SAVELLA Film-coated tablet Ref.[10333] Active ingredients: Milnacipran
Source: FDA, National Drug Code (US) Revision Year: 2017
12.1. Mechanism of Action
The exact mechanism of the central pain inhibitory action of milnacipran and its ability to improve the symptoms of fibromyalgia in humans are unknown. Preclinical studies have shown that milnacipran is a potent inhibitor of neuronal norepinephrine and serotonin reuptake; milnacipran inhibits norepinephrine uptake with approximately 3-fold higher potency in vitro than serotonin without directly affecting the uptake of dopamine or other neurotransmitters. Milnacipran has no significant affinity for serotonergic (5-HT1-7), α- and β-adrenergic, muscarinic (M1-5), histamine (H1-4), dopamine (D1-5), opiate, benzodiazepine, and γ-aminobutyric acid (GABA) receptors in vitro. Pharmacologic activity at these receptors is hypothesized to be associated with the various anticholinergic, sedative, and cardiovascular effects seen with other psychotropic drugs.
Milnacipran has no significant affinity for Ca++, K+, Na+ and Cl– channels and does not inhibit the activity of human monoamine oxidases (MAO-A and MAO-B) or acetylcholinesterase.
12.2. Pharmacodynamics
Cardiovascular Electrophysiology
The effect of Savella on the QTcF interval was measured in a double-blind placebo- and positive-controlled parallel study in 88 healthy subjects using 600 mg/day Savella (3 to 6 times the recommended therapeutic dose for fibromyalgia). After baseline and placebo adjustment, the maximum mean QTcF change was 8 ms (2-sided 90% CI, 3-12 ms). This increase is not considered to be clinically significant.
12.3. Pharmacokinetics
Milnacipran is well absorbed after oral administration with an absolute bioavailability of approximately 85% to 90%. The exposure to milnacipran increased proportionally within the therapeutic dose range. It is excreted predominantly unchanged in urine (55%) and has a terminal elimination half-life of about 6 to 8 hours. Steady-state levels are reached within 36 to 48 hours and can be predicted from single-dose data. The active enantiomer, d-milnacipran, has a longer elimination half-life (8-10 hours) than the l-enantiomer (4-6 hours). There is no interconversion between the enantiomers.
Absorption and Distribution
Savella is absorbed following oral administration with maximum concentrations (Cmax) reached within 2 to 4 hours post dose. Absorption of Savella is not affected by food. The absolute bioavailability is approximately 85% to 90%. The mean volume of distribution of milnacipran following a single intravenous dose to healthy subjects is approximately 400 L.
Plasma protein binding is 13%.
Metabolism and Elimination
Milnacipran and its metabolites are eliminated primarily by renal excretion. Following oral administration of 14C-milnacipran hydrochloride, approximately 55% of the dose was excreted in urine as unchanged milnacipran (24% as l-milnacipran and 31% as dmilnacipran). The lmilnacipran carbamoyl-O-glucuronide was the major metabolite excreted in urine and accounted for approximately 17% of the dose; approximately 2% of the dose was excreted in urine as d-milnacipran carbamoyl-O-glucuronide. Approximately 8% of the dose was excreted in urine as the N-desethyl milnacipran metabolite.
Pharmacokinetics in Special Populations
Renal Impairment: Milnacipran pharmacokinetics were evaluated following single oral administration of 50 mg Savella to subjects with mild (creatinine clearance [CLcr] 50-80 mL/min), moderate (CLcr 30-49 mL/min), and severe (CLcr 5-29 mL/min) renal impairment and to healthy subjects (CLcr >80 mL/min). The mean AUC0-∞ increased by 16%, 52%, and 199%, and terminal elimination half-life increased by 38%, 41%, and 122% in subjects with mild, moderate, and severe renal impairment, respectively, compared with healthy subjects.
No dosage adjustment is necessary for patients with mild renal impairment. Caution should be exercised in patients with moderate renal impairment. Dose adjustment is necessary in severe renal impairment patients [see Dosage and Administration (2.2)].
Hepatic Impairment: Milnacipran pharmacokinetics were evaluated following single oral administration of 50 mg Savella to subjects with mild (Child-Pugh A), moderate (Child-Pugh B), and severe (Child-Pugh C) hepatic impairment and to healthy subjects. AUC0-∞ and T½ were similar in healthy subjects and subjects with mild and moderate hepatic impairment. However, subjects with severe hepatic impairment had a 31% higher AUC0-∞ and a 55% higher T½ than healthy subjects. Caution should be exercised in patients with severe hepatic impairment.
Elderly: Cmax and AUC parameters of milnacipran were about 30% higher in elderly (>65 years) subjects compared with young subjects due to age-related decreases in renal function.
No dosage adjustment is necessary based on age unless renal function is severely impaired [see Dosage and Administration (2.2)].
