Source: FDA, National Drug Code (US) Revision Year: 2021
The mechanism of action of olanzapine and fluoxetine in the listed indications, is unclear. However, the combined effect of olanzapine and fluoxetine at the monoaminergic neural systems (serotonin, norepinephrine, and dopamine) could be responsible for the pharmacological effect.
Olanzapine binds with high affinity to the following receptors: serotonin 5HT2A/2C, 5HT6 (Ki=4, 11, and 5 nM, respectively), dopamine D1-4 (Ki=11 to 31 nM), histamine H1 (Ki=7 nM), and adrenergic α1 receptors (Ki=19 nM). Olanzapine is an antagonist with moderate affinity binding for serotonin 5HT3 (Ki=57 nM) and muscarinic M1-5 (Ki=73, 96, 132, 32, and 48 nM, respectively). Olanzapine binds weakly to GABAA, BZD, and β-adrenergic receptors (Ki>10 μM). Fluoxetine is an inhibitor of the serotonin transporter and is a weak inhibitor of the norepinephrine and dopamine transporters.
Fluoxetine (administered as a 60 mg single dose or 60 mg daily for 8 days) caused a small increase in the mean maximum concentration of olanzapine (16%) following a 5 mg dose, an increase in the mean area under the curve (17%) and a small decrease in mean apparent clearance of olanzapine (16%). In another study, a similar decrease in apparent clearance of olanzapine of 14% was observed following olanzapine doses of 6 or 12 mg with concomitant fluoxetine doses of 25 mg or more. The decrease in clearance reflects an increase in bioavailability. The terminal half-life is not affected, and therefore the time to reach steady state should not be altered. The overall steady-state plasma concentrations of olanzapine and fluoxetine when given as the combination in the therapeutic dose ranges were comparable with those typically attained with each of the monotherapies. The small change in olanzapine clearance, observed in both studies, likely reflects the inhibition of a minor metabolic pathway for olanzapine via CYP2D6 by fluoxetine, a potent CYP2D6 inhibitor, and was not deemed clinically significant. Therefore, the pharmacokinetics of the individual components is expected to reasonably characterize the overall pharmacokinetics of the combination.
Following a single oral 12 mg/50 mg dose of SYMBYAX, peak plasma concentrations of olanzapine and fluoxetine occur at approximately 4 and 6 hours, respectively. The effect of food on the absorption and bioavailability of SYMBYAX has not been evaluated. The bioavailability of olanzapine given as Zyprexa, and the bioavailability of fluoxetine given as Prozac were not affected by food. It is unlikely that there would be a significant food effect on the bioavailability of SYMBYAX.
Olanzapine is well absorbed and reaches peak concentration approximately 6 hours following an oral dose. Food does not affect the rate or extent of olanzapine absorption when olanzapine is given as Zyprexa. It is eliminated extensively by first pass metabolism, with approximately 40% of the dose metabolized before reaching the systemic circulation.
Following a single oral 40 mg dose, peak plasma concentrations of fluoxetine from 15 to 55 ng/mL are observed after 6 to 8 hours. Food does not appear to affect the systemic bioavailability of fluoxetine given as Prozac, although it may delay its absorption by 1 to 2 hours, which is probably not clinically significant.
The in vitro binding to human plasma proteins of olanzapine and fluoxetine in combination is similar to the binding of the individual components.
Olanzapine is extensively distributed throughout the body, with a volume of distribution of approximately 1000 L. It is 93% bound to plasma proteins over the concentration range of 7 to 1100 ng/mL, binding primarily to albumin and α1-acid glycoprotein.
Over the concentration range from 200 to 1000 ng/mL, approximately 94.5% of fluoxetine is bound in vitro to human serum proteins, including albumin and α1-glycoprotein. The interaction between fluoxetine and other highly protein-bound drugs has not been fully evaluated [see Drug Interactions (7.7)].
SYMBYAX therapy yielded steady-state concentrations of norfluoxetine similar to those seen with fluoxetine in the therapeutic dose range.
