Source: European Medicines Agency (EU) Revision Year: 2023 Publisher: Sanofi Winthrop Industrie, 82 avenue Raspail, 94250 Gentilly, France
Pharmacotherapeutic group: Antineoplastic agents, monoclonal antibodies
ATC code: L01FC02
Isatuximab is an IgG1-derived monoclonal antibody that binds to a specific extracellular epitope of CD38 receptor. CD38 is a transmembrane glycoprotein that is highly expressed on multiple myeloma cells.
In vitro, isatuximab acts through IgG Fc-dependent mechanisms including: antibody dependent cell mediated cytotoxicity (ADCC), antibody dependent cellular phagocytosis (ADCP), and complement dependent cytotoxicity (CDC). Furthermore, isatuximab can also trigger tumour cell death by induction of apoptosis via an Fc-independent mechanism.
In vitro, isatuximab blocks the enzymatic activity of CD38 which catalyses the synthesis and hydrolysis of cyclic ADP-ribose (cADPR), a calcium mobilizing agent. Isatuximab inhibits the cADPR production from extracellular nicotinamide adenine dinucleotide (NAD) in multiple myeloma cells.
In vitro, isatuximab can activate NK cells in the absence of CD38 positive target tumour cells.
In vivo, a decrease in absolute counts of total CD16+ and CD56+ NK cells, CD19+ B-cells, CD4+ Tcells and TREG (CD3+, CD4+, CD25+, CD127-) was observed in peripheral blood of patients treated with isatuximab monotherapy.
In multiple myeloma patients, SARCLISA monotherapy induced clonal expansion of the T-cell receptor repertoire indicating an adaptive immune response.
The combination of isatuximab and pomalidomide in vitro enhances cell lysis of CD38 expressing multiple myeloma cells by effector cells (ADCC), and by direct tumour cell killing compared to that of isatuximab alone. In vivo animal experiments using a human multiple myeloma xenograft model in mice demonstrated that the combination of isatuximab and pomalidomide results in enhanced antitumour activity compared to the activity of isatuximab or pomalidomide alone.
The efficacy and safety of SARCLISA in combination with pomalidomide and dexamethasone were evaluated in ICARIA-MM (EFC14335), a multicentre, multinational, randomised, open-label, 2-arm, phase III study in patients with relapsed and/or refractory multiple myeloma. Patients had received at least two prior therapies including lenalidomide and a proteasome inhibitor with disease progression on or within 60 days after the end of the previous therapy. Patients with primary refractory disease were excluded.
A total of 307 patients were randomised in a 1:1 ratio to receive either SARCLISA in combination with pomalidomide and dexamethasone (Isa-Pd, 154 patients) or pomalidomide and dexamethasone (Pd, 153 patients). Treatment was administered in both groups in 28-day cycles until disease progression or unacceptable toxicity. SARCLISA 10 mg/kg was administered as an I.V. infusion weekly in the first cycle and every two weeks thereafter. Pomalidomide 4 mg was taken orally once daily from day 1 to day 21 of each 28-day cycle. Dexamethasone (oral/intravenous) 40 mg (20 mg for patients ≥75 years of age) was given on days 1, 8, 15 and 22 for each 28-day cycle.
Overall, demographic and disease characteristics at baseline were similar between the two treatment groups, with some minor imbalances. The median patient age was 67 years (range 36-86), 19.9% of patients were ≥75 years. ECOG PS was 0 in 35.7% of patients in the isatuximab arm and 45.1% in the comparator arm, 1 in 53.9% in the isatuximab arm and 44.4% in the comparator arm, and 2 in 10.4% in the isatuximab arm and 10.5% in the comparator arm, 10.4% of patients in the isatuximab arm versus 10.5% in the comparator arm entered the study with a history of COPD or asthma, and 38.6% versus 33.3% of patients with renal impairment (creatinine clearance <60 mL/min/1.73 m²) were included in the isatuximab arm versus the comparator arm , respectively. The International Staging System (ISS) stage at study entry was I in 37.5% (41.6% in the isatuximab arm and 33.3% in the comparator arm), II in 35.5% (34.4% in the isatuximab arm and 36.6% in the comparator arm) and III in 25.1% (22.1% in the isatuximab arm and 28.1% in the comparator arm) of patients. Overall, 19.5% of patients (15.6% in the isatuximab arm and 23.5% in the comparator arm) had high-risk chromosomal abnormalities at study entry; del(17p), t(4;14) and t(14;16) were present in 12.1% (9.1% in the isatuximab arm and 15.0% in the comparator arm), 8.5% (7.8% in the isatuximab arm and 9.2% in the comparator arm) and 1.6% (0.6% in the isatuximab arm and 2.6% in the comparator arm) of patients, respectively.
