Source: European Medicines Agency (EU) Revision Year: 2021 Publisher: bluebird bio (Netherlands) B.V., Stadsplateau 7, WTC Utrecht, 3521AZ Utrecht, The Netherlands
Pharmacotherapeutic group: Other nervous system drugs
ATC code: not yet assigned
Skysona adds functional copies of the ABCD1 cDNA into patients' HSCs through transduction of autologous CD34+ cells with Lenti-D LVV. After Skysona infusion, transduced CD34+ HSCs engraft in the bone marrow and differentiate into various cell types, including monocytes (CD14+) that migrate to the brain where they are believed to further differentiate into macrophages and cerebral microglia that can produce functional ALDP. The functional ALDP can then enable the local degradation of very long chain fatty acids (VLCFAs) in the brain, which in turn can stabilise the disease by preventing further inflammation and demyelination. However, it is not anticipated that Skysona treatment will affect other manifestations of ALD including adrenal insufficiency. Impact of Skysona treatment on adrenomyeloneuropathy has not been studied. Following successful engraftment with genetically modified cells, the expression of ALDP is expected to be life-long.
One month after Skysona treatment, all evaluable patients in Study ALD-102 (N=25) produced ALDP in CD14+ peripheral blood cells with a median (min, max) CD14+ ALDP+ of 29.50% (8.20%, 49.65%) demonstrating early expression of the transgene. For patients with at least 6 months of follow-up, CD14+ ALDP+ cells generally declined slightly after Skysona infusion and stabilized by approximately Month 6. Patients had a Month 6 median (min, max) CD14+ ALDP+ of 22.20 (2.00%, 71.40%) in Study ALD-102 (N=27).
The percentage of ALDP+ cells remained generally stable in CD14+ peripheral blood cells through Month 24 with a median (min, max) of 16.90% (5.80%, 44.60%) in Study ALD-102 (N=26). The percentage of CD14+ ALDP+ cells continued to be stable at last follow-up through Month 60, demonstrating long-term expression of transgenic ALDP in the progeny of haematopoietic stem cells.
The safety and efficacy of Skysona were assessed in an open-label, single-arm study in patients with CALD (ALD-102; N=32) and compared to the efficacy and safety of allo-HSCT in patients with CALD in a contemporaneous comparator study (ALD-103; N=59). All patients who completed or discontinued Study ALD-102 were asked to participate in a long-term follow-up study, LTF-304.
Enrolment in Study ALD-102 is complete with 32 patients enrolled and treated; 30 patients are evaluable for the Month 24 primary efficacy endpoint.
In addition, a second open-label, single-arm study (ALD-104; N=19) is ongoing; no patients have reached the Month 24 evaluation timepoint and thus are not included in any efficacy analyses.
All patients were administered a median dose of 10 µg/kg of G-CSF for a minimum of 4 days to mobilise stem cells prior to the apheresis procedure.
In Study ALD-102, patients were assessed on the morning after the 4th G-CSF dose. If the peripheral blood CD34+ count on that morning was <50 cells/µL, a 5th dose of G-CSF was administered and plerixafor was administered at a dose of 0.24 mg/kg of body weight approximately 10 hours prior to the next day’s apheresis collection. Plerixafor could be given daily for up to 4 days. Eleven of the 32 (34.4%) patients in Study ALD-102 received plerixafor.
For all patients, 1 cycle of mobilisation and apheresis was sufficient to collect the minimum number of CD34+ cells to manufacture Skysona.
In Study ALD-102, 32 patients received pharmacokinetically-dosed busulfan in conjunction with cyclophosphamide prior to treatment with Skysona. Busulfan was administered with a recommended cumulative AUC of 17,000 to 21,000 µmol*min/L over four days of conditioning. For patients ≤ 12 kg, busulfan was dosed at 1.1 mg/kg/dose IV every 6 hours and for patients > 12 kg busulfan was dosed at 0.8 mg/kg/dose IV every 6 hours for 4 days. Busulfan dose adjustments were made as needed based on pharmacokinetic monitoring. Patients received anti-seizure, anti-fungal, and antibiotic prophylaxis in accordance with institutional guidelines. The recommended dose of cyclophosphamide was 50 mg/kg/day. The median (min, max) daily average busulfan dose was 3.5 (2.8, 4.2) mg/kg/day (N=31) and the median (min, max) estimated average daily AUC was 4729 (4039, 5041) µmol*min/L/day (N=31).