Olanzapine displays linear pharmacokinetics over the clinical dosing range. Its half-life ranges from 21 to 54 hours (5th to 95th percentile; mean of 30 hr), and apparent plasma clearance ranges from 12 to 47 L/hr (5th to 95th percentile; mean of 25 L/hr). Administration of olanzapine once daily leads to steady-state concentrations in about 1 week that are approximately twice the concentrations after single doses. Plasma concentrations, half-life, and clearance of olanzapine may vary between individuals on the basis of smoking status, gender, and age [see Dosage and Administration (2.3) and Clinical Pharmacology (12.4)].
Following a single oral dose of 14C-labeled olanzapine, 7% of the dose of olanzapine was recovered in the urine as unchanged drug, indicating that olanzapine is highly metabolized. Approximately 57% and 30% of the dose was recovered in the urine and feces, respectively. In the plasma, olanzapine accounted for only 12% of the AUC for total radioactivity, indicating significant exposure to metabolites. After multiple dosing, the major circulating metabolites were the 10-N-glucuronide, present at steady state at 44% of the concentration of olanzapine, and 4′-N-desmethyl olanzapine, present at steady state at 31% of the concentration of olanzapine. Both metabolites lack pharmacological activity at the concentrations observed.
Direct glucuronidation and CYP450-mediated oxidation are the primary metabolic pathways for olanzapine. In vitro studies suggest that CYP1A2, CYP2D6, and the flavin-containing monooxygenase system are involved in olanzapine oxidation. CYP2D6-mediated oxidation appears to be a minor metabolic pathway in vivo, because the clearance of olanzapine is not reduced in subjects who are deficient in this enzyme.
Fluoxetine is a racemic mixture (50/50) of R-fluoxetine and S-fluoxetine enantiomers. In animal models, both enantiomers are specific and potent serotonin uptake inhibitors with essentially equivalent pharmacologic activity. The S-fluoxetine enantiomer is eliminated more slowly and is the predominant enantiomer present in plasma at steady state.
Fluoxetine is extensively metabolized in the liver to its only identified active metabolite, norfluoxetine, via the CYP2D6 pathway. A number of unidentified metabolites exist.
In animal models, Snorfluoxetine is a potent and selective inhibitor of serotonin uptake and has activity essentially equivalent to R or S-fluoxetine. R-norfluoxetine is significantly less potent than the parent drug in the inhibition of serotonin uptake. The primary route of elimination appears to be hepatic metabolism to inactive metabolites excreted by the kidney.
The complexity of the metabolism of fluoxetine has several consequences that may potentially affect the clinical use of SYMBYAX.
A subset (about 7%) of the population has reduced activity of the drug metabolizing enzyme CYP2D6. Such individuals are referred to as “poor metabolizers” of drugs such as debrisoquin, dextromethorphan, and the tricyclic antidepressants (TCAs). In a study involving labeled and unlabeled enantiomers administered as a racemate, these individuals metabolized S-fluoxetine at a slower rate and thus achieved higher concentrations of S-fluoxetine. Consequently, concentrations of S-norfluoxetine at steady state were lower. The metabolism of R-fluoxetine in these poor metabolizers appears normal. When compared with normal metabolizers, the total sum at steady state of the plasma concentrations of the 4 enantiomers was not significantly greater among poor metabolizers. Thus, the net pharmacodynamic activities were essentially the same. Alternative nonsaturable pathways (non-CYP2D6) also contribute to the metabolism of fluoxetine. This explains how fluoxetine achieves a steady-state concentration rather than increasing without limit.
Because the metabolism of fluoxetine, like that of a number of other compounds including TCAs and other selective serotonin antidepressants, involves the CYP2D6 system, concomitant therapy with drugs also metabolized by this enzyme system (such as the TCAs) may lead to drug interactions [see Drug Interactions (7.7)].
