REYATAZ Hard capsule Ref.[6232] Active ingredients: Atazanavir
Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: BRISTOL-MYERS SQUIBB PHARMA EEIG, Uxbridge Business Park, Sanderson Road, Uxbridge UB8 1DH, United Kingdom
Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
REYATAZ is contraindicated in patients with severe hepatic insufficiency (see sections 4.2, 4.4 and 5.2). REYATAZ with ritonavir is contraindicated in patients with moderate hepatic insufficiency (see sections 4.2, 4.4 and 5.2).
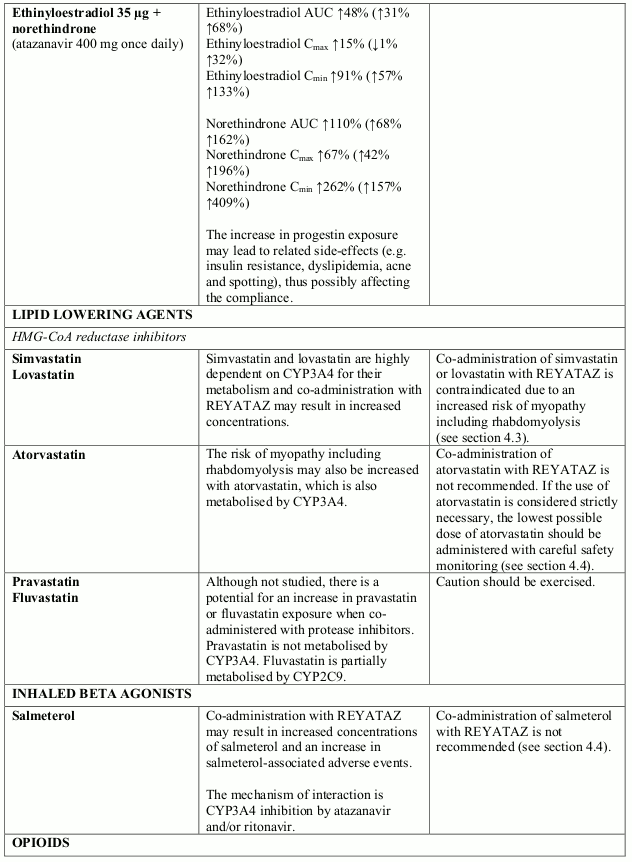
Co-administration with simvastatin or lovastatin (see section 4.5).
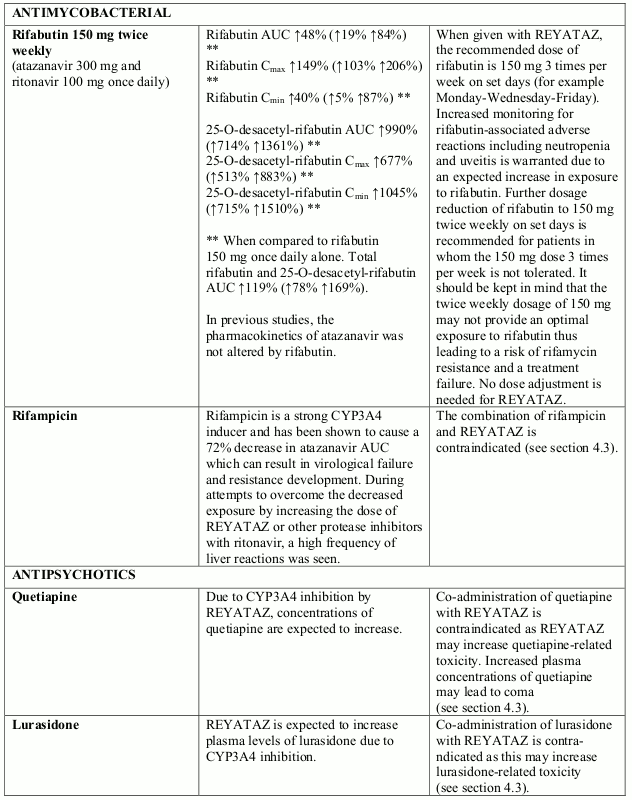
Combination of rifampicin (see section 4.5).
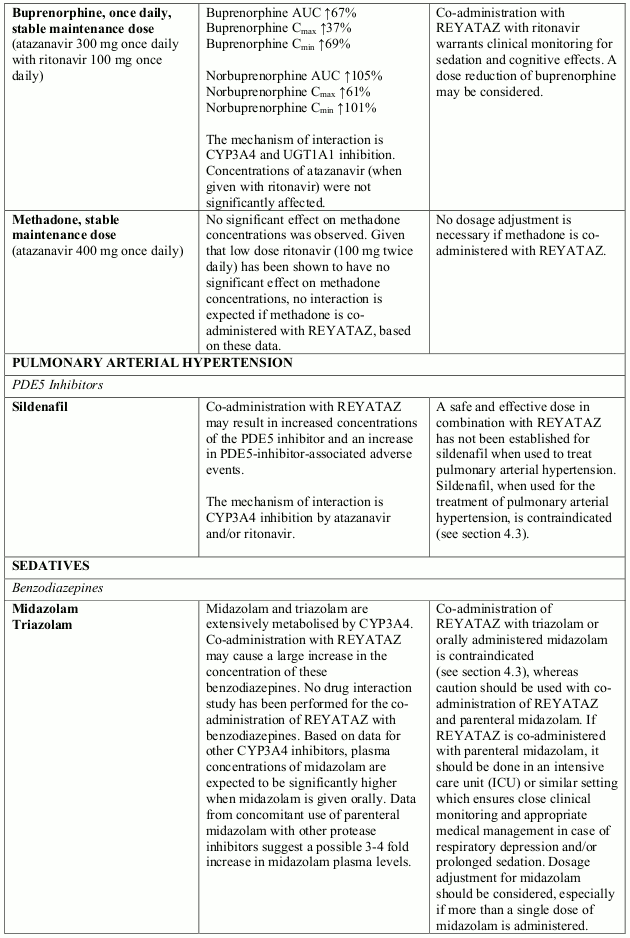
Combination of the PDE5 inhibitor sildenafil when used for the treatment of pulmonary arterial hypertension (PAH) only (see section 4.5). For co-administration of sildenafil for the treatment of erectile dysfunction see sections 4.4 and 4.5.