The median number of prior lines of therapy was 3 (range 2-11). All patients received a prior proteasome inhibitor, all patients received prior lenalidomide, and 56.4% of patients received prior stem cell transplantation. The majority of patients (92.5%) were refractory to lenalidomide, 75.9% to a proteasome inhibitor, and 72.6% to both an immunomodulatory and a proteasome inhibitor, and 59% of patients were refractory to lenalidomide at last line of therapy.
The median duration of treatment was 41.0 weeks for the Isa-Pd group compared to 24.0 weeks for the Pd group.
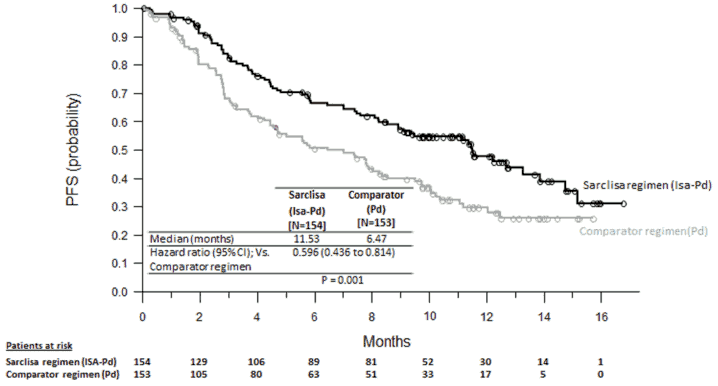
Progression-free survival (PFS) was the primary efficacy endpoint of ICARIA-MM. The improvement in PFS represented a 40.4% reduction in the risk of disease progression or death in patients treated with Isa-Pd.
Efficacy results are presented in Table 7 and Kaplan-Meier curves for PFS and OS are provided in Figures 1 and 2.
Table 7. Efficacy of SARCLISA in combination with pomalidomide and dexamethasone versus pomalidomide and dexamethasone in the treatment of multiple myeloma (intent-to-treat analysis):
| Endpoint | SARCLISA + pomalidomide + dexamethasone N=154 | Pomalidomide + dexamethasone N=153 |
|---|---|---|
| Progression-Free Survivalab | ||
| Median (months) [95% CI] | 11.53 [8.936-13.897] | 6.47 [4.468-8.279] |
| Hazard ratioc [95% CI] | 0.596 [0.436-0.814] | |
| p-value (stratified log-rank test)c | 0.0010 | |
| Overall Response Rated Responders (sCR+CR+VGPR+PR) n() [95 CI]e | 93 (60.4) [0.5220-0.6817] | 54 (35.3) [0.2775-0.4342] |
| Odds ratio vs comparator [95% exact CI] | 2.795 [1.715-4.562] | |
| p-value (stratified Cochran- Mantel-Haenszel)c | <0.0001 | |
| Stringent Complete Response (sCR) + Complete Response (CR) n (%) | 7 (4.5) | 3 (2.0) |
| Very Good Partial Response (VGPR) n (%) | 42 (27.3) | 10 (6.5) |
| Partial Response (PR) n (%) | 44 (28.6) | 41 (26.8) |
| VGPR or better n () [95 CI]e | 49 (31.8) [0.2455-0.3980] | 13 (8.5) [0.0460-0.1409] |
| Odds ratio vs comparator [95% exact CI] | 5.026 [2.514-10.586] | |
| p-value (stratified Cochran-Mantel- Haenszel)c | <0.0001 | |
| Duration of Responsef* Median in months [95% CI]g | 13.27 [10.612-NR] | 11.07 [8.542-NR] |
a PFS results were assessed by an Independent Response Committee based on central laboratory data for Mprotein and central radiologic imaging review using the International Myeloma Working Group (IMWG) criteria.