The relatively slow elimination of fluoxetine (elimination half-life of 1 to 3 days after acute administration and 4 to 6 days after chronic administration) and its active metabolite, norfluoxetine (elimination half-life of 4 to 16 days after acute and chronic administration), leads to significant accumulation of these active species in chronic use and delayed attainment of steady state, even when a fixed dose is used. After 30 days of dosing at 40 mg/day, plasma concentrations of fluoxetine in the range of 91 to 302 ng/mL and norfluoxetine in the range of 72 to 258 ng/mL have been observed. Plasma concentrations of fluoxetine were higher than those predicted by single-dose studies, because the metabolism of fluoxetine is not proportional to dose. However, norfluoxetine appears to have linear pharmacokinetics. Its mean terminal half-life after a single dose was 8.6 days and after multiple dosing was 9.3 days. Steady-state levels after prolonged dosing are similar to levels seen at 4 to 5 weeks.
The long elimination half-lives of fluoxetine and norfluoxetine assure that, even when dosing is stopped, active drug substance will persist in the body for weeks (primarily depending on individual patient characteristics, previous dosing regimen, and length of previous therapy at discontinuation). This is of potential consequence when drug discontinuation is required or when drugs are prescribed that might interact with fluoxetine and norfluoxetine following the discontinuation of fluoxetine.
Based on the individual pharmacokinetic profiles of olanzapine and fluoxetine, the pharmacokinetics of SYMBYAX may be altered in geriatric patients. Caution should be used in dosing the elderly, especially if there are other factors that might additively influence drug metabolism and/or pharmacodynamic sensitivity.
In a study involving 24 healthy subjects, the mean elimination half-life of olanzapine was about 1.5 times greater in elderly subjects (≥65 years of age) than in non-elderly subjects (<65 years of age).
The disposition of single doses of fluoxetine in healthy elderly subjects (≥65 years of age) did not differ significantly from that in younger normal subjects. However, given the long half-life and nonlinear disposition of the drug, a single-dose study is not adequate to rule out the possibility of altered pharmacokinetics in the elderly, particularly if they have systemic illness or are receiving multiple drugs for concomitant diseases. The effects of age upon the metabolism of fluoxetine have been investigated in 260 elderly but otherwise healthy depressed patients (≥60 years of age) who received 20 mg fluoxetine for 6 weeks. Combined fluoxetine plus norfluoxetine plasma concentrations were 209.3 ± 85.7 ng/mL at the end of 6 weeks. No unusual age-associated pattern of adverse reactions was observed in those elderly patients.
The pharmacokinetics of SYMBYAX has not been studied in patients with renal impairment. However, olanzapine and fluoxetine individual pharmacokinetics do not differ significantly in patients with renal impairment. SYMBYAX dosing adjustment based upon renal impairment is not routinely required.
Because olanzapine is highly metabolized before excretion and only 7% of the drug is excreted unchanged, renal dysfunction alone is unlikely to have a major impact on the pharmacokinetics of olanzapine. The pharmacokinetic characteristics of olanzapine were similar in patients with severe renal impairment and normal subjects, indicating that dosage adjustment based upon the degree of renal impairment is not required. In addition, olanzapine is not removed by dialysis. The effect of renal impairment on olanzapine metabolite elimination has not been studied.
In depressed patients on dialysis (N=12), fluoxetine administered as 20 mg once daily for 2 months produced steady-state fluoxetine and norfluoxetine plasma concentrations comparable with those seen in patients with normal renal function. While the possibility exists that renally excreted metabolites of fluoxetine may accumulate to higher levels in patients with severe renal dysfunction, use of a lower or less frequent dose is not routinely necessary in renally impaired patients.
Based on the individual pharmacokinetic profiles of olanzapine and fluoxetine, the pharmacokinetics of SYMBYAX may be altered in patients with hepatic impairment. The lowest starting dose should be considered for patients with hepatic impairment [see Dosage and Administration (2.3) and Warnings and Precautions (5.20)].
Although the presence of hepatic impairment may be expected to reduce the clearance of olanzapine, a study of the effect of impaired liver function in subjects (N=6) with clinically significant cirrhosis (Child-Pugh Classification A and B) revealed little effect on the pharmacokinetics of olanzapine.