Co-administration with medicinal products that are substrates of the CYP3A4 isoform of cytochrome P450 and have narrow therapeutic windows (e.g. quetiapine, lurasidone, alfuzosin, astemizole, terfenadine, cisapride, pimozide, quinidine, bepridil, triazolam, midazolam administered orally (for caution on parenterally administered midazolam, see section 4.5), and ergot alkaloids, particularly, ergotamine, dihydroergotamine, ergonovine, methylergonovine) (see section 4.5).
Co-administration with grazoprevir-containing products, including elbasvir/grazoprevir fixed dose combination (see section 4.5).
Co-administration with glecaprevir/pibrentasvir fixed dose combination (see section 4.5)
Co-administration with products containing St. John’s wort (Hypericum perforatum) (see section 4.5).
Special warnings and precautions for use
While effective viral suppression with antiretroviral therapy has been proven to substantially reduce the risk of sexual transmission, a residual risk cannot be excluded. Precautions to prevent transmission should be taken in accordance with national guidelines.
Co-administration of REYATAZ with ritonavir at doses greater than 100 mg once daily has not been clinically evaluated. The use of higher ritonavir doses may alter the safety profile of atazanavir (cardiac effects, hyperbilirubinaemia) and therefore is not recommended. Only when atazanavir with ritonavir is co-administered with efavirenz, a dose increase of ritonavir to 200 mg once daily could be considered. In this instance, close clinical monitoring is warranted (see Interaction with other Medicinal Products below).
Patients with coexisting conditions
Hepatic impairment
Atazanavir is primarily hepatically metabolised and increased plasma concentrations were observed in patients with hepatic impairment (see sections 4.2 and 4.3). The safety and efficacy of REYATAZ has not been established in patients with significant underlying liver disorders. Patients with chronic hepatitis B or C and treated with combination antiretroviral therapy are at an increased risk for severe and potentially fatal hepatic adverse reactions. In case of concomitant antiviral therapy for hepatitis B or C, please refer also to the relevant Summary of Product Characteristics for these medicinal products (see section 4.8).
Patients with pre-existing liver dysfunction, including chronic active hepatitis, have an increased frequency of liver function abnormalities during combination antiretroviral therapy and should be monitored according to standard practice. If there is evidence of worsening liver disease in such patients, interruption or discontinuation of treatment must be considered. Renal impairment: No dosage adjustment is needed in patients with renal impairment. However, REYATAZ is not recommended in patients undergoing haemodialysis (see sections 4.2 and 5.2).
QT prolongation
Dose related asymptomatic prolongations in PR interval with REYATAZ have been observed in clinical studies. Caution should be used with medicinal products known to induce PR prolongations. In patients with pre-existing conduction problems (second degree or higher atrioventricular or complex bundle-branch block), REYATAZ should be used with caution and only if the benefits exceed the risk (see section 5.1). Particular caution should be used when prescribing REYATAZ in association with medicinal products which have the potential to increase the QT interval and/or in patients with pre-existing risk factors (bradycardia, long congenital QT, electrolyte imbalances (see sections 4.8 and 5.3).
Haemophiliac patients
There have been reports of increased bleeding, including spontaneous skin haematomas and haemarthroses, in type A and B haemophiliac patients treated with protease inhibitors. In some patients additional factor VIII was given. In more than half of the reported cases, treatment with protease inhibitors was continued or reintroduced if treatment had been discontinued. A causal relationship has been suggested, although the mechanism of action has not been elucidated. Haemophiliac patients should therefore be made aware of the possibility of increased bleeding.
Weight and metabolic parameters
An increase in weight and in levels of blood lipids and glucose may occur during antiretroviral therapy. Such changes may in part be linked to the disease control and life style. For lipids, there is in some cases evidence for a treatment effect, while for weight gain there is no strong evidence relating this to any particular treatment. For monitoring of blood lipids and glucose reference is made to established HIV treatment guidelines. Lipid disorders should be managed as clinically appropriate.
In clinical studies, REYATAZ (with or without ritonavir) has been shown to induce dyslipidaemia to a lesser extent than comparators.
Hyperbilirubinaemia
Reversible elevations in indirect (unconjugated) bilirubin related to inhibition of UDP-glucuronosyl transferase (UGT) have occurred in patients receiving REYATAZ (see section 4.8). Hepatic transaminase elevations that occur with elevated bilirubin in patients receiving REYATAZ should be evaluated for alternative aetiologies. Alternative antiretroviral therapy to REYATAZ may be considered if jaundice or scleral icterus is unacceptable to a patient. Dose reduction of atazanavir is not recommended because it may result in a loss of therapeutic effect and development of resistance.
Indinavir is also associated with indirect (unconjugated) hyperbilirubinaemia due to inhibition of UGT. Combinations of REYATAZ and indinavir have not been studied and co-administration of these medicinal products is not recommended (see section 4.5).
Withdrawal of ritonavir only under restrictive conditions
The recommended standard treatment is REYATAZ boosted with ritonavir, ensuring optimal pharmacokinetic parameters and level of virologic suppression.
The withdrawal of ritonavir from the boosted regimen of REYATAZ is not recommended, but may be considered in adults patients at the dose of 400 mg once daily with food only under the following combined restrictive conditions:
- absence of prior virologic failure
- undetectable viral load during the last 6 months under current regimen
- viral strains not harbouring HIV resistance associated mutations (RAMs) to current regimen.
REYATAZ given without ritonavir should not be considered in patients treated with a backbone regimen containing tenofovir disoproxil and with other concomitant medications that reduce atazanavir bioavailability (see section 4.5 In case of withdrawal of ritonavir from the recommended atazanavir boosted regimen) or in case of perceived challenging compliance.
REYATAZ given without ritonavir should not be used in pregnant patients given that it could result of suboptimal exposure of particular concern for the mother infection and vertical transmission.
Cholelithiasis
Cholelithiasis has been reported in patients receiving REYATAZ (see section 4.8). Some patients required hospitalization for additional management and some had complications. If signs or symptoms of cholelithiasis occur, temporary interruption or discontinuation of treatment may be considered.
Chronic kidney disease
Chronic kidney disease in HIV-infected patients treated with atazanavir, with or without ritonavir, has been reported during postmarketing surveillance. A large prospective observational study has shown an association between an increased incidence of chronic kidney disease and cumulative exposure to atazanavir/ritonavir-containing regimen in HIV-infected patients with an initially normal eGFR. This association was observed independently of exposure to tenofovir disoproxil. Regular monitoring of the renal function of patients should be maintained throughout the treatment duration (see section 4.8).
