TEGSEDI Solution for injection Ref.[116635] Active ingredients: Inotersen
Source: European Medicines Agency (EU) Revision Year: 2026 Publisher: Akcea Therapeutics Ireland Ltd, St. James House, 72 Adelaide Road, Dublin 2, D02 Y017, Ireland
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Other Nervous System Drugs
ATC code: N07XX15
Mechanism of action
Inotersen is a 2′-O-2-methoxyethyl (2′-MOE) phosphorothioate antisense oligonucleotide (ASO) inhibitor of human transthyretin (TTR) production. The selective binding of inotersen to the TTR messenger RNA (mRNA) causes the degradation of both mutant and wild type (normal) TTR mRNA. This prevents the synthesis of TTR protein in the liver, resulting in significant reductions in the levels of mutated and wild type TTR protein secreted by the liver into the circulation.
TTR is a carrier protein for retinol binding protein 4 (RBP4) which is the principal carrier of vitamin A (retinol). Therefore, reduction in plasma TTR is expected to result in reduction of plasma retinol levels to below the lower limit of normal.
Pharmacodynamic effects
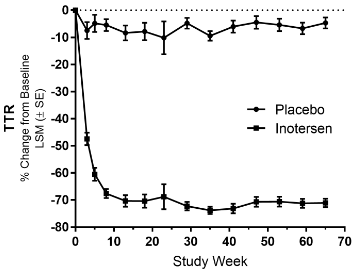
In the pivotal study, a phase ⅔ randomized, double-blind, placebo-controlled study to assess the efficacy and safety of ISIS 420915 in patients with Familial Amyloid Polyneuropathy (NEURO-TTR Study), in the inotersen treatment group, robust reduction in circulating TTR levels was observed throughout the 15-month treatment period, with mean percent changes from baseline in serum TTR ranging from 68.41% to 74.03% (median range: 74.64% to 78.98%) from Week 13 to Week 65 (Figure 1). In the placebo group, mean serum TTR concentration decreased by 8.50% at Week 3 and then remained fairly constant throughout the treatment period.
Figure 1. Percent change from baseline in serum TTR over time:
Transthyretin (TTR)
Least Squares Mean (LSM)
Standard Error (SE)
Clinical efficacy and safety
The NEURO-TTR multicentre, double-blind, placebo-controlled trial was comprised of 172 treated patients with hereditary transthyretin amyloidosis with polyneuropathy (hATTR-PN). The disease hATTR-PN is classified into 3 stages such that i) Stage 1 patients do not require assistance with ambulation, ii) Stage 2 patients do require assistance with ambulation, and iii) Stage 3 patients are bound to wheelchair. Subjects with Stage 1 and Stage 2 hATTR-PN and a Neuropathy Impairment Score (NIS) ≥ 10 and ≤ 130 were recruited in the pivotal NEURO-TTR study. The study evaluated 284 mg inotersen administered as one subcutaneous injection once per week, for 65 weeks of treatment. Patients were randomised 2:1 to receive either inotersen or placebo. The primary efficacy endpoints were the change from baseline to Week 66 in the modified Neuropathy Impairment Score + 7 tests (mNIS+7) composite score and in the Norfolk Quality of Life – Diabetic Neuropathy (QoL-DN) questionnaire total score. Patients were stratified for stage of disease (Stage 1 versus Stage 2), TTR mutation (V30M versus non-V30M) and previous treatment with either tafamidis or diflunisal (yes versus no). Baseline demographic and disease characteristics are shown in Table 3.
Table 3. Baseline demographics:
| Placebo (N=60) | Inotersen (N=112) | |
| Age (years), mean (SD) | 59,5 (14,05) | 59,0 (12,53) |
| Age 65 years and older, n (%) | 26 (43,3) | 48 (42,9) |
| Male, n (%) | 41 (68,3) | 77 (68,8) |
| mNIS+7, mean (SD) | 74,75 (39,003) | 79,16 (36,958) |
| Norfolk QoL-DN, mean (SD) | 48,68 (26,746) | 48,22 (27,503) |
| Disease stage, n (%) | ||
| Stage 1 | 42 (70,0) | 74 (66,1) |
| Stage 2 | 18 (30,0) | 38 (33,9) |
| V30M TTR mutation1, n (%) | ||
| Yes | 33 (55,0) | 56 (50,0) |
| No | 27 (45,0) | 56 (50,0) |
| Previous treatment with tafamidis or diflunisal1, n (%) | ||
| Yes | 36 (60,0) | 63 (56,3) |
| No | 24 (40,0) | 49 (43,8) |
| hATTR-CM2, n (%) | 33 (55,0) | 75 (66,4) |
| hATTR-PN Disease Duration3 (months) mean (SD) | 64,0 (52,34) | 63,9 (53,16) |
| hATTR-CM Disease Duration3 (months) mean (SD) | 34,1 (29,33) | 44,7 (58,00) |
1 Based on clinical database.
2 Defined as all patients with a diagnosis of hereditary transthyretin amyloidosis with cardiomyopathy (hATTR-CM) at study entry or left ventricular wall thickness >1.3 cm on echocardiogram without a known history of persistent hypertension.