b Patients without progressive disease or death before the analysis cut-off or the date of initiation of further antimyeloma treatment were censored at the date of the last valid disease assessment not showing disease progression performed prior to initiation of a further anti-myeloma treatment (if any) or the analysis cut-off date, whichever came first.
c Stratified on age (<75 years versus >75 years) and number of previous lines of therapy (2 or 3 versus >3) according to IRT.
d sCR, CR, VGPR and PR were evaluated by the IRC using the IMWG response criteria.
e Estimated using Clopper-Pearson method.
f The duration of response was determined for patients who achieved a response of ≥PR (93 patients in the isatuximab arm and 54 patients in the comparator arm). Kaplan-Meier estimates of duration of response. g CI for Kaplan-Meier estimates are calculated with log-log transformation of survival function and methods of Brookmeyer and Crowley.
* Cut-off date of 11-Oct-2018. Median follow-up time=11.60 months. HR<1 favours Isa-Pd arm.
NR: not reached
In patients with high-risk cytogenetics (central laboratory assessment), median PFS was 7.49 (95% CI: 2.628 to NC) in the Isa-Pd group and 3.745 (95% CI: 2.793 to 7.885) in the Pd group (HR=0.655; 95% CI: 0.334 to 1.283). PFS improvements in the Isa-Pd group were also observed in patients >75 years (HR=0.479; 95% CI: 0.242 to 0.946), with ISS stage III at study entry (HR=0.635; 95% CI: 0.363 to 1.110), with baseline creatinine clearance <60 ml/min/1.73 m² (HR=0.502; 95% CI: 0.297 to 0.847), with >3 prior lines of therapy (HR=0.590; 95% CI: 0.356 to 0.977), in patients refractory to prior therapy with lenalidomide (HR=0.593; 95% CI: 0.431 to 0.816) or proteasome inhibitor (HR=0.578; 95% CI: 0.405 to 0.824) and in those refractory to lenalidomide at the last line before to the study entry (HR= 0.601; 95%CI: 0.436 to 0.828).
Insufficient data is available to conclude on the efficacy of Isa-Pd in patients previously treated with daratumumab (1 patient in the isatuximab arm and no patient in the comparator arm).
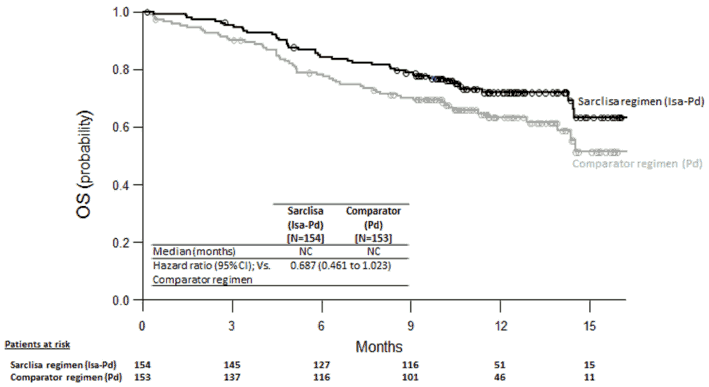
The median time to first response in responders was 35 days in the Isa-Pd group versus 58 days in the Pd group. With a median duration of follow-up of 11.56 months in the Isa-Pd group and 11.73 months in the Pd group, median overall survival was not reached for either treatment group. The hazard ratio for OS was 0.687 (95% CI: 0.461-1.023, p-value=0.0631).
Figure 1. Kaplan-Meier Curves of PFS – ITT population – ICARIA-MM (assessment by the IRC):
Figure 2. Kaplan-Meier Curves of OS – ITT population – ICARIA-MM:
Cut-off date = 11 October 2018
In the ICARIA-MM (EFC14335) study, a weight-based volume was used for isatuximab infusion. The fixed volume infusion method as described in section 4.2 was evaluated in study TCD14079 Part B and pharmacokinetics simulations confirmed minimal differences between the pharmacokinetics following injection applying a volume based on patient weight and a fixed volume of 250 mL (see section 5.2). In study TCD14079 part B, there were no new safety signals or differences in efficacy and safety as compared to ICARIA-MM.