Nephrolithiasis
Nephrolithiasis has been reported in patients receiving REYATAZ (see section 4.8). Some patients required hospitalization for additional management and some had complications. In some cases, nephrolithiasis has been associated with acute renal failure or renal insufficiency. If signs or symptoms of nephrolithiasis occur, temporary interruption or discontinuation of treatment may be considered.
Immune reactivation syndrome
In HIV-infected patients with severe immune deficiency at the time of institution of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic pathogens may arise and cause serious clinical conditions, or aggravation of symptoms. Typically, such reactions have been observed within the first few weeks or months of initiation of CART. Relevant examples are cytomegalovirus retinitis, generalised and/or focal mycobacterial infections, and Pneumocystis jirovecii pneumonia. Any inflammatory symptoms should be evaluated and treatment instituted when necessary. Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported to occur in the setting of immune reactivation; however, the reported time to onset is more variable and these events can occurs many months after initiation of treatment.
Osteonecrosis
Although the aetiology is considered to be multifactorial (including corticosteroid use, alcohol consumption, severe immunosuppression, higher body mass index), cases of osteonecrosis have been reported particularly in patients with advanced HIV-disease and/or long-term exposure to combination antiretroviral therapy (CART). Patients should be advised to seek medical advice if they experience joint aches and pain, joint stiffness or difficulty in movement.
Rash and associated syndromes
Rashes are usually mild -to-moderate maculopapular skin eruptions that occur within the first 3 weeks of starting therapy with REYATAZ.
Stevens-Johnson syndrome (SJS), erythema multiforme, toxic skin eruptions and drug rash with eosinophilia and systemic symptoms (DRESS) syndrome have been reported in patients receiving REYATAZ. Patients should be advised of the signs and symptoms and monitored closely for skin reactions. REYATAZ should be discontinued if severe rash develops.
The best results in managing these events come from early diagnosis and immediate interruption of any suspect medicines. If the patient has developed SJS or DRESS associated with the use of REYATAZ, REYATAZ may not be restarted.
Interactions with other medicinal products
The combination of REYATAZ with atorvastatin is not recommended (see section 4.5).
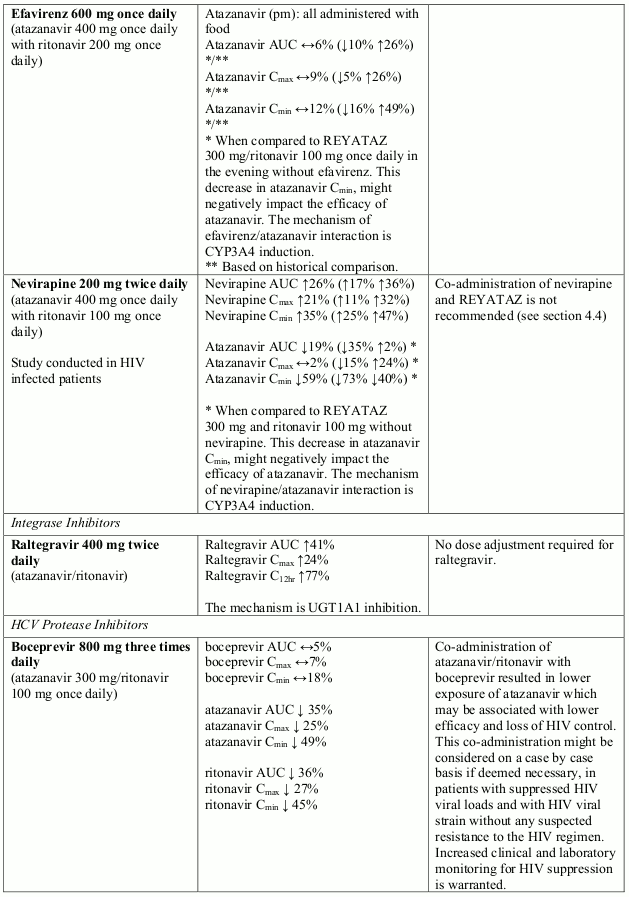
Co-administration of REYATAZ with nevirapine or efavirenz is not recommended (see section 4.5). If the co-administration of REYATAZ with an NNRTI is required, an increase in the dose of both REYATAZ and ritonavir to 400 mg and 200 mg, respectively, in combination with efavirenz could be considered with close clinical monitoring.
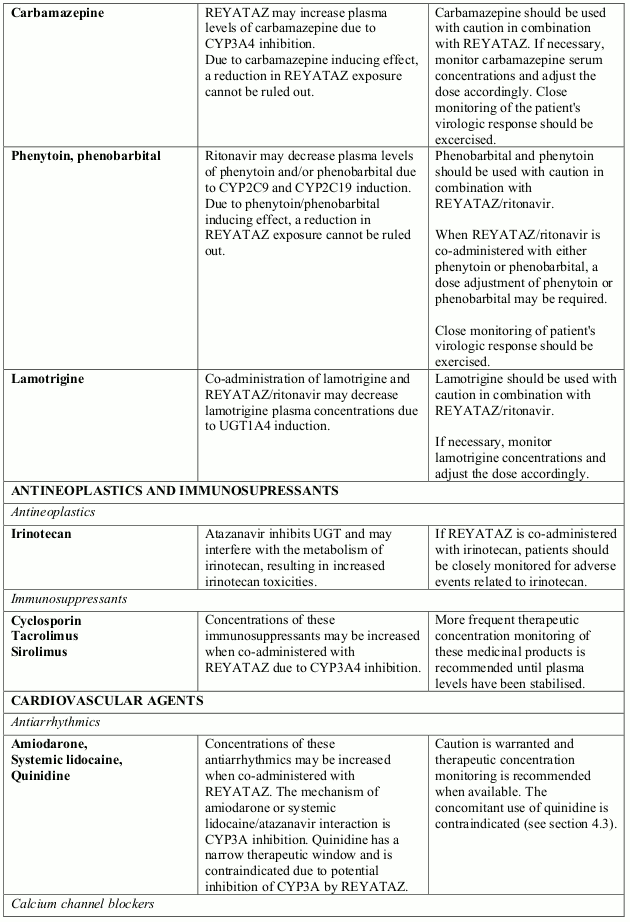
Atazanavir is metabolised principally by CYP3A4. Co-administration of REYATAZ and medicinal products that induce CYP3A4 is not recommended (see sections 4.3 and 4.5).