Gender: Cmax and AUC parameters of milnacipran were about 20% higher in female subjects compared with male subjects. Dosage adjustment based on gender is not necessary.
Lactation study: In a pharmacokinetic study, a single, oral dose of 50 mg milnacipran HCl tablet was administered to 8 lactating women who were at least 12 weeks postpartum and weaning their infants. The maximum estimated daily infant dose for milnacipran from breast milk (assuming mean milk consumption of 150 mL/kg/day) was 5% of the maternal dose based on peak plasma concentrations. In most patients, peak concentrations of milnacipran in breast milk were seen within 4 hours after the maternal dose. Because of the limited data regarding infant exposure to Savella, caution should be exercised when Savella is administered to a nursing woman.
Drug-Drug Interactions
In Vitro Studies:
In general, milnacipran, at concentrations that were at least 25 times those attained in clinical trials, did not inhibit human CYP1A2, CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4 or induce human CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, and CYP3A4/5 enzyme systems, indicating a low potential of interactions with drugs metabolized by these enzymes.
In vitro studies have shown that the biotransformation rate of milnacipran by human hepatic microsomes and hepatocytes was low. A low biotransformation was also observed following incubation of milnacipran with cDNA-expressed human CYP1A2, CYP2A6, CYP2B6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4 isozymes.
In Vivo Studies:
The drug interaction studies described in this section were conducted in healthy adult subjects.
Carbamazepine: There were no clinically significant changes in the pharmacokinetics of milnacipran following co-administration of Savella (100 mg/day) and carbamazepine (200 mg twice a day). No changes were observed in the pharmacokinetics of carbamazepine or its epoxide metabolite due to co-administration with Savella.
Clomipramine: Switching from clomipramine (75 mg once a day) to milnacipran (100 mg/day) without a washout period did not lead to clinically significant changes in the pharmacokinetics of milnacipran. Because an increase in adverse events (eg, euphoria and postural hypotension) was observed after switching from clomipramine to milnacipran, monitoring of patients during treatment switch is recommended.
Digoxin: There was no pharmacokinetic interaction between Savella (200 mg/day) and digoxin (0.2 mg/day Lanoxicaps) following multiple-dose administration to healthy subjects.
Fluoxetine: Switching from fluoxetine (20 mg once a day), a strong inhibitor of CYP2D6 and a moderate inhibitor of CYP2C19, to milnacipran (100 mg/day) without a washout period did not affect the pharmacokinetics of milnacipran.
Lithium: Multiple doses of Savella (100 mg/day) did not affect the pharmacokinetics of lithium.
Lorazepam: There was no pharmacokinetic interaction between a single dose of Savella (50 mg) and lorazepam (1.5 mg).
Pregabalin: There were no clinically significant changes in the steady-state pharmacokinetics of milnacipran or pregabalin following twice a day co-administration of 50 mg milnacipran and 150 mg pregabalin.
Warfarin: Steady-state milnacipran (200 mg/day) did not affect the pharmacokinetics of R-warfarin and S-warfarin or the pharmacodynamics (as assessed by measurement of prothrombin INR) of a single dose of 25 mg warfarin. The pharmacokinetics of Savella were not altered by warfarin.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Dietary administration of milnacipran to rats at doses of 50 mg/kg/day (2 times the MRHD on a mg/m2 basis) for 2 years caused a statistically significant increase in the incidence of thyroid C-cell adenomas and combined adenomas and carcinomas in males. A carcinogenicity study was conducted in Tg.rasH2 mice for 6 months at oral gavage doses of up to 125 mg/kg/day.
Milnacipran did not induce tumors in Tg.rasH2 mice at any dose tested.
Mutagenesis
Milnacipran was not mutagenic in the in vitro bacterial reverse mutation assay (Ames test) or in the L5178Y TK +/- mouse lymphoma forward mutation assay. Milnacipran was also not clastogenic in an in vitro chromosomal aberration test in human lymphocytes or in the in vivo mouse micronucleus assay.
Impairment of Fertility
Although administration of milnacipran to male and female rats had no statistically significant effect on mating or fertility at doses up to 80 mg/kg/day (4 times the MRHD on an mg/m2 basis), there was an apparent dose-related decrease in the fertility index at clinically relevant doses based on body surface area.
13.2. Animal Toxicology and/or Pharmacology
Hepatic Effects
Chronic administration (2 years) of milnacipran to rats at 15 mg/kg (0.6 times the MRHD on an mg/m2 basis) and higher doses showed increased incidences of centrilobular vacuolation of the liver in male rats and eosinophilic foci in male and female rats in the absence of any change in hepatic enzymes. The clinical significance of the finding is not known. Chronic (1 year) administration in the primate at doses up to 25 mg/kg (2 times the MRHD on a mg/m2 basis) did not demonstrate similar evidence of hepatic changes.