3 Duration from symptom onset to informed consent date.
modified Neuropathy Impairment Score (mNIS)
Quality of Life-Diabetic Neuropathy (QoL-DN)
hereditary transthyretin amyloidosis-polyneuropathy (hATTR-PN)
Standard deviation (SD)
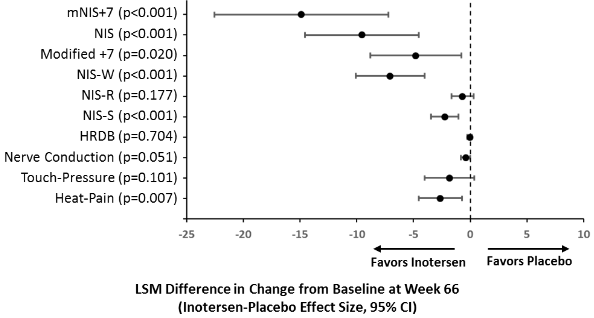
The changes from baseline in both primary endpoints (mNIS+7 and Norfolk QoL-DN) demonstrated statistically significant benefit in favour of inotersen treatment at Week 66 (Table 4). Results across multiple disease characteristics [TTR mutation (V30M, non-V30M)], disease stage (Stage 1, Stage 2), previous treatment with tafamidis or diflunisal (yes, no), presence of hATTR-CM (yes, no) at Week 66 showed statistically significant benefit in all subgroups based on mNIS+7 composite score and all but one of these subgroups (CM-Echo Set; p=0.067) based on Norfolk QoL-DN total score (Table 5). Furthermore, results across the components of mNIS+7 and domains of Norfolk QoL-DN composite scores were consistent with the primary endpoint analysis, showing benefit in motor, sensory and autonomic neuropathies (Figure 2).
Table 4. Primary endpoint analysis mNIS+7 and Norfolk QoL-DN:
| mNIS+7 | Norfolk-QOL-DN | |||
| Placebo (N=60) | Inotersen (N=112) | Placebo (N=60) | Inotersen (N=112) | |
| Baseline | ||||
| n | 60 | 112 | 59 | 111 |
| Mean (SD) | 74,75 (39,003) | 79,165 (36,958) | 48,68 (26,746) | 48,22 (27,503) |
| Week 66 Change | ||||
| n | 60 | 112 | 59 | 111 |
| LSM (SE) | 25,43 (3,225) | 10,54 (2,397) | 12,94 (2,840) | 4,38 (2,175) |
| 95% CI | 19,11, 31,75 | 15,85, 15,24 | 7,38, 18,51 | 0,11, 8,64 |
| Difference in LSM (Tegsedi – Placebo) | -14,89 | -8,56 | ||
| 95% CI | -22,55; -7,22 | -15,42; -1,71 | ||
| P-value | <0,001 | 0,015 | ||
Quality of Life-Diabetic Neuropathy (QoL-DN)
Standard deviation (SD)
Least squares mean (LSM)
Table 5. Subgroup analysis of mNIS+7 and Norfolk QoL-DN:
| mNIS+7 | Norfolk QOL-DN | |||||
| Change from Baseline Inotersen – Placebo | Change from Baseline Inotersen – Placebo | |||||
| Subgroup | N (Placebo, Inotersen) | LSM Difference (SE) | P-value | n (Placebo, Inotersen) | LSM Difference (SE) | P-value |
| Week 66 | ||||||
| V30M | 32, 58 | -13,52 (3,795) | p<0,001 | 32, 58 | -8,14 (3,998) | p=0,042 |
| Non-V30 | 28, 54 | -19,06 (5,334) | p<0,001 | 27, 53 | -9,87 (4,666) | p=0,034 |
| Stage I Disease | 39, 74 | -12,13 (3,838) | p=0,002 | 38, 73 | -8,44 (3,706) | p=0,023 |
| Stage II Disease | 21, 38 | -24,79 (5,601) | p<0,001 | 21, 38 | -11,23 (5,271) | p=0,033 |
| Previous use of stabilisers | 33, 61 | -18,04 (4,591) | p<0,001 | 32, 60 | -9,26 (4,060) | p=0,022 |
| Treatment naïve | 27, 51 | -14,87 (4,377) | p<0,001 | 27, 51 | -10,21 (4,659) | p=0,028 |
| CM-Echo Set | 33, 75 | -14,94 (4,083) | p<0,001 | 33, 75 | -7,47 (4,075) | p=0,067 |
| Non-CM- Echo Set | 27, 37 | -18,79 (5,197) | p<0,001 | 26, 36 | -11,67 (4,213) | p=0,006 |
Figure 2. Difference in least squares mean (LSM) change from baseline between treatment groups in mNIS+7 and components:
Least squares mean (LSM)
Quality of Life-Diabetic Neuropathy (QoL-DN)
modified Neuropathy Impairment Score (mNIS)
NIS-W – sub-score for weakness
NIS-R – sub-score for muscle stretch reflexes
NIS-S – sub-score for clinical sensation
Heart Rate during Deep Breathing (HRDB)
A responder analysis of mNIS+7 using thresholds ranging from a 0-point to 30-point increase from baseline (using the safety set), showed the inotersen group had approximately a 2-fold higher response rate than the placebo group at each threshold tested, demonstrating consistency of response. A responder was defined as a subject who had a change from baseline that was less than or equal to the threshold value. Subjects that terminate the treatment early irrespective of the reason or have missing week 66 data are considered as non-responders. Statistical significance in favour of inotersen was demonstrated at all thresholds beyond a 0-point change.