The efficacy and safety of SARCLISA in combination with carfilzomib and dexamethasone were evaluated in IKEMA (EFC15246), a multicentre, multinational, randomized, open-label, 2-arm, phase III study in patients with relapsed and/or refractory multiple myeloma. Patients had received one to three prior therapies. Patients with primary refractory disease, who had previously been treated with carfilzomib, or who were refractory to previous anti-CD38 monoclonal antibody treatment were excluded.
A total of 302 patients were randomized in a 3:2 ratio to receive either SARCLISA in combination with carfilzomib and dexamethasone (Isa-Kd, 179 patients) or carfilzomib and dexamethasone (Kd, 123 patients). Treatment was administered in both groups in 28-day cycles until disease progression or unacceptable toxicity. SARCLISA 10 mg/kg was administered as an I.V. infusion weekly in the first cycle and every two weeks thereafter. Carfilzomib was administered as an I.V. infusion at the dose of 20 mg/m² on days 1 and 2; 56 mg/m² on days 8, 9, 15 and 16 of cycle 1; and at the dose of 56 mg/m² on days 1, 2, 8, 9, 15 and 16 for subsequent cycles of each 28-day cycle. Dexamethasone (IV on the days of isatuximab and/or carfilzomib infusions, and PO on the other days) 20 mg was given on days 1, 2, 8, 9, 15, 16, 22 and 23 for each 28-day cycle.
Overall, demographic and disease characteristics at baseline were similar between the two treatment groups. The median patient age was 64 years (range 33-90), 8.9% of patients were ≥75 years. ECOG PS was 0 in 53.1% of patients in the Isa-Kd group and 59.3% in the Kd group, 1 in 40.8% in the IsaKd group and 36.6% in the Kd group, and 2 in 5.6% in the Isa-Kd group and 4.1% in the Kd group, and 3 in 0.6% in the Isa-Kd group and 0% in the Kd group. The proportion of patients with renal impairment (eGFR<60 mL/min/1.73 m²) was 24.0% in the Isa-Kd group versus 14.6% in the Kd group. The International Staging System (ISS) stage at study entry was I in 53.0%, II in 31.1%, and III in 15.2% of patients. The Revised-ISS (R-ISS) stage at study entry was I in 25.8%, II in 59.6%, and III in 7.9% of patients. Overall, 24.2% of patients had high -risk chromosomal abnormalities at study entry; del(17p), t(4;14), t(14;16) were present in 11.3%, 13.9% and 2.0% of patients, respectively. In addition, gain(1q21) was present in 42.1% of patients.
The median number of prior lines of therapy was 2 (range 1-4) with 44.4% of patients who received 1 prior line of therapy. Overall, 89.7% of patients received prior proteasome inhibitors, 78.1% received prior immunomodulators (including 43.4% who received prior lenalidomide), and 61.3% received prior stem cell transplantation. Overall, 33.1% of patients were refractory to prior proteasome inhibitors, 45.0% were refractory to prior immunomodulators (including 32.8% refractory to lenalidomide), and 20.5% were refractory to both a proteasome inhibitor and an immunomodulator.
The median duration of treatment was 80.0 weeks for the Isa-Kd group compared to 61.4 weeks for the Kd group.
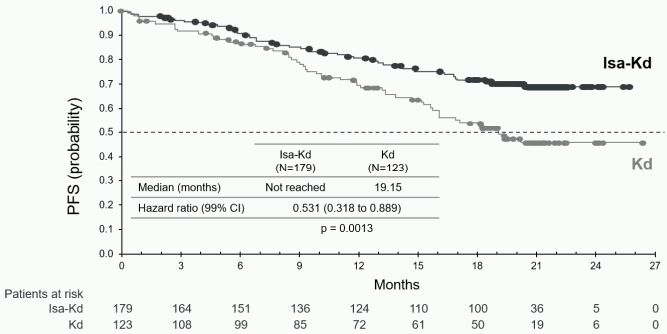
Progression-free survival (PFS) was the primary efficacy endpoint of IKEMA. With a median followup time of 20.73 months, the primary analysis of PFS showed a statistically significant improvement in PFS represented by a 46.9% reduction in the risk of disease progression or death in patients treated with Isa-Kd compared to patients treated with Kd.
