SYLVANT Powder for concentrate for solution for infusion Ref.[8887] Active ingredients: Siltuximab
Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: EUSA Pharma (Netherlands) B.V., Johannes Vermeerplein 11, 1071 DV, Amsterdam, Netherlands
Pharmacodynamic properties
Pharmacotherapeutic group: Immunosuppresants, interleukin inhibitors
ATC code: L04AC11
Mechanism of action
Siltuximab is a human-mouse chimeric monoclonal antibody that forms high affinity, stable complexes with soluble bioactive forms of human IL-6. Siltuximab prevents the binding of human IL-6 to both soluble and membrane-bound IL-6 receptors (IL-6R), thus inhibiting the formation of the hexameric signaling complex with gp130 on the cell surface. Interleukin-6 is a pleiotropic pro-inflammatory cytokine produced by a variety of cell types including T-cells and B-cells, lymphocytes, monocytes and fibroblasts, as well as malignant cells. IL-6 has been shown to be involved in diverse normal physiologic processes such as induction of immunoglobulin secretion, initiation of hepatic acute phase protein synthesis, and stimulation of hematopoietic precursor cell proliferation and differentiation. Overproduction of IL-6, in chronic inflammatory diseases and malignancies has been linked to anaemia and cachexia and has been hypothesised to play a central role in driving plasma cell proliferation and systemic manifestations in patients with CD.
Pharmacodynamic effects
In vitro, siltuximab dose-dependently inhibited the growth of an IL-6-dependent murine plasmacytoma cell line in response to human IL-6. In cultures of human hepatoma cells, IL-6-stimulated production of the acute-phase protein serum amyloid A was dose-dependently inhibited by siltuximab. Similarly, in cultures of human Burkitt's B-lymphoma cells, the production of immunoglobulin M protein in response to IL-6 was dose-dependently inhibited by siltuximab.
Biomarkers
It is well established that IL-6 stimulates the acute-phase expression of C-reactive protein (CRP). The mechanism of action of siltuximab is neutralisation of IL-6 bioactivity, which can be measured indirectly by suppression of CRP. Siltuximab treatment in MCD results in rapid and sustained decreases in CRP serum concentrations. Measurement of IL-6 concentrations in serum or plasma during treatment should not be used as a pharmacodynamic marker, as siltuximab-neutralised antibody-IL-6 complexes interfere with current immunological-based IL-6 quantification methods.
Clinical efficacy and safety
Study 1
A Phase 2, multinational, randomised (2:1) double-blind, placebo-controlled study was conducted to assess the efficacy and safety of siltuximab (11 mg/kg every 3 weeks) compared with placebo in combination with best supportive care in patients with MCD. Treatment was continued until treatment failure (defined as disease progression based on increase in symptoms, radiologic progression or deterioration in performance status) or unacceptable toxicity. A total of 79 patients with symptomatic MCD were randomised and treated. Median age was 47 years (range 20-74) in the siltuximab arm and 48 years (range 27-78) in the placebo arm. More male patients were enrolled in the placebo arm (85% in placebo vs. 56% in the siltuximab group). ECOG performance status score (0/1/2) at baseline was 42%/45%/13% in the siltuximab arm and 39%/62%/0% in the placebo arm, respectively. At baseline, 55% of patients in the siltuximab arm and 65% of patients in the placebo arm had received prior systemic therapies for MCD and 30% of patients in the siltuximab arm and 31% in the placebo arm were using corticosteroids. Histological subtype was similar in both treatment arms, with 33% hyaline vascular subtype, 23% plasmacytic subtype and 44% mixed subtype. The primary endpoint of the study was durable tumour and symptomatic response, defined as tumour response assessed by independent review and complete resolution or stabilisation of prospectively collected MCD symptoms, for at least 18 weeks without treatment failure.
In Study 1 a statistically significant difference in independently reviewed durable tumour and symptomatic response rate in the siltuximab arm compared with the placebo arm (34% vs. 0%, respectively; 95% CI: 11.1, 54.8; p=0.0012) was observed. The overall tumour response rate was evaluated based on modified Cheson criteria both by independent review and investigator assessment.
Key efficacy results from Study 1 are summarised in Table 3.