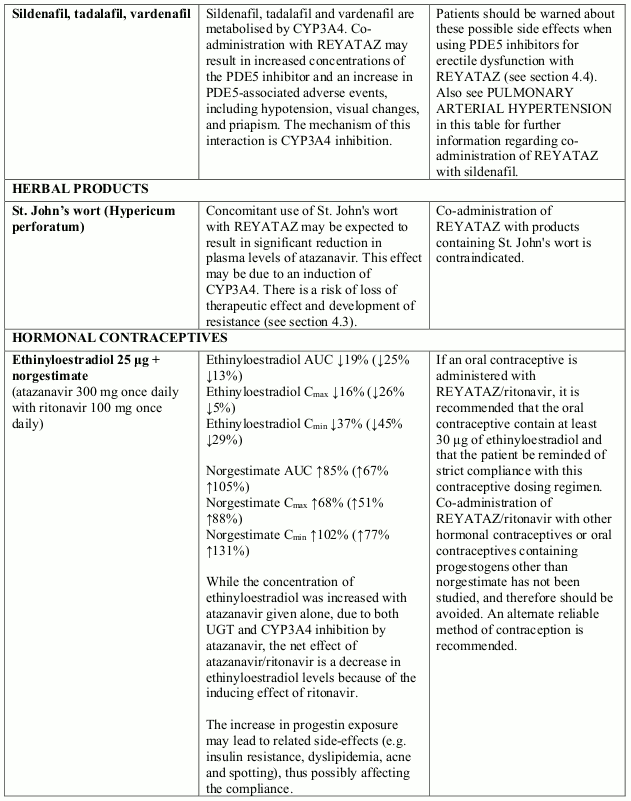
PDE5 inhibitors used for the treatment of erectile dysfunction: particular caution should be used when prescribing PDE5-inhibitors (sildenafil, tadalafil, or vardenafil) for the treatment of erectile dysfunction in patients receiving REYATAZ. Co-administration of REYATAZ with these medicinal products is expected to substantially increase their concentrations and may result in PDE5-associated adverse reactions such as hypotension, visual changes and priapism (see section 4.5).
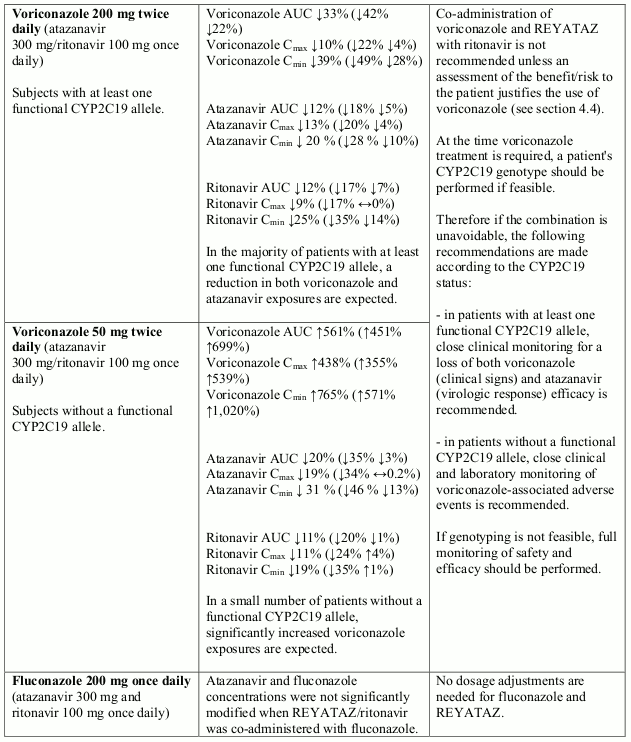
Co-administration of voriconazole and REYATAZ with ritonavir is not recommended, unless an assessment of the benefit/risk justifies the use of voriconazole.
In the majority of patients, a reduction in both voriconazole and atazanavir exposures are expected. In a small number of patients without a functional CYP2C19 allele, significantly increased voriconazole exposures are expected (see section 4.5).
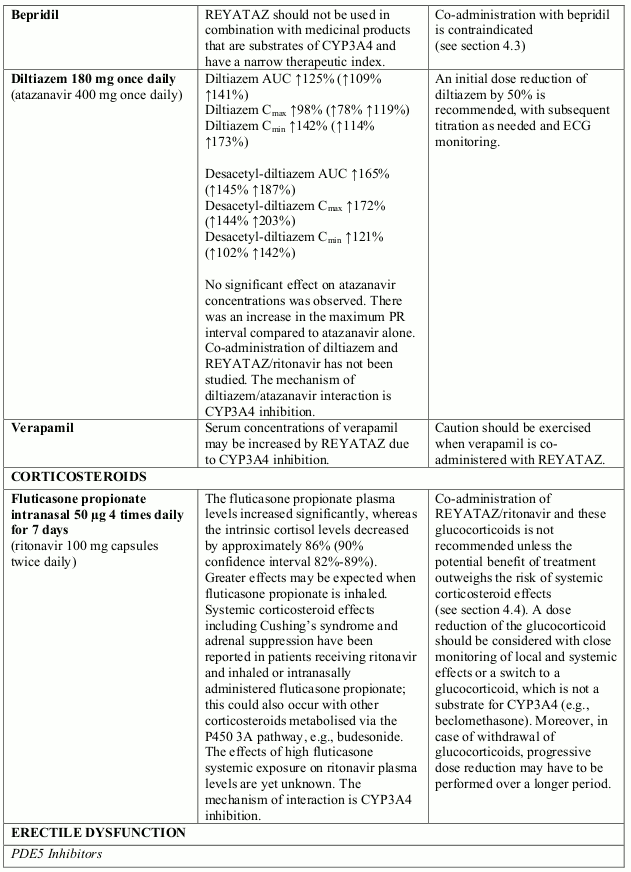
Concomitant use of REYATAZ/ritonavir and fluticasone or other glucocorticoids that are metabolised by CYP3A4 is not recommended unless the potential benefit of treatment outweighs the risk of systemic corticosteroid effects, including Cushing’s syndrome and adrenal suppression (see section 4.5).
Concomitant use of salmeterol and REYATAZ may result in increased cardiovascular adverse events associated with salmeterol. Co-administration of salmeterol and REYATAZ is not recommended (see section 4.5).