As might be predicted from its primary site of metabolism, liver impairment can affect the elimination of fluoxetine. The elimination half-life of fluoxetine was prolonged in a study of cirrhotic patients, with a mean of 7.6 days compared with the range of 2 to 3 days seen in subjects without liver disease; norfluoxetine elimination was also delayed, with a mean duration of 12 days for cirrhotic patients compared with the range of 7 to 9 days in normal subjects.
Clearance of olanzapine is approximately 30% lower in women than in men. There were, however, no apparent differences between men and women in effectiveness or adverse effects. Dosage modifications based on gender should not be needed.
Olanzapine clearance is about 40% higher in smokers than in nonsmokers, although dosage modifications are not routinely required.
No SYMBYAX pharmacokinetic study was conducted to investigate the effects of race. In vivo studies have shown that exposures to olanzapine are similar among Japanese, Chinese and Caucasians, especially after normalization for body weight differences. Dosage modifications for race, therefore, are not routinely required.
The combined effects of age, smoking, and gender could lead to substantial pharmacokinetic differences in populations. The clearance of olanzapine in young smoking males, for example, may be 3 times higher than that in elderly nonsmoking females. SYMBYAX dosing modification may be necessary in patients who exhibit a combination of factors that may result in slower metabolism of the olanzapine component [see Dosage and Administration (2.3)].
Based on the pediatric SYMBYAX study, steady-state olanzapine, fluoxetine, and norfluoxetine plasma concentrations were about 31%, 76%, and 38% higher, respectively, in pediatric patients with lower body weights (less than 50 kg) than in pediatric patients with high body weight (greater than or equal to 50 kg). Exposures in pediatric patients with high body weight were similar to those previously observed in adults. Dose modifications based on body weight are not required.
No carcinogenicity, mutagenicity, or fertility studies were conducted with SYMBYAX. The following data are based on findings in studies performed with the individual components, and all dose multiples (based on body surface area) reflect the maximum recommended human dose (MRHD) of 12 mg olanzapine, or 50 mg fluoxetine in SYMBYAX.
Oral carcinogenicity studies were conducted in mice and rats. Olanzapine was administered to mice in two 78-week studies at doses of 3, 10, and 30/20 mg/kg/day [equivalent to 1 to 12 times the MRHD based on mg/m² body surface area] and 0.25, 2, and 8 mg/kg/day (equivalent to up to 3 times the oral MRHD based on mg/m² body surface area). Rats were dosed for 2 years at doses of 0.25, 1, 2.5 and 4 mg/kg/day (males) and 0.25, 1, 4 and 8 mg/kg/day (females) (equivalent to up to 3 and 7 times the oral MRHD based on mg/m² body surface area, respectively). The incidence of liver hemangiomas and hemangiosarcomas was significantly increased in 1 mouse study in female mice at 3 times the daily oral MRHD based on mg/m² body surface area). These tumors were not increased in another mouse study in females dosed at (up to 12 times the daily oral MRHD based on mg/m² body surface area); in this study, there was a high incidence of early mortalities in males of the 30/20 mg/kg/day group. The incidence of mammary gland adenomas and adenocarcinomas was significantly increased in female mice dosed at ≥2 mg/kg/day and in female rats dosed at ≥4 mg/kg/day (1 and 3 times the oral MRHD based on mg/m² body surface area, respectively). Antipsychotic drugs have been shown to chronically elevate prolactin levels in rodents. Serum prolactin levels were not measured during the olanzapine carcinogenicity studies; however, measurements during subchronic toxicity studies showed that olanzapine elevated serum prolactin levels up to 4-fold in rats at the same doses used in the carcinogenicity study. An increase in mammary gland neoplasms has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be prolactin-mediated. The relevance for human risk of the finding of prolactin-mediated endocrine tumors in rodents is unknown [see Warnings and Precautions (5.22)].
