SKELID Tablet Ref.[50227] Active ingredients: Tiludronic acid
Source: FDA, National Drug Code (US) Revision Year: 2010
2. Clinical Pharmacology
Mechanism of Action
In vitro studies indicate that tiludronate disodium acts primarily on bone through a mechanism that involves inhibition of osteoclastic activity with a probable reduction in the enzymatic and transport processes that lead to resorption of the mineralized matrix.
Bone resorption occurs following recruitment, activation, and polarization of osteoclasts. Tiludronate disodium appears to inhibit osteoclasts through at least two mechanisms: disruption of the cytoskeletal ring structure, possibly by inhibition of protein-tyrosine-phosphatase, thus leading to detachment of osteoclasts from the bone surface and the inhibition of the osteoclastic proton pump.
Pharmacokinetics
Absorption
Relative to an intravenous (IV) reference dose, the mean oral bioavailability of tiludronate disodium in healthy male subjects was 6% after an oral dose equivalent to 400 mg tiludronic acid administered after an overnight fast and 4 hours before a standard breakfast. In single-dose studies, bioavailability was reduced by 90% when an oral dose equivalent to 400 mg tiludronic acid was administered with, or 2 hours after, a standard breakfast compared to the same dose administered after an overnight fast and 4 hours before a standard breakfast. However, in clinical studies, efficacy was seen when SKELID was dosed at least 2 hours before or after meals.
After administration of a single dose equivalent to 400 mg tiludronic acid to healthy male subjects, tiludronic acid was rapidly absorbed with peak plasma concentrations of approximately 3 mg/L occurring within 2 hours. In pagetic patients, after repeated administration of doses equivalent to 400 mg/day tiludronic acid (2 hours before or 2 hours after a meal) for durations of 12 days to 12 weeks, average plasma concentrations of tiludronic acid occurring between 1 and 2 hours after dosing ranged between 1 and 4.6 mg/L.
Distribution
Animal pharmacology studies in rats demonstrate that tiludronic acid is widely distributed to bone and soft tissues. Over a period of days, loss of drug occurs from most tissues with the exception of bone and cartilage. Tiludronate is then slowly released from bone with a half-life in rats of 30 days or longer depending on the status of bone turnover.
After oral administration of doses equivalent to 400 mg/day tiludronic acid to nonpagetic patients with osteoarthrosis, the steady state in bone was not reached after 30 days of dosing. At plasma concentrations between 1 and 10 mg/L, tiludronic acid was approximately 90% bound to human serum protein (mainly albumin).
Metabolism
In laboratory animals, tiludronic acid undergoes little if any metabolism. In vitro, tiludronic acid is not metabolized in human liver microsomes and hepatocytes.
Elimination
The principal route of elimination of tiludronic acid is in the urine. After IV administration to healthy volunteers, approximately 60% of the dose was excreted in the urine as tiludronic acid within 13 days. Renal clearance is dose independent and is approximately 10 mL/min in healthy subjects. In pagetic patients treated with doses equivalent to 400 mg/day tiludronic acid for 12 days, the mean apparent plasma elimination half-life was approximately 150 hours. The elimination rate from human bone is unknown.
Special Populations
Geriatric
No dosage adjustment in elderly patients is necessary. Plasma concentrations of tiludronic acid were higher in elderly pagetic patients (≥65 years of age); however, this difference was not clinically significant.
Pediatric
SKELID pharmacokinetics have not been investigated in subjects under the age of 18 years.
Gender
There were no clinically significant differences in plasma concentrations after repeated administration of tiludronate disodium to male and female pagetic patients.
Race
Pharmacokinetic differences due to race have not been studied.
Renal Insufficiency
SKELID is not recommended for patients with severe renal failure (creatinine clearance <30 mL/min) due to lack of clinical experience. After a single oral dose equivalent to 400 mg tiludronic acid, subjects with creatinine clearance between 11 and 18 mL/min had Cmax values (approximately 3 mg/L) in the range of healthy volunteers. However, the plasma elimination half-life was approximately 205 hours, which is longer than that observed in pagetic patients after repeated doses (150 hours) and healthy subjects after single doses (50 hours). These values were obtained in a cross-study comparison between healthy volunteers and pagetic patients.
Hepatic Insufficiency
No dosage adjustment is needed. Since tiludronate undergoes little or no metabolism, no studies were conducted in subjects with hepatic insufficiency.
Drug-Drug Interactions
(See also PRECAUTIONS, Drug Interactions.) The bioavailability of SKELID is decreased 80% by calcium, when calcium and SKELID are administered at the same time, and 60% by some aluminum- or magnesium-containing antacids, when administered 1 hour before SKELID. Aspirin may decrease bioavailability of SKELID by up to 50% when taken 2 hours after SKELID. The bioavailability of SKELID is increased 2-4 fold by indomethacin and is not significantly altered by coadministration of diclofenac. The pharmacokinetic parameters of digoxin are not significantly modified by SKELID coadministration. In vitro studies show that tiludronate disodium does not displace warfarin from its binding site on protein.
Summary of Pharmacokinetic Parameters in the Normal Population:
| Parameter | Mean (SD) |
|---|---|
| Absolute bioavailability of two 200-mg tablets taken 4 hrs before standard breakfast | 6% (2%)* |
| Time to peak plasma concentration (taken 4 hrs before first meal of day, n=151) | 1.5 (0.9) hr |
| Maximum plasma concentration after a single 400-mg dose (taken 4 hrs before first meal of day, n=151) | 2.66 (1.22) mg/L |
| Renal clearance after IV administration of 20-mg dose | 0.54 (0.14) L/hr |
* Bioavailability was reduced by 90% when this single oral dose of 400 mg was administered with, or 2 hours after, a standard breakfast.