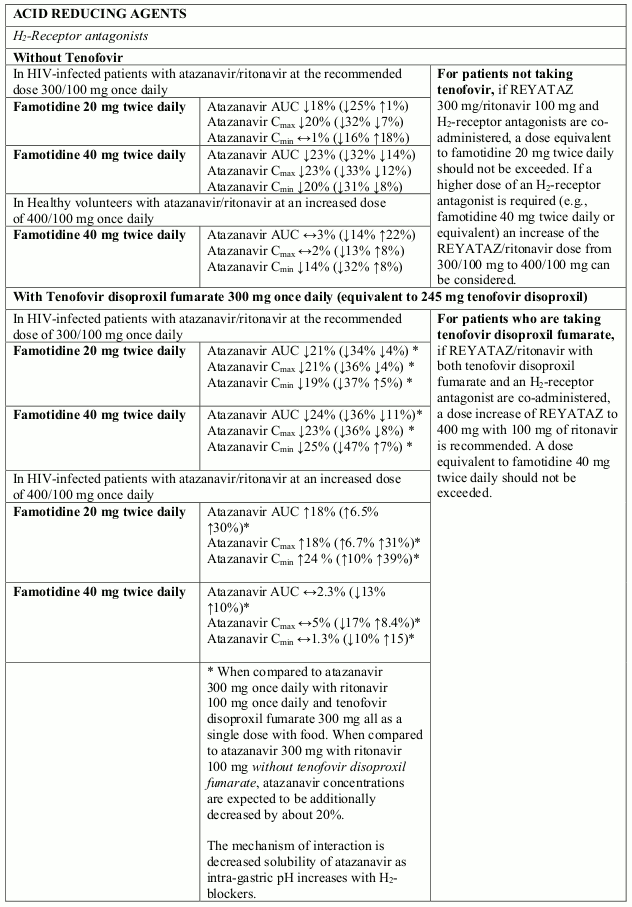
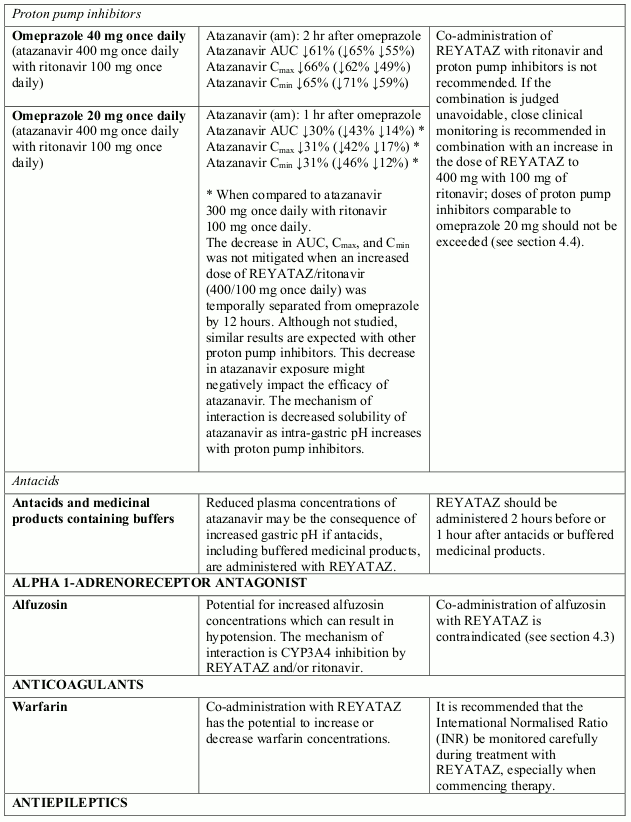
The absorption of atazanavir may be reduced in situations where gastric pH is increased irrespective of cause.
Co-administration of REYATAZ with proton pump inhibitors is not recommended (see section 4.5). If the combination of REYATAZ with a proton pump inhibitor is judged unavoidable, close clinical monitoring is recommended in combination with an increase in the dose of REYATAZ to 400 mg with 100 mg of ritonavir; doses of proton pump inhibitors comparable to omeprazole 20 mg should not be exceeded.
Co-administration of REYATAZ with other hormonal contraceptives or oral contraceptives containing progestogens other than norgestimate or norethindrone has not been studied, and therefore should be avoided (see section 4.5).
Paediatric population
Safety
Asymptomatic PR interval prolongation was more frequent in paediatric patients than adults. Asymptomatic first- and second-degree AV block was reported in paediatric patients (see section 4.8). Caution should be used with medicinal products known to induce PR prolongations. In paediatric patients with pre-existing conduction problems (second degree or higher atrioventricular or complex bundle-branch block), REYATAZ should be used with caution and only if the benefits exceed the risk. Cardiac monitoring is recommended based on the presence of clinical findings (e.g. bradycardia).
Efficacy
Atazanavir/ritonavir is not effective in viral strains harbouring multiple mutations of resistance.
Excipients
Lactose
Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucosegalactose malabsorption should not take this medicinal product.
Interaction with other medicinal products and other forms of interaction
When REYATAZ and ritonavir are co-administered, the metabolic drug interaction profile for ritonavir may predominate because ritonavir is a more potent CYP3A4 inhibitor than atazanavir. The Summary of Product Characteristics for ritonavir must be consulted before initiation of therapy with REYATAZ and ritonavir.
Atazanavir is metabolised in the liver through CYP3A4. It inhibits CYP3A4. Therefore, REYATAZ is contraindicated with medicinal products that are substrates of CYP3A4 and have a narrow therapeutic index: quetiapine, lurasidone, alfuzosin, astemizole, terfenadine, cisapride, pimozide, quinidine, bepridil, triazolam, orally administered midazolam, and ergot alkaloids, particularly ergotamine and dihydroergotamine (see section 4.3).