Efficacy results are presented in Table 8 and Kaplan-Meier curves for PFS are provided in the Figure 3.
Table 8. Efficacy of SARCLISA in combination with carfilzomib and dexamethasone versus carfilzomib and dexamethasone in the treatment of multiple myeloma (intent-to-treat analysis):
| Endpoint | SARCLISA + carfilzomib + dexamethasone N=179 | Carfilzomib + dexamethasone N=123 |
|---|---|---|
| Progression-Free Survivala | ||
| Median (months) [95% CI] | NR [NR-NR] | 19.15 [15.77-NR] |
| Hazard ratiob [99% CI] | 0.531 [0.318-0.889] | |
| p-value (Stratified Log-Rank test)b | 0.0013 | |
| Overall Response Ratec | ||
| Responders (sCR+CR+VGPR+PR) [95% CI]d | 86.6% [0.8071-0.9122] | 82.9% [0.7509-0.8911] |
| p-value (stratified Cochran-Mantel- Haenszel)b | 0.3859 | |
| Complete Response (CR) | 39.7% | 27.6% |
| Very Good Partial Response (VGPR) | 33.0% | 28.5% |
| Partial Response (PR) | 14.0% | 26.8% |
| VGPR or better (sCR+CR+VGPR) [95% CI]d | 72.6% [0.6547-0.7901] | 56.1% [0.4687 -0.6503] |
| p-value (stratified Cochran- Mantel-Haenszel)be | 0.0021 | |
| CRf [95% CI]d | 39.7% [0.3244-0.4723] | 27.6% [0.1996 to 0.3643] |
| Minimal Residual Disease negative rateg [95% CI]d | 29.6% [0.2303-0.3688] | 13.0% [0.0762-0.2026] |
| p-value (stratified Cochran- Mantel-Haenszel)be | 0.0008 | |
| Duration of Responseh* (PR or better) | ||
| Median in months [95% CI]i | NR [NR-NR] | NR [14.752-NR] |
| Hazard ratiob [95% CI] | 0.425 [0.269-0.672] | |
a PFS results were assessed by an Independent Response Committee based on central laboratory data for Mprotein and central radiologic imaging review using the International Myeloma Working Group (IMWG) criteria.
b Stratified on number of previous lines of therapy (1 versus >1) and R-ISS (I or II versus III versus not classified) according to IRT.
c sCR, CR, VGPR, and PR were evaluated by the IRC using the IMWG response criteria.
d Estimated using Clopper-Pearson method.
e Nominal p-value.
f CR to be tested with final analysis.
g Based on a sensitivity level of 10-5 by NGS in ITT population.
h Based on Responders in the ITT population. Kaplan-Meier estimates of duration of response.
i CI for Kaplan-Meier estimates are calculated with log-log transformation of survival function and methods of Brookmeyer and Crowley.
* Cut-off date of 7 February 2020. Median follow-up time=20.73 months. HR<1 favours Isa-Kd arm.
NR: not reached.
PFS improvements in the Isa-Kd group were observed in patients with high -risk cytogenetics (central laboratory assessment, HR = 0.724; 95% CI: 0.361 to 1.451), with gain (1q21) chromosomal abnormality (HR=0.569; 95% CI: 0.330 to 0.981), ≥65 years (HR =0.429; 95% CI: 0.248 to 0.742), with baseline eGFR (MDRD) < 60 mL/min/1.73 m² (HR =0.273; 95% CI: 0.113 to 0.660), with >1 prior line of therapy (HR =0.479; 95% CI: 0.294 to 0.778), with ISS stage III at study entry (HR=0.650; 95% CI: 0.295 to 1.434), and in patients refractory to prior therapy with lenalidomide (HR=0.598; 95% CI: 0.339 to 1.055).