In Study ALD-104, 19 patients received pharmacokinetically-dosed busulfan in conjunction with fludarabine prior to treatment with Skysona. Skysona administration All patients were administered Skysona as an intravenous infusion with a median (min, max) dose of 11.78 (5.0, 38.2) × 106 CD34+ cells/kg (N=51).
In Study ALD-102, patients received G-CSF at the investigator’s discretion per institutional practice following treatment with Skysona. Of the 32 treated patients, 24 received G-CSF following treatment with Skysona.
In Study ALD-104, patients were to receive G-CSF beginning on Day 5 following treatment with Skysona.
Study ALD-102 was an open-label, single-arm, 24-month study that included a total of 32 patients with CALD treated with Skysona. In study ALD-102, early CALD was defined as: a Loes score between 0.5 and 9 (inclusive), gadolinium enhancement on MRI of demyelinating lesions and a neurologic function score (NFS) of ≤1, indicating limited changes in neurologic function. Patients were excluded from Study ALD-102 if they had a willing and available HLA-matched sibling HSC donor. The median (min, max) age at Skysona infusion was 6.0 (4, 14) years, 100% of patients were males, and 46.9% were White/Caucasian. The median (min, max) Loes score at baseline was 2.00 (1.0, 9.0). Of the 32 patients, 31 had an NFS of 0 and one had an NFS of 1 at baseline. All patients that completed ALD-102 enrolled for long-term follow-up in the LTF-304 study. The median (min, max) duration of follow-up was 38.59 (13.4, 82.7) months.
The primary efficacy endpoint was the proportion of patients who had none of the 6 Major Functional Disabilities (MFDs), were alive, did not receive a second allo-HSCT or rescue cell administration, and had not withdrawn or been lost to follow-up at Month 24 (i.e., Month 24 MFD-free survival). The 6 MFDs are: loss of communication, cortical blindness, tube feeding, total incontinence, wheelchair dependence, or complete loss of voluntary movement.
An analysis was conducted after 30 patients were evaluable for the primary efficacy endpoint, Month 24 MFD-free survival. Twenty-seven out of 30 patients (90%, 95% CI: 73.5, 97.9) achieved Month 24 MFDfree survival, with the lower bound of 95% CI above the clinically meaningful benchmark (Month 24 MFD-free survival rate of 50%) indicating that treatment with Skysona provides clinically meaningful benefits by preserving motor function and communication ability and improves survival when compared to untreated patients at an early stage of cerebral disease.
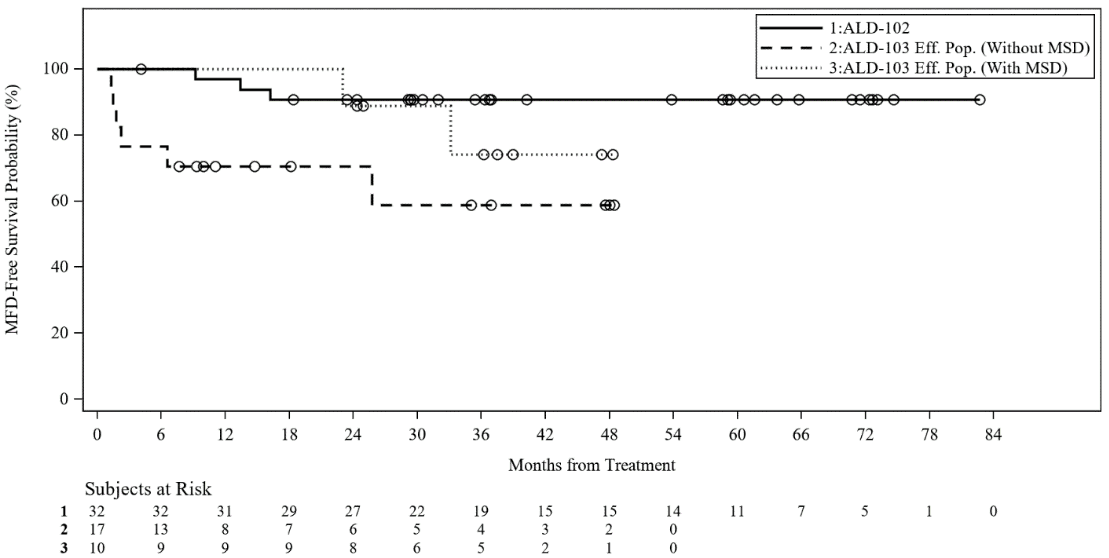
A contemporaneous comparator study was conducted in 59 patients with CALD treated with allo-HSCT (ALD-103 Safety Population). A subset of 27 patients (ALD-103 Efficacy Population) was matched to the ALD-102 population for baseline Loes score, presence of contrast enhancement and NFS score. This population was further divided into those who received an allo-HSCT from a matched sibling donor (N=10; ALD-103 Efficacy Population with MSD) and those who received an allo-HSCT from an alternative donor source, i.e., not a matched sibling donor (N=17; ALD-103 Efficacy Population without MSD).