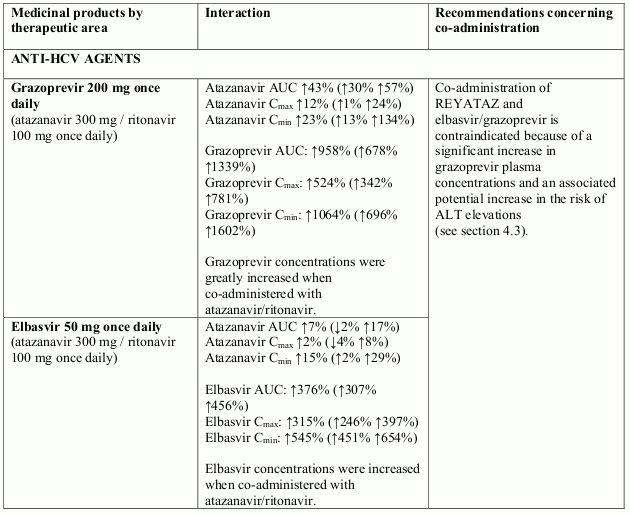
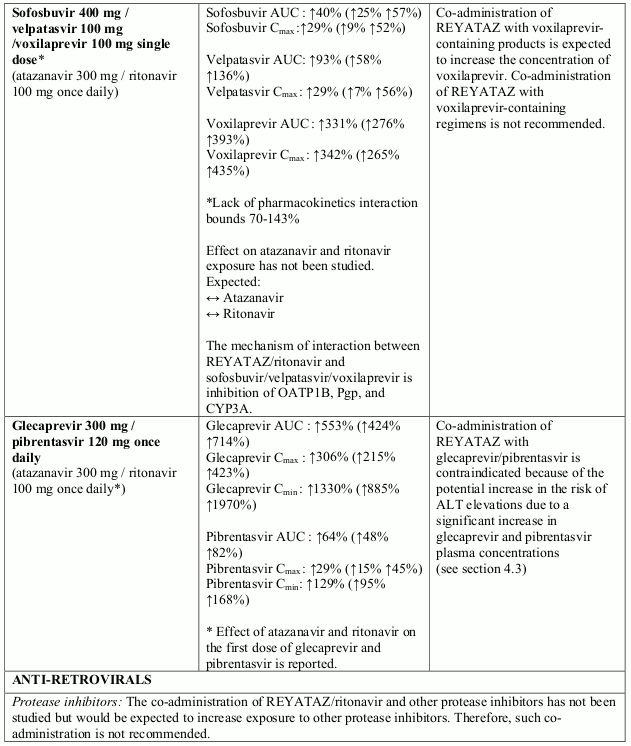
Co-administration of REYATAZ with grazoprevir-containing products, including elbasvir/grazoprevir fixed dose combination is contraindicated because of the increase in grazoprevir and elbasvir plasma concentrations and potential for the increase in risk of ALT elevations associated with increased grazoprevir concentrations (see section 4.3). Co-administration of REYATAZ with glecaprevir/pibrentasvir fixed dose combination is contraindicated because of the potential increase in the risk of ALT elevations due to a significant increase in glecapreir and pibrentasvir plasma concentrations (see section 4.3).
Other interactions
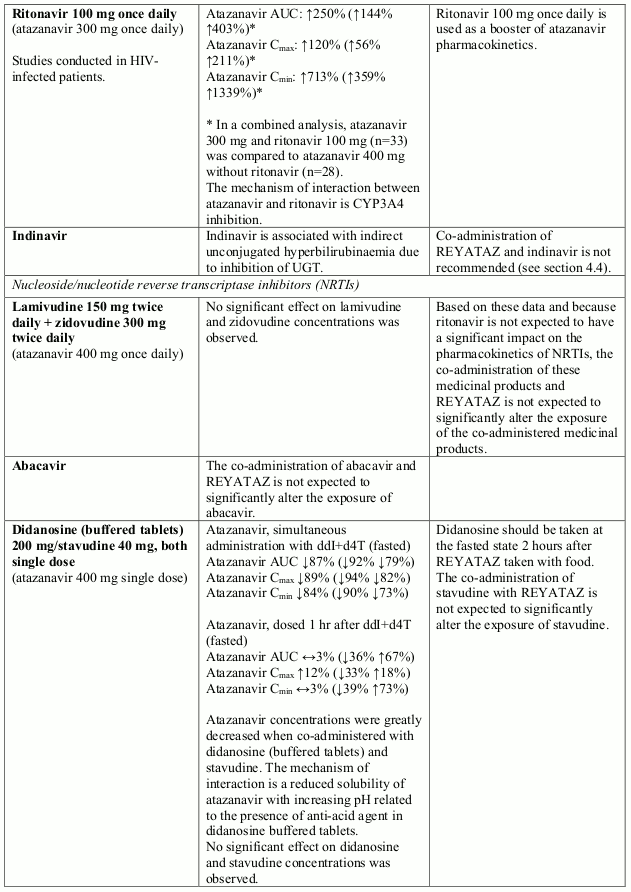
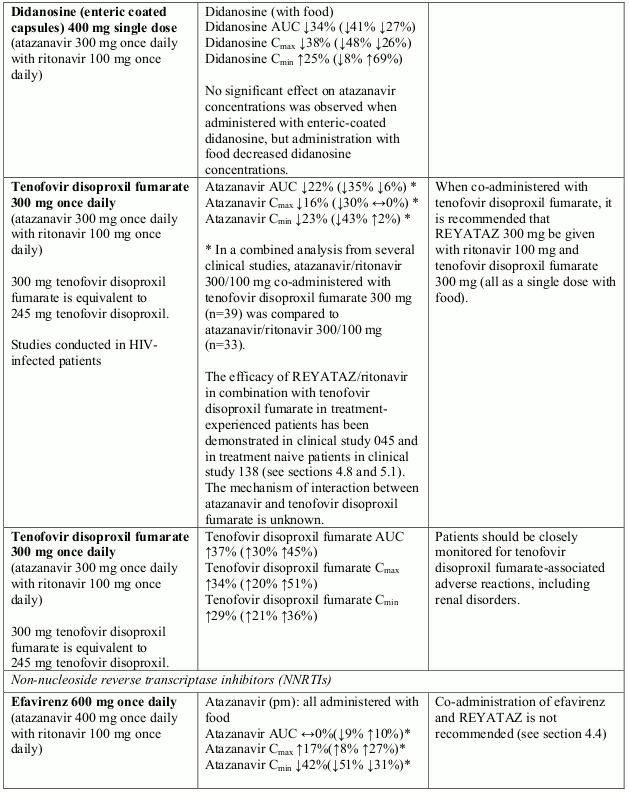
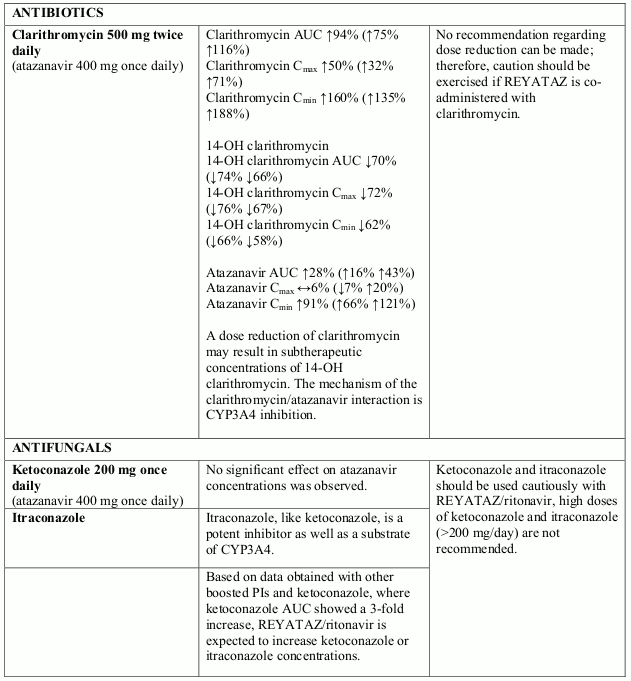
Interactions between atazanavir and other medicinal products are listed in the table below (increase is indicated as “↑”, decrease as “↓”, no change as “↔”). If available, 90% confidence intervals (CI) are shown in parentheses. The studies presented in Table 2 were conducted in healthy subjects unless otherwise noted. Of importance, many studies were conducted with unboosted atazanavir, which is not the recommended regimen of atazanavir (see section 4.4).