The dietary administration of fluoxetine to rats and mice for 2 years at doses of up to 10 and 12 mg/kg/day, respectively (approximately 2 and 1 times, respectively, the MRHD of 20 mg given to children based on mg/m² body surface area), produced no evidence of carcinogenicity.
No evidence of genotoxic potential for olanzapine was found in the following tests: Ames reverse mutation test, in vivo micronucleus test in mice, the chromosomal aberration test in Chinese hamster ovary cells, unscheduled DNA synthesis test in rat hepatocytes, induction of forward mutation test in mouse lymphoma cells, or in vivo sister chromatid exchange test in bone marrow of Chinese hamsters.
No evidence of genotoxic potential for fluoxetine and norfluoxetine was found in the following tests: bacterial mutation assay, DNA repair assay in cultured rat hepatocytes, mouse lymphoma assay, and in vivo sister chromatid exchange assay in Chinese hamster bone marrow cells.
Fertility studies were not conducted with SYMBYAX. However, in a repeat-dose rat toxicology study of 3 months duration, ovary weight was decreased in females treated with the low-dose [2 and 4 mg/kg/day (approximately 2 and 1 times the MRHD of 12 mg (olanzapine) and 50 mg (fluoxetine) based on mg/m² body surface area), respectively] and high-dose [4 and 8 mg/kg/day (3 and 2 times the MRHD based on mg/m² body surface area), respectively] combinations of olanzapine and fluoxetine. Decreased ovary weight, and corpora luteal depletion and uterine atrophy were observed to a greater extent in the females receiving the high-dose combination than in females receiving either olanzapine or fluoxetine alone. In a 3-month repeat-dose dog toxicology study, reduced epididymal sperm and reduced testicular and prostate weights were observed with the high-dose combination of olanzapine and fluoxetine [5 and 5 mg/kg/day (14 and 3 times the MRHD based on mg/m² body surface area), respectively] and with olanzapine alone (5 mg/kg/day or 14 times the MRHD based on mg/m² body surface area).
In an oral fertility and reproductive performance study in rats, male mating performance, but not fertility, was impaired at a dose of 22.4 mg/kg/day and female fertility was decreased at a dose of 3 mg/kg/day (18 and 2 times the daily oral MRHD of 12 mg given to adults based on mg/m² body surface area, respectively). Discontinuance of olanzapine treatment reversed the effects on male-mating performance. In female rats, the precoital period was increased and the mating index reduced at 5 mg/kg/day (4 times the MRHD based on mg/m² body surface area). Diestrous was prolonged and estrous was delayed at 1.1 mg/kg/day (1 times the daily oral MRHD based on mg/m² body surface area); therefore, olanzapine may produce a delay in ovulation.
Two fertility studies conducted in adult rats at doses of up to 7.5 and 12.5 mg/kg/day (approximately 1 and 2 times the MRHD of 50 mg given to adolescents based on mg/m² body surface area) indicated that fluoxetine had no adverse effects on fertility. However, adverse effects on fertility were seen when juvenile rats were treated with fluoxetine [see Use in Specific Populations (8.4)].
Efficacy for SYMBYAX was established for the:
Adults: The efficacy of SYMBYAX for the acute treatment of depressive episodes associated with Bipolar I Disorder was established in 2 identically designed, 8-week, randomized, double-blind, controlled studies of patients who met Diagnostic and Statistical Manual 4th edition (DSM-IV) criteria for Bipolar I Disorder, Depressed utilizing flexible dosing of SYMBYAX (6/25, 6/50, or 12/50 mg/day), olanzapine (5 to 20 mg/day), and placebo. These studies included patients (≥18 years of age [n=788]) with or without psychotic symptoms and with or without a rapid cycling course.
The primary rating instrument used to assess depressive symptoms in these studies was the Montgomery-Asberg Depression Rating Scale (MADRS), a 10-item clinician-rated scale with total scores ranging from 0 to 60. The primary outcome measure of these studies was the change from baseline to endpoint in the MADRS total score. In both studies, SYMBYAX was statistically significantly superior to both olanzapine monotherapy and placebo in reduction of the MADRS total score. Refer to Table 18 (Studies 1 and 2).