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with Tegsedi in all subsets of the paediatric population in transthyretin amyloidosis (see section 4.2 for information on paediatric use).
5.2. Pharmacokinetic properties
Absorption
Following subcutaneous administration, inotersen is absorbed rapidly into systemic circulation in a dose-dependent fashion with the median time to maximum plasma concentrations (Cmax) of inotersen typically reached within 2 to 4 hours.
Distribution
Inotersen is highly bound to human plasma protein (>94%) and the fraction bound is independent of concentration. The apparent volume of distribution of inotersen at steady-state is 293 L in patients with hATTR. The high volume of distribution suggests inotersen extensively distributes into tissues following subcutaneous administration.
Biotransformation
Inotersen is not a substrate for CYP450 metabolism and is metabolised in tissues by endonucleases to form shorter inactive oligonucleotides that are the substrates for additional metabolism by exonucleases. Unchanged inotersen is the predominant circulating component.
Elimination
The elimination of inotersen involves both metabolism in tissues and excretion in urine. Both inotersen and its shorter oligonucleotide metabolites are excreted in human urine. Urinary recovery of the parent active substance is limited to less than 1% within the 24 hours post dose. Following subcutaneous administration, elimination half-life for inotersen is approximately 1 month.
Special populations
Based on the population pharmacokinetic analysis, age, body weight, sex or race has no clinically relevant effect on inotersen exposure. Definitive assessments were limited in some cases as covariates were limited by the overall low numbers.
Elderly population
No overall differences in pharmacokinetics were observed between other adult and elderly patients.
Renal impairment
A population pharmacokinetic analysis suggests that mild and moderate renal impairment has no clinically relevant effect on the systemic exposure of inotersen. No data are available in patients with severe renal impairment.
Hepatic impairment
The pharmacokinetics of inotersen in patients with hepatic impairment has not been studied. Inotersen is not primarily cleared by metabolism in the liver, not a substrate for CYP450 oxidation, and metabolized broadly by nucleases in all tissues of distribution. Thus, pharmacokinetics should not be altered in mild to moderate hepatic impairment.
5.3. Preclinical safety data
Toxicology
Decreased platelet counts were observed in chronic toxicity studies in mice, rats and monkeys at 1.4 to 2-fold the human AUC at the recommended therapeutic inotersen dose. Severe platelet declines in association with increased bleeding or bruising were observed in individual monkeys. Platelet counts returned to normal when treatment was stopped but dropped to even lower levels when inotersen administration was resumed. This suggests an immunologically related mechanism.
Extensive and persistent uptake of inotersen was observed by various cell types in multiple organs of all tested animal species including monocytes/macrophages, kidney proximal tubular epithelia, Kupffer cells of the liver, and histiocytic cell infiltrates in lymph nodes and injection sites. The kidney accumulation of inotersen was associated with proteinuria in rats at 13.4-fold the human AUC at the recommended therapeutic inotersen dose. In addition, reduced thymus weight due to lymphocyte depletion was observed in mice and rats. In monkeys, perivascular cell infiltration by lymphohistiocytic cells in multiple organs was noted. These pro-inflammatory organ changes were observed at 1.4 to 6.6-fold the human AUC at the recommended therapeutic dose in all animal species tested and were accompanied by increases of various plasma cytokines/chemokines.
Genotoxicity/carcinogenicity
Inotersen did not exhibit genotoxic potential in in vitro and in vivo and was not carcinogenic in transgenic rasH2 mice.
Subcutaneous administration of inotersen to Sprague-Dawley rats for up to 94 weeks at doses of 0.5, 2, and 6 mg/kg/week resulted in a dose-related incidence of subcutaneous pleomorphic fibrosarcoma and subcutaneous fibrosarcoma (monomorphic type) at 2 and 6 mg/kg/week in the injection site or injection site regions. The human relevance of these findings is considered to be low.
Reproductive toxicology
Inotersen showed no effects on fertility, embryo-foetal, or postnatal development in mice and rabbits at approximately 3-fold the maximum recommended human equivalent dose. Milk transfer of inotersen was low in mice. However, inotersen is not pharmacologically active in mice and rabbits. Consequently, only effects related to the chemistry of inotersen could be captured in these investigations. Still, no effect on embryo-foetal development was noted with a mouse-specific analogue of inotersen in mice, which was associated with ~60% inhibition (individual range up to 90% reduction) of TTR mRNA expression.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.