Table 3. Efficacy endpoints from study 1:
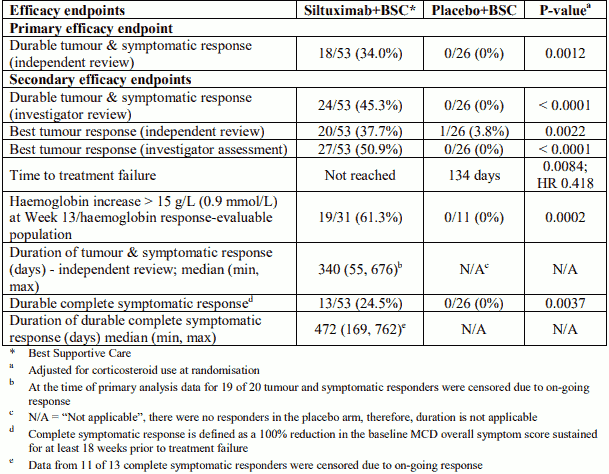
MCD-related signs and symptoms were prospectively collected. A total score of all symptoms (referred to as the MCD-related Overall Symptom Score) is the sum of the severity grades (NCI-CTCAE grade) of the MCD-related signs and symptoms [general MCD-related (fatigue, malaise, hyperhidrosis, night sweats, fever, weight loss, anorexia, tumour pain, dyspnea, and pruritus), autoimmune phenomena, fluid retention, neuropathy, and skin disorders]. The percent change from baseline in MCD-related signs and symptoms and MCD-related overall symptom score at each cycle was calculated. Complete symptom response was defined as a 100% reduction from the baseline overall in the MCD-related overall symptom score sustained for at least 18 weeks prior to treatment failure.
Haemoglobin response was defined as a change from baseline of ≥15 g/L (0.9 mmol/L) at Week 13. A statistically significant difference (61.3% vs. 0% respectively; p=0.0002) in the haemoglobin response in the siltuximab arm compared with the placebo arm was observed.
Subgroup analyses
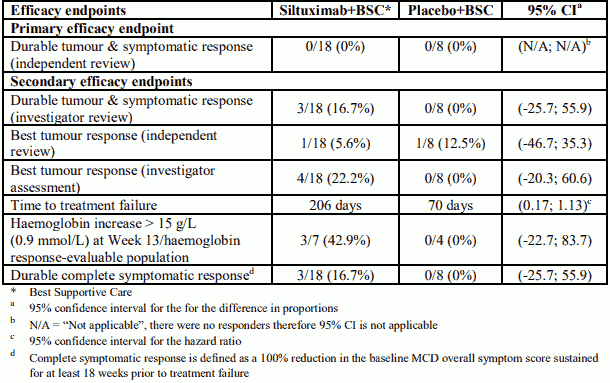
Analyses for both primary and secondary endpoints on various subgroups including age (<65 years and ≥65 years); race (White and Non-White); region (North America, Europe, Middle East and Africa, and Asia Pacific); baseline corticosteroid use (yes and no); prior therapy (yes and no); and MCD histology (plasmatic and mixed histology) consistently showed that the treatment effect favoured the siltuximab arm except for the hyaline vascular subgroup in which no patient achieved the definition of the primary endpoint. A consistent treatment effect favouring siltuximab treated patients across all major secondary endpoints was shown in the hyaline vascular subgroup. Select efficacy results from Study 1 in the hyaline vascular subgroup are summarised in Table 4.
Table 4. Select efficacy endpoints for hyaline vascular subgroup from study 1:
Study 2
In addition to Study 1, efficacy data are available in patients with CD from a single arm Phase 1 study (Study 2). In this study 37 patients with CD (35 MCD patients) were treated with siltuximab. In the 16 patients with MCD treated with 11 mg/kg every 3 weeks, overall tumour response rate by independent review was 43.8% with 6.3% complete response. All tumour responses were durable for >18 weeks. In this study, 16 of the 35 MCD patients were hyaline vascular subtype; 31% of these patients had a radiologic response based on independent review and 88% showed clinical benefit response as defined in the protocol.
Study 3
An open-label, multicentre, non-randomised Phase 2 study assessed the safety and efficacy of extended treatment with siltuximab in 60 patients with MCD who were previously enrolled in Study 1 (41 patients) or Study 2 (19 patients). Median duration of siltuximab treatment was 5.52 years (range: 0.8 to 10.8 years); more than 50% of patients received siltuximab treatment for ≥5 years. After a median of 6 years of follow-up, none of the 60 patients had died and maintenance of disease control was demonstrated in 58 of 60 patients.
Highest total dose in clinical trials
The highest total amount of siltuximab administered in any clinical trial so far per dose was 2,190 mg (11 mg/kg).
