG from baseline (Figure 1) and median absolute TG values (Figure 2) over time demonstrated a consistent lowering effect during the 12-month treatment period.
Figure 1. Median Percent Change from Baseline in Fasting Triglycerides Over Time in Trial 1:
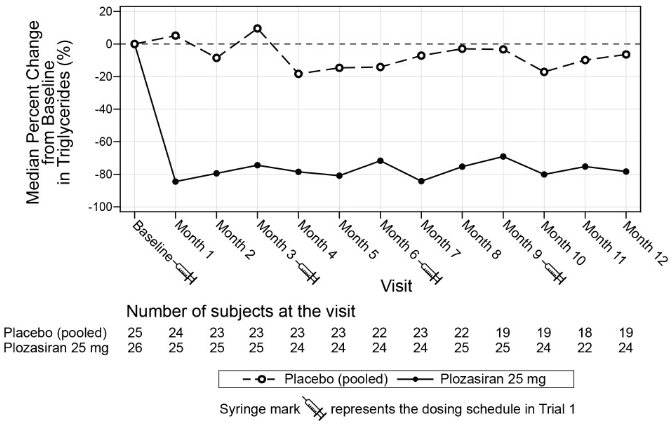
Figure 2. Median Absolute Fasting Triglyceride Levels (mg/dL) in Trial 1:
Over the 12-month treatment period, the numerical incidence of acute pancreatitis in patients treated with REDEMPLO 25 mg was lower compared with placebo [2 (8%) patients in the REDEMPLO 25 mg group compared with 5 (20%) patients in the placebo group].
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.