In the sensitivity analysis without censoring for further anti-myeloma therapy, the median PFS was not reached (NR) in the Isa-Kd group versus 19.0 months (95% CI: 15.38 to NR) in the Kd group (HR=0.572; 99% CI: 0.354 to 0.925, p=0.0025). Insufficient data is available to conclude on the efficacy of Isa-Kd in patients previously treated with daratumumab (1 patient in the isatuximab arm and no patient in the comparator arm).
The median time to first response was 1.08 months in the Isa-Kd group and 1.12 months in the Kd group. With a median follow-up time of 20.73 months, 17.3% patients in the Isa-Kd arm and 20.3% patients in the Kd arm had died.
Figure 3. Kaplan-Meier Curves of PFS – ITT population – IKEMA (assessment by the IRC):
Cut-off date = 07 February 2020.
Among patients with eGFR (MDRD) <50 mL/min/1.73 m² at baseline, complete renal response (≥60 mL/min/1.73 m² at ≥1 postbaseline assessment) was observed for 52.0% (13/25) of patients in the IsaKd group and 30.8% (4/13) in the Kd group. Sustained complete renal response (≥60 days) occurred in 32.0% (8/25) of patients in the Isa-Kd group and in 7.7% (1/13) in the Kd group. In the 4 patients in the Isa-Kd group and the 3 patients in the Kd group with severe renal impairment at baseline (eGFR (MDRD) >15 to <30 mL/min/1.73 m²), minimal renal response (≥30 to <60 mL/min/1.73 m² at ≥1 postbaseline assessment) was observed for 100% of patients in the Isa-Kd group and 33.3% of patients in the Kd group.
At a median follow-up time of 43.96 months, final PFS analysis showed a median PFS of 35.65 months for Isa-Kd group compared to 19.15 months for Kd group, with a hazard ratio of 0.576 (95.4% CI: 0.418 to 0.792). Final complete response, determined using a validated isatuximab-specific IFE assay (Sebia Hydrashift) (see section 4.5), was 44.1% in Isa-Kd group compared to 28.5% in Kd group, with odds ratio 2.094 (95% CI: 1.259 to 3.482, descriptive p=0.0021). In 26.3% of patients in Isa-Kd group, both MRD negativity and CR were met compared to 12.2% in Kd group, with odds ratio 2.571 (95% CI: 1.354 to 4.882, descriptive p=0.0015).
The European Medicines Agency has deferred the obligation to submit the results of studies with SARCLISA in one or more subsets of the paediatric population in the treatment of malignant neoplasms of the haematopoietic and lymphoid tissue. See section 4.2 for information on paediatric use.
The pharmacokinetics of isatuximab were assessed in 476 patients with multiple myeloma treated with isatuximab intravenous infusion as a single agent or in combination with pomalidomide and dexamethasone, at doses ranging from 1 to 20 mg/kg, administered either once weekly; every 2 weeks; or every 2 weeks for 8 weeks followed by every 4 weeks; or every week for 4 weeks followed by every 2 weeks.
Isatuximab displays nonlinear pharmacokinetics with target-mediated drug disposition due to its binding to CD38 receptor.
Isatuximab exposure (area under the plasma concentration-time curve over the dosing interval AUC) increases in a greater than dose proportional manner from 1 to 20 mg/kg following every 2 weeks schedule, while no deviation to the dose proportionality is observed between 5 and 20 mg/kg following every week for 4 weeks followed by every 2 weeks schedule. This is due to the high contribution of nonlinear target-mediated clearance to the total clearance at doses below 5 mg/kg, which becomes negligible at higher doses. After isatuximab 10 mg/kg administration every week for 4 weeks followed by every 2 weeks, the median time to reach steady state was 18 weeks with a 3.1-fold accumulation. In ICARIA-MM, clinical trial performed in relapsed and/or refractory multiple myeloma patients treated with isatuximab in combination with pomalidomide and dexamethasone, the mean (CV%) predicted maximum plasma concentration Cmax and AUC at steady state were 351 µg/mL (36.0%) and 72,600 µg.h/mL (51.7%), respectively. Although the change from a weight-based volume administration method for isatuximab infusion to the fixed volume infusion method resulted in changes in the tmax, the change had a limited impact on pharmacokinetics exposure with comparable simulated Cmax at steady state (283 µg/mL vs 284 µg/mL) and Ctrough at 4 weeks (119 µg/mL vs 119 µg/mL) for a patient with median weight (76 kg). Also for other patient weight groups, Cmax and Ctrough were comparable. In IKEMA, clinical trial performed in relapsed and/or refractory multiple myeloma patients treated with isatuximab in combination with carfilzomib and dexamethasone, the mean (CV%) predicted maximum plasma concentration Cmax and AUC at steady state were 637 µg/mL (30.9%) and 152,000 µg.h/mL (37.8%), respectively.