If withdrawal of ritonavir is medically warranted under restrictive conditions (see section 4.4), special attention should be given to atazanavir interactions that may differ in the absence of ritonavir (see information below Table 2).
Table 2. Interactions between REYATAZ and other medicinal products:
In case of withdrawal of ritonavir from the recommended atazanavir boosted regimen (see section 4.4)
The same recommendations for drug drug interactions would apply except:
- that co-administration is not recommended with tenofovir, boceprevir, carbamazepine, phenytoin, phenobarbital, proton pump inhibitors, and buprenorphine.
- that co-administration with famotidine is not recommended but if required, atazanavir without ritonavir should be administered either 2 hours after famotidine or 12 hours before. No single dose of famotidine should exceed 20 mg, and the total daily dose of famotidine should not exceed 40 mg.
- the need to consider that
- co-administration of voriconazole and REYATAZ without ritonavir may affect atazanavir concentrations
- co-administration of fluticasone and REYATAZ without ritonavir may increase fluticasone concentrations relative to fluticasone given alone
- if an oral contraceptive is administered with REYATAZ without ritonavir, it is recommended that the oral contraceptive contain no more than 30 µg of ethinyloestradiol
- no dose adjustment of lamotrigine is required
Paediatric population
Interaction studies have only been performed in adults.
Fertility, pregnancy and lactation
Pregnancy
A moderate amount of data in pregnant women (between 300-1000 pregnancy outcomes) indicate no malformative toxicity of atazanavir. Animal studies do not indicate reproductive toxicity (see section 5.3). The use of REYATAZ with ritonavir may be considered during pregnancy only if the potential benefit justifies the potential risk.
In clinical trial AI424-182 REYATAZ/ritonavir (300/100 mg or 400/100 mg) in combination with zidovudine/lamivudine was administered to 41 pregnant women during the second or third trimester. Six of 20 (30%) women on REYATAZ/ritonavir 300/100 mg and 13 of 21 (62%) women on REYATAZ/ritonavir 400/100 mg experienced grades 3 to 4 hyperbilirubinaemia. There were no cases of lactic acidosis observed in the clinical trial AI424-182.
The study assessed 40 infants who received antiretroviral prophylactic treatment (which did not include REYATAZ) and were negative for HIV-1 DNA at the time of delivery and/or during the first 6 months postpartum. Three of 20 infants (15%) born to women treated with REYATAZ/ritonavir 300/100 mg and four of 20 infants (20%) born to women treated with REYATAZ/ritonavir 400/100 mg experienced grade 3-4 bilirubin. There was no evidence of pathologic jaundice and six of 40 infants in this study received phototherapy for a maximum of 4 days. There were no reported cases of kernicterus in neonates.
For dosing recommendations see section 4.2 and for pharmacokinetic data see section 5.2.
It is not known whether REYATAZ with ritonavir administered to the mother during pregnancy will exacerbate physiological hyperbilirubinaemia and lead to kernicterus in neonates and infants. In the prepartum period, additional monitoring should be considered.
Breast-feeding
Atazanavir has been detected in human milk. As a general rule, it is recommended that HIV infected women not breast-feed their infants in order to avoid transmission of HIV.
Fertility
In a nonclinical fertility and early embryonic development study in rats, atazanavir altered oestrus cycling with no effects on mating or fertility (see section 5.3).
Effects on ability to drive and use machines
Patients should be informed that dizziness has been reported during treatment with regimens containing REYATAZ (see section 4.8).
Undesirable effects
Summary of the safety profile
REYATAZ has been evaluated for safety in combination therapy with other antiretroviral medicinal products in controlled clinical trials in 1,806 adult patients receiving REYATAZ 400 mg once daily (1,151 patients, 52 weeks median duration and 152 weeks maximum duration) or REYATAZ 300 mg with ritonavir 100 mg once daily (655 patients, 96 weeks median duration and 108 weeks maximum duration).
Adverse reactions were consistent between patients who received REYATAZ 400 mg once daily and patients who received REYATAZ 300 mg with ritonavir 100 mg once daily, except that jaundice and elevated total bilirubin levels were reported more frequently with REYATAZ plus ritonavir.
Among patients who received REYATAZ 400 mg once daily or REYATAZ 300 mg with ritonavir 100 mg once daily, the only adverse reactions of any severity reported very commonly with at least a possible relationship to regimens containing REYATAZ and one or more NRTIs were nausea (20%), diarrhoea (10%), and jaundice (13%). Among patients receiving REYATAZ 300 mg with ritonavir 100 mg, the frequency of jaundice was 19%. In the majority of cases, jaundice was reported within a few days to a few months after the initiation of treatment (see section 4.4).
Chronic kidney disease in HIV-infected patients treated with atazanavir, with or without ritonavir, has been reported during postmarketing surveillance. A large prospective observational study has shown an association between an increased incidence of chronic kidney disease and cumulative exposure to atazanavir/ritonavir-containing regimen in HIV-infected patients with an initially normal eGFR. This association was observed independently of exposure to tenofovir disoproxil. Regular monitoring of the renal function of patients should be maintained throughout the treatment duration (see section 4.4).