Pharmacodynamics
Paget’s disease of bone is a chronic, focal skeletal disorder characterized by greatly increased and disorderly bone remodeling. Excessive osteoclastic bone resorption is followed by osteoblastic new bone formation, leading to the replacement of the normal bone architecture by disorganized, enlarged, and weakened bone structure.
Clinical manifestations of Paget’s disease range from no symptoms to severe bone pain, bone deformity, pathological fractures, and neurological and other complications. Serum alkaline phosphatase, the most frequently used biochemical index of disease activity, provides an objective measure of disease severity and response to therapy.
In pagetic patients treated with SKELID 400 mg/day for 3 months, changes in urinary hydroxyproline, a biochemical marker of bone resorption, and in serum alkaline phosphatase, a marker of bone formation, indicate a reduction toward normal in the rate of bone turnover. In addition, reduced numbers of osteoclasts by histomorphometric analysis and radiological improvement of lytic lesions indicate that SKELID can suppress the pagetic disease process.
Clinical Studies
The efficacy of SKELID 400 mg/day treatment was demonstrated in two randomized, double-blind, placebo-controlled multicenter studies and one positive-controlled study. All three studies included male and female patients with Paget’s disease of the bone (radiograph examination and level of serum alkaline phosphatase [SAP] at least twice the upper normal limit). In one placebo-controlled study, conducted in North America, patients were randomly assigned to receive a daily dose of placebo or 200 or 400 mg/day SKELID for 3 months followed by an additional 12 weeks without treatment. A second placebo-controlled study of similar design was conducted in the UK.
A positive-controlled study was conducted in Europe with treatment groups of 400 mg/day SKELID for 3 months with a 3-month treatment-free follow-up, 400 mg/day SKELID for 6 months, and 400 mg/day etidronate for 6 months. In all of these studies, the efficacy of SKELID was primarily assessed by SAP activity after 3 and 6 months.
Figure 1:
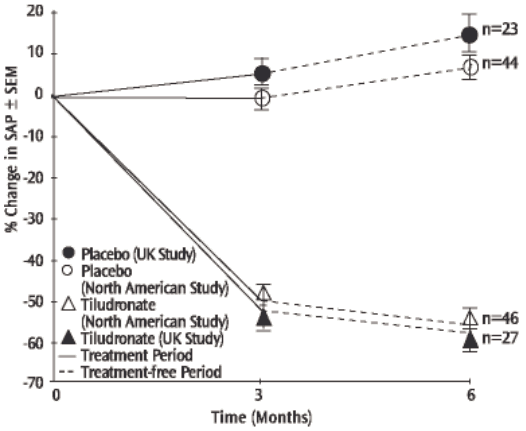
In the placebo-controlled trials, suppression of SAP levels was statistically significantly greater with 400 mg/day SKELID both at the end of treatment (3 months) and on follow-up (6 months) than with placebo (See Figure 1). The proportion of patients demonstrating at least a 50% reduction in SAP at 3 months with 400 mg/day SKELID was 61% in the North American study and 52% in the UK study.
Figure 2:
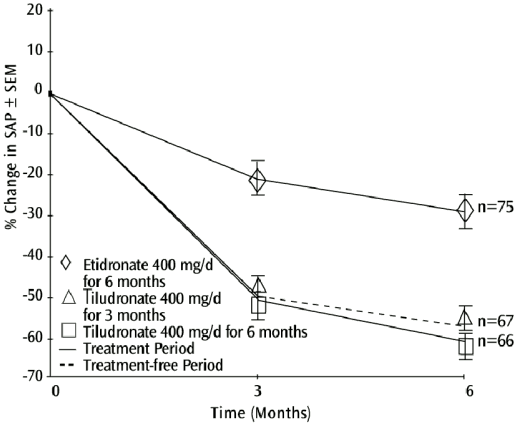
In the positive-controlled trial, six months after the start of dosing, the decrease in SAP levels in patients who ceased dosing after a 3-month course of SKELID was significantly greater than with 6 months of etidronate 400 mg/day, and was equivalent to levels in patients who completed a 6-month course of SKELID (See Figure 2).
Treatment effects of SKELID were similar, regardless of pagetic patients' baseline SAP level, gender or age in the population studied.
Histomorphometry of the bone was studied in 19 pagetic and 29 nonpagetic patients. Bone biopsy results in nonpagetic bone confirmed that SKELID did not impair bone remodeling or induce a significant decline in bone turnover. Results obtained in pagetic and nonpagetic bone indicated no evidence of osteomalacia or accumulation of unmineralized osteoid, and there was no reduction in the mineralization rate.
6.6. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not yet been completed.
Tiludronate was not genotoxic in the following assays: an in vitro microbial mutagenesis assay with and without metabolic activation, a human lymphocyte assay, a yeast cell assay for forward mutation and mitotic crossing over, or the in vivo mouse micronucleus test.
Tiludronate had no effect on rat fertility (male or female) at exposures up to two times the 400 mg/day human dose, based on surface area, mg/m² (75 mg/kg/day tiludronic acid dose).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.