The pharmacokinetics of isatuximab and pomalidomide, or of isatuximab and carfilzomib, were not influenced by their co-administration.
The estimated total volume of distribution of isatuximab is 8.75 L.
As a large protein, isatuximab is expected to be metabolized by non-saturable proteolytic catabolism processes.
Isatuximab is eliminated by two parallel pathways, a nonlinear target-mediated pathway predominating at low concentrations, and a nonspecific linear pathway predominating at higher concentrations. In the therapeutic plasma concentrations range, the linear pathway is predominant and decreases over time by 50% to a steady state value of 9.55 mL/h (0.229 L/day). This is associated with a terminal half-life of 28 days.
The population pharmacokinetic analyses of 476 patients aged 36 to 85 years showed comparable exposure to isatuximab in patients <75 years old (n=406) versus ≥75 years old (n=70).
The population pharmacokinetic analysis with 207 female (43.5%) and 269 male (56.5%) patients showed no clinically meaningful effect of gender on isatuximab pharmacokinetics.
The population pharmacokinetic analysis with 377 Caucasian (79%), 25 Asian (5%), 18 Black (4%), and 33 other race (7%) patients showed no clinically meaningful effect of race on isatuximab pharmacokinetics.
Based on a population pharmacokinetics analysis using data from 476 patients, the clearance of isatuximab increased with increasing body weight, supporting the body-weight based dosing.
No formal studies of isatuximab in patients with hepatic impairment have been conducted. Out of the 476 patients of the population pharmacokinetic analyses, 65 patients presented with mild hepatic impairment [total bilirubin >1 to 1.5 times upper limit of normal (ULN) or aspartate amino transferase (AST) > ULN] and 1 patient had moderate hepatic impairment (total bilirubin >1.5 to 3 times ULN and any AST). Mild hepatic impairment had no clinically meaningful effect on the pharmacokinetics of isatuximab. The effect of moderate (total bilirubin >1.5 times to 3 times ULN and any AST) and severe hepatic impairment (total bilirubin >3 times ULN and any AST) on isatuximab pharmacokinetics is unknown. However, since isatuximab is a monoclonal antibody, it is not expected to be cleared via hepatic-enzyme mediated metabolism and as such, variation in hepatic function is not expected to affect the elimination of isatuximab (see section 4.2).
No formal studies of isatuximab in patients with renal impairment have been conducted. The population pharmacokinetic analyses on 476 patients included 192 patients with mild renal impairment (60 mL/min/1.73 m² ≤ estimated glomerular filtration rate (e-GFR) <90 mL/min/1.73 m²), 163 patients with moderate renal impairment (30 mL/min/1.73 m² ≤ e-GFR < 60 mL/min/1.73 m²) and 12 patients with severe renal impairment (e-GFR <30 mL/min/1.73 m²). Analyses suggested no clinically meaningful effect of mild to severe renal impairment on isatuximab pharmacokinetics compared to normal renal function.
Isatuximab was not evaluated in patients under 18 years of age.
Non-clinical data reveal no special hazard for humans based on conventional studies of repeated dose toxicity, albeit the species selected is not pharmacologically responsive and therefore the relevance for humans is not known. Genotoxicity, carcinogenic potential and toxicity to reproduction and development studies have not been performed.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.