Source: FDA, National Drug Code (US) Revision Year: 2020
Isatuximab-irfc is an IgG1-derived monoclonal antibody that binds to CD38 expressed on the surface of hematopoietic and tumor cells, including multiple myeloma cells. Isatuximab-irfc induces apoptosis of tumor cells and activation of immune effector mechanisms including antibody-dependent cell-mediated cytotoxicity (ADCC), antibody-dependent cellular phagocytosis (ADCP), and complement dependent cytotoxicity (CDC). Isatuximab-irfc inhibits the ADP-ribosyl cyclase activity of CD38. Isatuximab-irfc can activate natural killer (NK) cells in the absence of CD38-positive target tumor cells and suppresses CD38-positive T-regulatory cells.
The combination of isatuximab-irfc and pomalidomide enhanced ADCC activity and direct tumor cell killing compared to that of isatuximab-irfc alone in vitro, and enhanced antitumor activity compared to the activity of isatuximab-irfc or pomalidomide alone in a human multiple myeloma xenograft model.
In multiple myeloma patients treated with SARCLISA combined with pomalidomide and dexamethasone, a decrease in absolute counts of total NK cells (including inflammatory CD16 + low CD56 + bright and cytotoxic CD16 + bright CD56 + dim NK cells) and CD19 + B cells was observed in peripheral blood.
Up to 2 times the approved recommended dose, SARCLISA does not prolong the QT interval to any clinically relevant extent.
A relationship between isatuximab-irfc exposure and overall response rate and progression-free survival was observed.
No apparent relationship was observed between an increase of isatuximab-irfc exposure and adverse reactions.
Following the administration of isatuximab-irfc at the recommended dose and schedule, the steady state isatuximab-irfc mean (CV ) predicted maximum plasma concentration (Cmax) was 351 µg/mL (36.0) and area under the plasma concentration-time curve (AUC) was 72,600 µg∙h/mL (51.7%). The median time to reach steady state of isatuximab-irfc was 8 weeks with a 3.1-fold accumulation.
Isatuximab-irfc AUC increases in a greater than dose proportional manner over a dosage range from 1 mg/kg to 20 mg/kg (0.1 to 2 times the approved recommended dosage) every 2 weeks. Isatuximab-irfc AUC increases proportionally over a dosage range from 5 mg/kg to 20 mg/kg (0.5 to 2 times the approved recommended dosage) every week for 4 weeks followed by every 2 weeks.
The mean (CV ) predicted total volume of distribution of isatuximab-irfc is of 8.13 L (26.2).
Isatuximab-irfc is expected to be metabolized into small peptides by catabolic pathways.
Isatuximab-irfc total clearance decreased with increasing dose and with multiple doses. At steady state, the near elimination (≥99%) of isatuximab-irfc from plasma after the last dose is predicted to occur in approximately 2 months. The elimination of isatuximab-irfc was similar when given as a single agent or as combination therapy.
Isatuximab-irfc exposure (AUC) at steady state decreases with increasing body weight. The following factors have no clinically meaningful effect on the exposure of isatuximab-irfc: age (36 to 85 years, 70 patients were >75 years old), sex, race (Caucasian, Black, Asian), renal impairment (eGFR <90 mL/min/1.73 m²), and mild hepatic impairment (total bilirubin 1 to 1.5 times upper limit of normal [ULN] or aspartate amino transferase [AST] > ULN). The effect of moderate (total bilirubin >1.5 times to 3 times ULN and any AST) and severe (total bilirubin >3 times ULN and any AST) hepatic impairment on isatuximab-irfc pharmacokinetics is unknown.
No dose adjustments are recommended in these specific patient populations.
Carcinogenicity and genotoxicity studies have not been conducted with isatuximab-irfc. Fertility studies have not been conducted with isatuximab-irfc.
The efficacy and safety of SARCLISA in combination with pomalidomide and low-dose dexamethasone (Isa-Pd) were evaluated in ICARIA-MM (NCT02990338), a multicenter, multinational, randomized, open-label, 2-arm, phase 3 study in patients with relapsed and refractory multiple myeloma. Patients had received at least two prior therapies including lenalidomide and a proteasome inhibitor.
A total of 307 patients were randomized in a 1:1 ratio to receive either SARCLISA in combination with pomalidomide and low-dose dexamethasone (Isa-Pd, 154 patients) or pomalidomide and low-dose dexamethasone (Pd, 153 patients). Treatment was administered in both groups in 28-day cycles until disease progression or unacceptable toxicity. SARCLISA 10 mg/kg was administered as an intravenous infusion weekly in the first cycle and every two weeks thereafter. Pomalidomide 4 mg was taken orally once daily from day 1 to day 21 of each 28-day cycle. Low-dose dexamethasone (orally or intravenously) 40 mg (20 mg for patients ≥75 years of age) was given on days 1, 8, 15, and 22 for each 28-day cycle.
Overall, demographic and disease characteristics at baseline were similar between the two treatment groups. The median patient age was 67 years (range 36–86), 20% of patients were ≥75 years; 10% of patients entered the study with a history of COPD or asthma. The proportion of patients with renal impairment (creatinine clearance <60 mL/min/1.73 m2) was 34%. The International Staging System (ISS) stage at study entry was I in 37%, II in 36% and III in 25% of patients. Overall, 20% of patients had high-risk chromosomal abnormalities at study entry; del(17p), t(4;14) and t(14;16) were present in 12%, 8% and 2% of patients, respectively.