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with siltuximab in all subsets of the paediatric population in CD (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
Following the first administration of siltuximab (doses ranging from 0.9 to 15 mg/kg), the area under the concentration-time curve (AUC) and maximal serum concentration (Cmax) increased in a dose-proportional manner and clearance (CL) was independent of dose. Following the single dose administration at the recommended dose regimen (11 mg/kg given once every 3 weeks), the clearance was 3.54 ± 0.44 mL/kg/day and half-life was 16.3 ± 4.2 days. Following the repeat dose administration at the recommended dose, siltuximab clearance was found to be time-invariant, and systemic accumulation was moderate (accumulation index of 1.7). Consistent with half-life after the first dose, serum concentrations reached steady-state levels by the sixth infusion (intervals every 3 weeks) with mean (± SD) peak and trough concentrations of 332 ± 139 and 84 ± 66 mcg/mL, respectively.
Immunogenicity
As with all therapeutic proteins, there is potential for the generation of anti-medicine antibodies (immunogenicity). The immunogenicity of siltuximab has been evaluated using antigen-bridging enzyme immunoassay (EIA) and electrochemiluminescence (ECL)-based immunoassay (ECLIA) methods.
In clinical studies including monotherapy and combination studies, samples from a total of 432 patients were available for anti-siltuximab antibody testing with 189 patients having at least one sample tested with the high medicinal product-tolerant ECLIA assay. The incidence rate of detectable anti-siltuximab antibodies was 0.9% (4/432) overall and 2.1% (4/189) in patients with at least once sample tested with the high medicinal product tolerant ECLIA assay. Further immunogenicity analyses were conducted for all positive samples from the 4 patients with detectable anti-siltuximab antibodies. None of these patients had neutralising antibodies. No evidence of altered safety or efficacy was identified in the patients who developed antibodies to siltuximab.
Special populations
Cross-study population PK analyses were performed using data from 378 patients with a variety of conditions who received single-agent siltuximab at doses ranging from 0.9 to 15 mg/kg. The effects of various covariates on siltuximab PK were assessed in the analyses.
Siltuximab clearance increased with increasing body weight; however, no dose adjustment is required for body weight since administration is on an mg/kg basis. The following factors had no clinical effect on the clearance of siltuximab: gender, age, and ethnicity. The effect of anti-siltuximab antibody status was not examined, as there were insufficient numbers of anti-siltuximab antibody positive patients.
Elderly
The population PK of siltuximab were analysed to evaluate the effects of demographic characteristics. The results showed no significant difference in the PK of siltuximab in patients older than 65 years compared to patients age 65 years or younger.
Renal impairment
No formal study of the effect of renal impairment on the pharmacokinetics of siltuximab has been conducted. For patients with baseline calculated creatinine clearance of 12 mL/min or greater, there was no meaningful effect on siltuximab PK. Four patients with severe renal impairment (creatinine clearance 12 to 30 mL/min) were included in the data set.
Hepatic impairment
No formal study of the effect of hepatic impairment on the pharmacokinetics of siltuximab has been conducted. For patients with baseline alanine transaminase up to 3.7 times the upper limit of normal baseline albumin ranging from 15 to 58 g/L, and baseline bilirubin ranging from 1.7 to 42.8 mg/dL there was no meaningful effect on siltuximab PK.
Paediatric population
The safety and efficacy of siltuximab have not been established in paediatric patients.
Preclinical safety data
The repeat-dose toxicology studies conducted in young cynomolgus monkeys at doses of 9.2 and 46 mg/kg/week (up to 22-fold greater exposure than in patients receiving 11 mg/kg every 3 weeks) with siltuximab showed no signs indicative of toxicity. A slight reduction in T-cell dependent antibody response and a reduction in the size of the splenic germinal centers following Keyhole limpet hemocyanin (KLH) immunisation was observed which were considered to be pharmacological responses of IL-6 inhibition and not of toxicological significance.
Siltuximab (9.2 and 46 mg/kg/week) did not produce any toxicity of the reproductive tract in cynomolgus monkeys. In mice dosed subcutaneously with an anti-mouse IL-6 monoclonal antibody, no effects on male or female fertility were observed.
During an embryo-fetal development study where siltuximab was administered intravenously to pregnant cynomolgus monkeys (gestation day 20-118) at doses of 9.2 and 46 mg/kg/week, no maternal or fetal toxicity was observed. Siltuximab crossed the placenta during gestation whereby fetal serum concentrations of siltuximab at gestation day (GD) 140 were similar to maternal concentrations. Histopathological examination of lymphoid tissues from GD140 fetuses showed no morphological abnormalities in the development of the immune system.
Rodent carcinogenicity studies have not been conducted with siltuximab. Evidence from studies conducted with siltuximab and other IL-6 inhibitors suggest that the potential for siltuximab to cause carcinogenicity is low. However, there is also evidence to suggest that IL-6 inhibition may suppress immune responses, immune surveillance and lower defense against established tumours. Therefore, an increased susceptibility to specific tumours cannot be entirely ruled out.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.