MFD-free survival over time and overall survival were analysed in 32 patients in ALD-102 and compared to 17 patients treated with allo-HSCT in the ALD-103 Efficacy Population (without MSD), which are presented in Table 4 and Figure 1.
Skysona showed a durable effect on MFD-free survival, with most patients (26/27, 96.3%) that enrolled in LTF-304 remaining alive and maintaining their MFD-free status through their last follow-up on study, including 14 patients with 5 or more years of follow-up. One patient refused further follow-up.
Table 4. Efficacy Endpoints:
| ALD-102 Skysona Treateda (N=32) | ALD-103 Allo-HSCT Efficacy Populationb (N=27) | ALD-103 Allo-HSCT Efficacy Populationc without MSD (N=17) | ALD-103 Allo-HSCT Efficacy Populationd with MSD (N=10) | |
|---|---|---|---|---|
| Proportion of MFD-Free Survivale at Month 24 | ||||
| Evaluable Patientsf n % [95% CI] | 30 27 90.0% [73.5, 97.9] | 18 14 77.8% [52.4, 93.6] | 9 6 66.7% [29.9, 92.5] | 9 8 88.9% [51.8, 99.7] |
| Number of Patients with Events by Month 24g | ||||
| n % | 3 9.4% | 8 29.6% | 6 35.3% | 2 20.0% |
| Number of Surviving Patients by Month 24h | ||||
| n % [95% CI] | 31 96.6% [77.9, 99.5] | 22 86.2% [62.6, 95.4] | 14 86.3% [54.7, 96.5] | 8 88.9% [43.3, 98.4] |
a entry criteria included elevated VLCFA values, a Loes score between 0.5 and 9 (inclusive), gadolinium enhancement on MRI of demyelinating lesions, NFS of ≤1 and no willing and available HLA-matched sibling HSC donor
b matched to the ALD-102 population for baseline Loes score, presence of contrast enhancement, and NFS score
c matched to the ALD-102 population for baseline Loes score, presence of contrast enhancement, and NFS score and no willing and available HLA-matched sibling HSC donor
d matched to the ALD-102 population for baseline Loes score, presence of contrast enhancement, and NFS score and had an HLA-matched sibling HSC donor
e Primary efficacy endpoint; proportion of patients with no event by Month 24; includes death, MFD, rescue cell administration, or subsequent allo-HSCT
f ALD-102 and ALD-103 Month 24 Evaluable Subjects for MFD-free Survival are defined as treated subjects who had been followed for 24 months, or had completed the Month 24 Visit, or had discontinued from the studies (for any reason, including death) but would have been followed for 24 months if still in the study, at the time of the data cut for these analyses
g Time-to-event Kaplan-Meier analysis; includes death, MFD, rescue cell administration, or subsequent allo-HSCT
h Time-to-event Kaplan-Meier analysis; includes death only
MSD = matched sibling donor.
Figure 1. Kaplan-Meier Curve of MFD-free Survival Between ALD-102 (Skysona Treated) and ALD-103 Efficacy Population (without MSD and with MSD):
The neurologic function score (NFS) was used as a secondary endpoint to evaluate 15 domains of neurological function; it has a total maximum score of 25. A score of 0 denotes no abnormality in the assessed areas of neurological function. At baseline, patients were required to have an NFS ≤1. In ALD-102, 26 of 28 evaluable patients maintained an NFS less than or equal to 1 through Month 24 and 24 of those patients had no change in their NFS, which showed maintenance of neurological function in the majority of patients. The majority of patients in ALD-102 maintained cognitive function (IQ, including performance IQ sub-measures) within the normal range (100 ± 15 points), with minimal decline and with stabilization by Month 24. A small subgroup of patients who had higher Loes scores at baseline tended to have a less favourable outcome.