Children and Adolescents: The efficacy of SYMBYAX for the acute treatment of depressive episodes associated with Bipolar I Disorder was established in a single 8-week, randomized, double-blind, placebo-controlled study of patients, 10 to 17 years of age [N=255], who met Diagnostic and Statistical Manual 4th edition-Text Revision (DSM-IV-TR) criteria for Bipolar I Disorder, Depressed. Patients were initiated at a dose of 3/25 mg/day and force-titrated to the maximum dose of 12/50 mg/day over two weeks. After Week 2, there was flexible dosing of SYMBYAX in the range of 6/25, 6/50, 12/25, or 12/50 mg/day. The average daily dose was olanzapine 7.7 mg and fluoxetine 37.6 mg. The recommended starting dose for children and adolescents is 3/25 mg per day. Flexible dosing is recommended, rather than the forced titration used in the study [see Dosage and Administration (2.1)]. This study included patients with or without psychotic symptoms.
The primary rating instrument used to assess depressive symptoms in these studies was the Children’s Depressive Rating Scale-Revised (CDRS-R), a 17-item clinician-rated scale with total scores ranging from 17 to 113. The primary outcome measure of this study was the change from baseline to Week 8 in the CDRS-R total score. In this study, SYMBYAX was statistically significantly superior to placebo in reduction of the CDRS-R total score. Refer to Table 18 (Study 3).
Table 18. Summary of the Primary Efficacy Result for Studies in Bipolar Depressiona:
| Study Number (Primary Efficacy Measure) | Treatment group | Mean baseline score (SD) | LS mean change from baseline (SE) | Differenceb from SYMBYAX (95% CI) |
|---|---|---|---|---|
| Study 1 (MADRS) | SYMBYAX Olanzapine Placebo | 29.9 (5.0) 32.4 (6.3) 31.2 (5.7) | -18.7 (1.8) -14.4 (1.0) -13.3 (1.0) | -4.4 (NA) -5.5 (NA) |
| Study 2 (MADRS) | SYMBYAX Olanzapine Placebo | 31.7 (6.8) 32.8 (6.1) 31.4 (6.6) | -18.44 (1.7) -15.81 (1.0) -10.68 (1.0) | -2.6 (NA) -7.8 (NA) |
| Study 3 (CDRS-R) | SYMBYAX Placebo | 54.6 (10.0) 53.7 (8.2) | -28.43 (1.1) -23.40 (1.5) | -5.0 (-8.3, -1.8) |
a SD – standard deviation; SE – standard error; LS mean – least-squares mean estimate; CI – unadjusted confidence interval; NA – not available.
b Difference (SYMBYAX minus active comparator or placebo) in least squares estimates.
The efficacy of SYMBYAX in acute treatment resistant depression was demonstrated with data from 3 clinical studies (n=579) in adults (18 to 85 years). Doses evaluated in these studies ranged from 6 to 18 mg for olanzapine and 25 to 50 mg for fluoxetine.
An 8-week randomized, double-blind controlled study was conducted to evaluate the efficacy of SYMBYAX in patients (n=300) who met DSM-IV criteria for Major Depressive Disorder and did not respond to 2 different antidepressants after at least 6 weeks at or above the minimally effective labeled dosage in their current episode. Patients who were not responding to an antidepressant in their current episode entered an 8-week open-label fluoxetine lead-in; non-responders were randomized (1:1:1) to receive SYMBYAX, olanzapine, or fluoxetine, and were treated for 8 weeks. SYMBYAX was flexibly dosed between 6/50 mg, 12/50 mg, and 18/50 mg. Results from this study yielded statistically significant greater reduction in mean total MADRS scores from baseline to endpoint for SYMBYAX versus fluoxetine and olanzapine. See Table 19 (Study 4). A second study with the same treatment-resistant patient population (n=28), when analyzed with change in MADRS as the outcome measure, demonstrated statistically significantly greater reduction in MADRS scores for SYMBYAX versus fluoxetine and olanzapine. See Table 19 (Study 5). A third study demonstrated statistically significantly greater reduction in total MADRS scores for SYMBYAX versus fluoxetine or olanzapine alone, when analyzed in a subpopulation of depressed patients (n=251) who met the definition of treatment resistance (patients who had not responded to 2 antidepressants of adequate dose and duration in the current episode). See Table 19 (Study 6).