Ocular Effects
Chronic (2 years) administration of milnacipran to rats at 15 mg/kg (0.6 times the MRHD on a mg/m2 basis) and higher doses showed increased incidence of keratitis of the eye. One-year studies in the rat and primate did not show this response.
14. Clinical Studies
Management of Fibromyalgia
The efficacy of Savella for the management of fibromyalgia was established in two double-blind, placebo-controlled, multicenter studies in adult patients (18-74 years of age). Enrolled patients met the of Rheumatology (ACR) criteria for fibromyalgia (a history of widespread pain for 3 months and pain present at 11 or more of the 18 specific tender point sites). Approximately 35% of patients had a history of depression. Study 1 was six months in duration and Study 2 was three months in duration.
A larger proportion of patients treated with Savella than with placebo experienced a simultaneous reduction in pain from baseline of at least 30% (VAS) and also rated themselves as much improved or very much improved based on the patient global assessment (PGIC). In addition, a larger proportion of patients treated with Savella met the criteria for treatment response, as measured by the composite endpoint that concurrently evaluated improvement in pain (VAS), physical function (SF-36 PCS), and patient global assessment (PGIC), in fibromyalgia as compared to placebo.
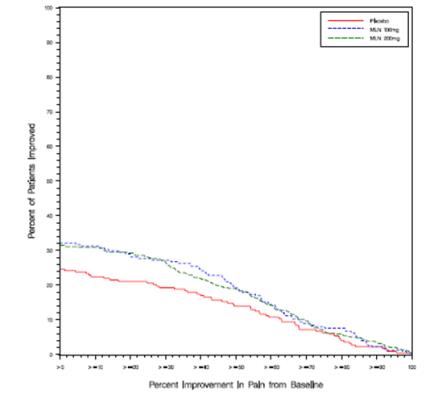
Study 1: This 6-month study compared total daily doses of Savella 100 mg and 200 mg to placebo. Patients were enrolled with a minimum mean baseline pain score of ≥50 mm on a 100 mm visual analog scale (VAS) ranging from 0 (“no pain”) to 100 (“worst possible pain”). The mean baseline pain score in this trial was 69. The efficacy results for Study 1 are summarized in Figure 1.
Figure 1 shows the proportion of patients achieving various degrees of improvement in pain from baseline to the 3-month time point and who concurrently rated themselves globally improved (PGIC score of 1 or 2). Patients who did not complete the 3-month assessment were assigned 0% improvement. More patients in the Savella treatment arms experienced at least a 30% reduction in pain from baseline (VAS) and considered themselves globally improved (PGIC) than did patients in the placebo arm. Treatment with Savella 200 mg/day did not confer greater benefit than treatment with Savella 100 mg/day.
Figure 1. Patients Achieving Various Levels of Pain Relief with Concurrent Ratings of Being Much or Very Much Improved on the PGIC ― Study 1:
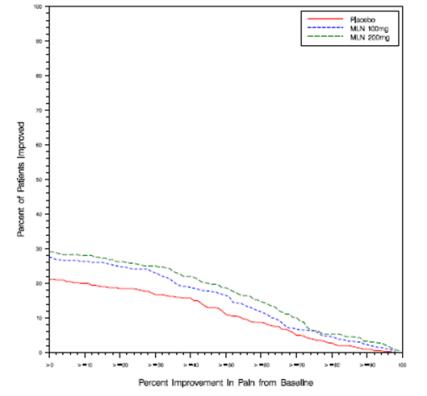
Study 2: This 3-month study compared total daily doses of Savella 100 mg and 200 mg to placebo. Patients were enrolled with a minimum mean baseline pain score of ≥40 mm on a 100-mm VAS ranging from 0 (“no pain”) to 100 (“worst possible pain”). The mean baseline pain score in this trial was 65. The efficacy results for Study 2 are summarized in Figure 2.
Figure 2 shows the proportion of patients achieving various degrees of improvement in pain from baseline to the 3-month time point and who concurrently rated themselves globally improved (PGIC score of 1 or 2). Patients who did not complete the 3-month assessment were assigned 0% improvement. More patients in the Savella treatment arms experienced at least a 30% reduction in pain from baseline (VAS) and considered themselves globally improved (PGIC) than did patients in the placebo arm. Treatment with Savella 200 mg/day did not confer greater benefit than treatment with Savella 100 mg/day.
Figure 2. Patients Achieving Various Levels of Pain Relief with Concurrent Ratings of Being Much or Very Much Improved on the PGIC ― Study 2:
In both studies, some patients who rated themselves as globally “much” or “very much” improved experienced a decrease in pain as early as week 1 of treatment with a stable dose of Savella that persisted throughout these studies.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.