Tabulated list of adverse reactions
Assessment of adverse reactions for REYATAZ is based on safety data from clinical studies and post-marketing experience. Frequency is defined using the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
Immune system disorders
uncommon: hypersensitivity
Metabolism and nutrition disorders
uncommon: weight decreased, weight gain, anorexia, appetite increased
Psychiatric disorders
uncommon: depression, disorientation, anxiety, insomnia, sleep disorder, abnormal dream
Nervous system disorders
common: headache;
uncommon: peripheral neuropathy, syncope, amnesia, dizziness, somnolence, dysgeusia
Eye disorders
common: ocular icterus
Cardiac disorders
uncommon: torsades de pointesa
rare: QTc prolongationa, oedema, palpitation
Vascular disorders
uncommon: hypertension
Respiratory, thoracic and mediastinal disorders
uncommon: dyspnoea
Gastrointestinal disorders
common: vomiting, diarrhoea, abdominal pain, nausea, dyspepsia;
uncommon: pancreatitis, gastritis, abdominal distension, stomatitis aphthous, flatulence, dry mouth
Hepatobiliary disorders
common: jaundice;
uncommon: hepatitis, cholelithiasisa, cholestasisa;
rare: hepatosplenomegaly, cholecystitisa
Skin and subcutaneous tissue disorders
common: rash;
uncommon: erythemia multiformea,b, toxic skin eruptionsa,b, drug rash with eosinophilia and systemic symptoms (DRESS) syndromea,b, angioedemaa, urticaria, alopecia, pruritus;
rare: Stevens-Johnson syndromea,b, vesiculobullous rash, eczema, vasodilatation
Musculoskeletal and connective tissue disorders
uncommon: muscle atrophy, arthralgia, myalgia;
rare: myopathy
Renal and urinary disorders
uncommon: nephrolithiasisa, haematuria, proteinuria, pollakiuria, interstitial nephritis, chronic kidney diseasea;
rare: kidney pain
Reproductive system and breast disorders
uncommon: gynaecomastia
General disorders and administration site conditions
common: fatigue;
uncommon: chest pain, malaise, pyrexia, asthenia;
rare: gait disturbance
a These adverse reactions were identified through post-marketing surveillance, however, the frequencies were estimated from a statistical calculation based on the total number of patients exposed to REYATAZ in randomised controlled and other available clinical trials (n=2321).
b See description of selected adverse reactions for more details.
Description of selected adverse reactions
In HIV-infected patients with severe immune deficiency at the time of initiation of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic infections may arise. Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported; however, the reported time to onset is more variable and these events can occur many months after initiation of treatment (see section 4.4).
Cases of osteonecrosis have been reported, particularly in patients with generally acknowledged risk factors, advanced HIV disease or long-term exposure to combination antiretroviral therapy (CART). The frequency of this is unknown (see section 4.4).
Metabolic parameters
Weight and levels of blood lipids and glucose may increase during antiretroviral therapy (see section 4.4).
Rash and associated syndromes
Rashes are usually mild-to-moderate maculopapular skin eruptions that occur within the first 3 weeks of starting therapy with REYATAZ.
Stevens-Johnson syndrome (SJS), erythema multiforme, toxic skin eruptions and drug rash with eosinophilia and systemic symptoms (DRESS) syndrome have been reported with the use of REYATAZ (see section 4.4).
Laboratory abnormalities
The most frequently reported laboratory abnormality in patients receiving regimens containing REYATAZ and one or more NRTIs was elevated total bilirubin reported predominantly as elevated indirect [unconjugated] bilirubin (87% Grade 1, 2, 3, or 4). Grade 3 or 4 elevation of total bilirubin was noted in 37% (6% Grade 4). Among experienced patients treated with REYATAZ 300 mg once daily with 100 mg ritonavir once daily for a median duration of 95 weeks, 53% had Grade 3-4 total bilirubin elevations. Among naive patients treated with REYATAZ 300 mg once daily with 100 mg ritonavir once daily for a median duration of 96 weeks, 48% had Grade 3-4 total bilirubin elevations (see section 4.4).
Other marked clinical laboratory abnormalities (Grade 3 or 4) reported in ≥ 2% of patients receiving regimens containing REYATAZ and one or more NRTIs included: elevated creatine kinase (7%), elevated alanine aminotransferase/serum glutamic-pyruvic transaminase (ALT/SGPT) (5%), low neutrophils (5%), elevated aspartate aminotransferase/serum glutamic-oxaloacetic transaminase (AST/SGOT) (3%), and elevated lipase (3%).
Two percent of patients treated with REYATAZ experienced concurrent Grade 3-4 ALT/AST and Grade 3-4 total bilirubin elevations.
Paediatric population
In a clinical study AI424-020, paediatric patients 3 months to less than 18 years of age who received either the oral powder or capsule formulation had a mean duration of treatment with REYATAZ of 115 weeks. The safety profile in this study was overall comparable to that seen in adults. Both asymptomatic first-degree (23%) and second-degree (1%) atrioventricular block were reported in paediatric patients. The most frequently reported laboratory abnormality in paediatric patients receiving REYATAZ was elevation of total bilirubin (≥2.6 times ULN, Grade 3-4) which occurred in 45% of patients.
In clinical studies AI424-397 and AI424-451, paediatric patients 3 months to less than 11 years of age had a mean duration of treatment with REYATAZ oral powder of 80 weeks. No deaths were reported.
The safety profile in these studies was overall comparable to that seen in previous paediatric and adult studies. The most frequently reported laboratory abnormalities in paediatric patients receiving REYATAZ oral powder was elevation of total bilirubin (≥2.6 times ULN, Grade 3-4; 16%) and increased amylase (Grade 3-4; 33%), generally of non-pancreatic origin. Elevation in ALT levels were more frequently reported in paediatric patients in these studies than in adults.
Other special populations
Patients co-infected with hepatitis B and/or hepatitis C virus
Among 1,151 patients receiving atazanavir 400 mg once daily, 177 patients were co-infected with chronic hepatitis B or C, and among 655 patients receiving atazanavir 300 mg once daily with ritonavir 100 mg once daily, 97 patients were co-infected with chronic hepatitis B or C. Co-infected patients were more likely to have baseline hepatic transaminase elevations than those without chronic viral hepatitis. No differences in frequency of bilirubin elevations were observed between these patients and those without viral hepatitis. The frequency of treatment emergent hepatitis or transaminase elevations in co-infected patients was comparable between REYATAZ and comparator regimens (see section 4.4).
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.