The median number of prior lines of therapy was 3 (range 2–11). All patients received a prior proteasome inhibitor, all patients received prior lenalidomide, and 56% of patients received prior stem cell transplantation; the majority of patients (93%) were refractory to lenalidomide, 76% to a proteasome inhibitor, and 73% to both an immunomodulator and a proteasome inhibitor.
The median duration of treatment was 41 weeks for Isa-Pd group compared to 24 weeks for Pd group.
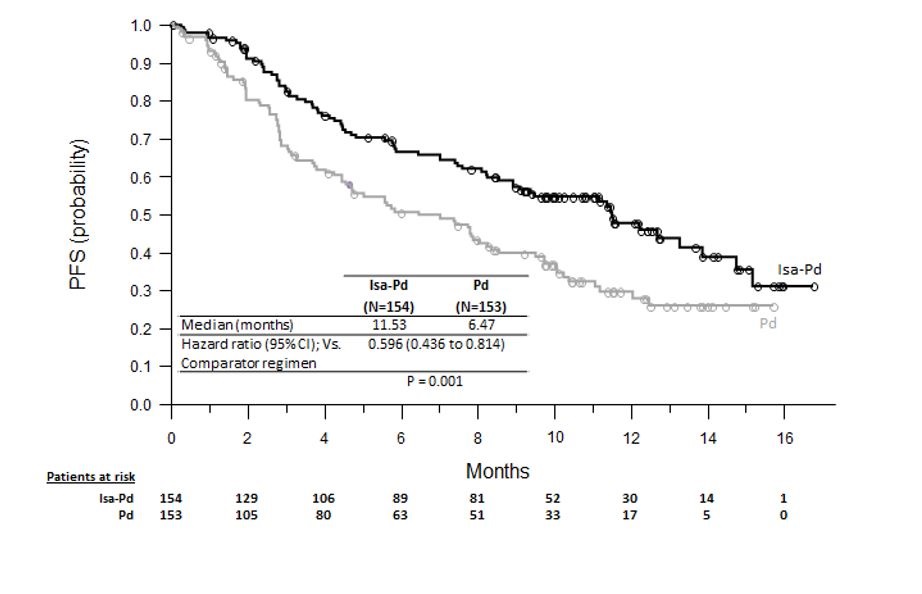
The efficacy of SARCLISA was based upon progression-free survival (PFS). PFS results were assessed by an Independent Response Committee based on central laboratory data for M-protein and central radiologic imaging review using the International Myeloma Working Group (IMWG) criteria. The improvement in PFS represented a 40% reduction in the risk of disease progression or death in patients treated with Isa-Pd.
Efficacy results are presented in Table 5 and Kaplan-Meier curve for PFS is provided in Figure 1.
Table 5. Efficacy of SARCLISA in Combination with Pomalidomide and Low-Dose Dexamethasone versus Pomalidomide and Dexamethasone in the Treatment of Multiple Myeloma (ICARIA-MM):
| Endpoint | SARCLISA + Pomalidomide + Dexamethasone | Pomalidomide + Dexamethasone |
|---|---|---|
| N=154 | N=153 | |
| Progression-Free Survival | ||
| Median (months) | 11.53 | 6.47 |
| [95% CI] | [8.94–13.9] | [4.47–8.28] |
| Hazard ratio* [95% CI] | 0.596 [0.44–0.81] | |
| p-value* (stratified log-rank test) | 0.0010 | |
| Overall Response Rate† | ||
| Responders (sCR+CR+VGPR+PR) n (%) | 93 (60.4) | 54 (35.3) |
| [95% CI]‡ | [52.2%–68.2%] | [27.8%–43.4%] |
| p-value (stratified Cochran-Mantel-Haenszel)* | <0.0001 | |
| Stringent Complete Response (sCR) + Complete Response (CR) n (%) | 7 (4.5) | 3 (2) |
| Very Good Partial Response (VGPR) n (%) | 42 (27.3) | 10 (6.5) |
| Partial Response (PR) n (%) | 44 (28.6) | 41 (26.8) |
* Stratified on age (<75 years versus ≥75 years) and number of previous lines of therapy (2 or 3 vs >3) according to IRT.
† sCR, CR, VGPR and PR were evaluated by the IRC using the IMWG response criteria.
‡ Estimated using Clopper-Pearson method.
The median time to first response in responders was 35 days in Isa-Pd group versus 58 days in Pd group. The median duration of response was 13.3 months (95% CI: 10.6-NR) in the Isa-Pd group versus 11.1 months (95% CI: 8.5-NR) in the Pd group. Median overall survival was not reached for either treatment group. At a median follow-up time of 11.6 months, 43 (27.9%) patients on Isa-Pd and 56 (36.6%) patients on Pd had died. The OS results at interim analysis did not reach statistical significance.
Figure 1. Kaplan-Meier Curves of PFS – ITT Population – ICARIA-MM (assessment by the IRC):
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.