The primary safety endpoint, the proportion of evaluable patients who experienced either acute (≥ Grade II) or chronic graft versus host disease (GVHD) in ALD-102 vs. ALD-103 by Month 24, was 0 vs. 52%.
The proportion of all patients who experienced either acute (≥ Grade II) or chronic GVHD in ALD102/ALD-104 vs. ALD-103 is summarized in Table 5.
Table 5. Graft Versus Host Disease:
| Skysona treated | Allo-HSCT | ||
|---|---|---|---|
| ALD-102 (N=32) | ALD-102/104 (N=51) | ALD-103 Safety Populationa (N=59) | |
| Acute (≥ Grade II) GVHD or Chronic GVHD | |||
| n % [95% CI] | 0 0% [0.0, 10.9] | 0 0% [0.0, 7.0] | 26 44.1% [31.2, 57.6] |
| Acute (≥ Grade II) GVHD | |||
| n % [95% CI] | 0 0% [0, 10.9] | 0 0% [0.0, 7.0] | 15 25.4% [15.0, 38.4] |
| Chronic GVHD | |||
| n % [95% CI] | 0 0% [0, 10.9] | 0 0% [0.0, 7.0] | 14 23.7% [13.6, 36.6] |
a For censored observations in the ALD-103 Safety Population, it was assumed that no GVHD was observed in any category.
Neutrophil engraftment was monitored as a secondary endpoint and was defined as achieving 3 consecutive absolute neutrophil counts (ANC) ≥500 cells/µL obtained on different days by Day 43 after Skysona infusion. In clinical studies neutrophil engraftment occurred on median (min, max) Day 13 (11, 41) after Skysona infusion (see section 4.4) (N=32, ALD-102; N=17, ALD-104) compared to Day 17 (12, 36) in ALD-103 (N=53).
No primary or secondary neutrophil engraftment failure was observed in subjects in ALD-102/ALD-104 (N=51), compared to 10/59 (16.9%) subjects in ALD-103.
Platelet engraftment was monitored as a secondary endpoint and was defined as achieving 3 consecutive unsupported platelet counts of ≥20 × 109 cells/L obtained on different days after Skysona infusion, with no platelet transfusions administered for 7 days immediately preceding and during the evaluation period. In clinical studies, platelet engraftment occurred on median (min, max) Day 32 (14, 108) after Skysona infusion (N=32, ALD-102; N=15, ALD-104) compared to Day 26 (13, 67) in ALD-103 (N=47).
No patients experienced transplant-related mortality (TRM), a secondary endpoint, at 100 days or 365 days after transplant in ALD-102 and ALD-104. In contrast, 2/59 (3.4%) patients experienced TRM at 100 days and 8/59 (13.6%) patients experienced TRM at 365 days after transplant in the ALD-103 Safety Population.
Skysona is an autologous gene therapy medicinal product consisting of autologous cells that have been genetically modified ex vivo. The nature of Skysona is such that conventional studies on pharmacokinetics, absorption, distribution, metabolism, and elimination are not applicable.
Conventional mutagenicity, carcinogenicity and reproductive and developmental toxicity studies have not been conducted.
The pharmacology, toxicology and genotoxicity of the Lenti-D LVV used for transduction were evaluated in vitro and in vivo. In an in vitro immortalization assay, Lenti-D LVV-transduced mouse bone marrow cells showed strongly reduced mutagenic potential as compared to positive control vectors. Integration site analysis of pre-transplantation Lenti-D LVV-transduced human CD34+ HSCs demonstrated the expected self-inactivating LVV integration profile, with no enrichment for insertion in or near cancerrelated genes.
A pivotal GLP-compliant combined toxicity, genotoxicity and biodistribution study of Lenti-D LVV-transduced mobilized peripheral blood CD34+ HSCs was conducted in myeloablated immunodeficient mice. There was no evidence of toxicity, genotoxicity (insertional mutagenesis resulting in oncogenic mutations) or oncogenesis (tumorigenicity) related to Lenti-D LVV integration. Integration site analysis of post-transplantation bone marrow cells demonstrated no preferred integration in the proximity of or within cancer-related genes. An additional study with Lenti-D LVV-transduced human CD34+ HSCs administered to myeloablated, immunodeficient mice demonstrated engraftment of humanorigin microglial cells within brain tissues with no toxicity or tumorigenicity.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.