Table 19. Summary of the Primary Efficacy Result for Studies in Treatment-Resistant Depressiona:
| Study Number (Primary Efficacy Measure) | Treatment group | Mean baseline score (SD) | LS Mean change from baseline (SE) | Differenceb from SYMBYAX (95% CI) |
|---|---|---|---|---|
| Study 4 (MADRS) | SYMBYAX Olanzapine Fluoxetine | 30.6 (6.1) 30.1 (6.3) 30.1 (5.9) | -14.1 (1.0) -7.1 (1.0) -8.3 (1.1) | -6.9 (NA) -5.8 (NA) |
| Study 5 (HAMD-21) | SYMBYAX Olanzapine Fluoxetine | 26.4 (7.5) 24.5 (5.2) 23.5 (6.0) | -11.7 (3.3) -5.9 (1.9) -3.8 (3.0) | -6.1 (-13.7, 1.5) -6.7 (-14.0, 0.5) |
| Study 6 (MADRS) | SYMBYAX Olanzapine Fluoxetine | 30.1 (6.6) 31.5 (6.8) 31.1 (5.6) | -13.3 (0.8) -8.8 (1.7) -10.0 (1.4) | NA NA |
a SD – standard deviation; SE – standard error; LS mean – least-squares mean estimate; CI – unadjusted confidence interval; NA – not available.
b Difference (SYMBYAX minus active comparator or placebo) in least squares estimates.
The efficacy of SYMBYAX in the maintenance therapy of treatment-resistant depression was demonstrated in a 47-week study (Study 7) in adults (18 to 65 years). SYMBYAX was dosed between 6/25 mg, 12/25 mg, 6/50 mg, 12/50 mg, and 18/50 mg.
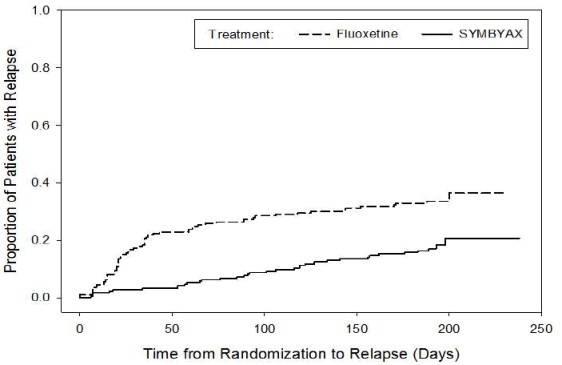
Patients (N=892) met DSM-IV criteria for Major Depressive Disorder and for treatment-resistant depression (a lack of response to 2 antidepressants after at least 6 weeks at or above the minimally effective labeled dose in their current episode of major depressive disorder). Patients were initially treated with open-label SYMBYAX; those who responded to and were stabilized on treatment over approximately 20 weeks were randomized to continue receiving treatment with SYMBYAX (n=221) or to receive treatment with fluoxetine (n=223) for another 27 weeks. Relapse was assessed using 3 criteria: a 50% increase in Montgomery-Åsberg Depression Rating Scale score from randomization with concomitant Clinical Global Impressions–Severity of Depression score increase to 4 or more; hospitalization due to depression or suicidality; or discontinuation due to lack of efficacy/worsening of depression/suicidality. A total of 15.8% of patients on SYMBYAX and 31.8% of patients on fluoxetine relapsed; this difference was statistically significant. Patients receiving continued SYMBYAX experienced statistically significantly longer time to relapse over the 27 weeks compared with those receiving fluoxetine (Figure 1).
Figure 1. Kaplan-Meier Estimation of Cumulative Proportion of Patients with Relapse (Study 7):
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.