TEZSPIRE Solution for injection Ref.[50203] Active ingredients: Tezepelumab
Source: European Medicines Agency (EU) Revision Year: 2025 Publisher: AstraZeneca AB, SE-151 85 Södertälje, Sweden
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Drugs for obstructive airway diseases, other systemic drugs for obstructive airway diseases
ATC code: R03DX11
Mechanism of action
Tezepelumab is a monoclonal antibody (IgG2λ) directed against thymic stromal lymphopoietin (TSLP), preventing its interaction with the heterodimeric TSLP receptor. In asthma and CRSwNP, both allergic and non-allergic triggers induce TSLP production. Blocking TSLP with tezepelumab reduces a broad spectrum of biomarkers and cytokines associated with airway and mucosal inflammation in asthma and CRSwNP (e.g. blood eosinophils, airway submucosal eosinophils, IgE, FeNO, IL-5, and IL-13); however, the mechanism of action of tezepelumab in asthma and CRSwNP has not been definitively established.
Pharmacodynamic effects
Effect on blood eosinophils and inflammatory biomarkers and cytokines
In clinical trials, administration of tezepelumab 210 mg subcutaneously every 4 weeks reduced blood eosinophils counts, FeNO, IL-5 concentration, IL-13 concentration and serum IgE concentration from baseline compared with placebo. These markers were near maximal suppression after 2 weeks of treatment, except for IgE which declined more slowly. These effects were sustained throughout treatment.
In a CRSwNP clinical trial, administration of tezepelumab 210 mg subcutaneously every 4 weeks resulted in reductions of inflammatory biomarkers (blood eosinophils, FeNO [in participants with co-morbid asthma] and serum IgE).
Effect on eosinophils in the airway submucosa
In a clinical trial, administration of tezepelumab 210 mg subcutaneously every 4 weeks reduced submucosal eosinophil counts by 89% compared with a 25% reduction with placebo. Reduction was consistent regardless of baseline inflammatory biomarkers.
Immunogenicity
In patients with asthma (NAVIGATOR), anti-drug antibodies (ADA) were detected at any time in 26 (4.9%) out of 527 patients who received tezepelumab at the recommended dosing regimen during the 52-week study period. Of these 26 patients, 10 patients (1.9% of patients treated with tezepelumab) developed treatment-emergent ADA and 1 patient (0.2% of patients treated with tezepelumab) developed neutralising antibodies. ADA titres were generally low and often transient. No evidence of ADA impact on pharmacokinetics, pharmacodynamics, efficacy, or safety was observed.
In patients with CRSwNP (WAYPOINT), a treatment-emergent ADA response developed in 6 (4%) out of 164 patients treated with tezepelumab 210 mg subcutaneously every 4 weeks during the 52-week treatment period. Neutralising antibody activity was detected in 1 of the ADA positive patients. While there was no apparent impact of ADA on pharmacokinetics, pharmacodynamics, efficacy, or safety, there were insufficient numbers of patients with treatment-emergent ADA to make a formal assessment in CRSwNP.
Clinical efficacy
Asthma
The efficacy of tezepelumab was evaluated in two randomised, double-blind, parallel group, placebo-controlled clinical trials (PATHWAY and NAVIGATOR) of 52 weeks in duration involving a total of 1609 patients aged 12 years and older with severe asthma. In both trials, patients were enrolled without requiring a minimum baseline level of blood eosinophils or other inflammatory biomarkers (e.g. FeNO or IgE).
PATHWAY was a 52-week exacerbation trial which enrolled 550 patients (18 years of age and older) with severe, uncontrolled asthma to receive treatment with tezepelumab 70 mg subcutaneous Q4W, tezepelumab 210 mg subcutaneous Q4W, tezepelumab 280 mg subcutaneous Q2W or placebo. Patients were required to have a history of 2 or more asthma exacerbations requiring oral or systemic corticosteroid treatment or 1 asthma exacerbation resulting in hospitalisation in the past 12 months.
NAVIGATOR was a 52-week exacerbation trial which enrolled a total of 1061 patients (adults and adolescents 12 years of age and older) with severe, uncontrolled asthma to receive treatment with tezepelumab 210 mg subcutaneous Q4W or placebo. Patients were required to have a history of 2 or more asthma exacerbations requiring oral or systemic corticosteroid treatment or resulting in hospitalisation in the past 12 months.
In both PATHWAY and NAVIGATOR, patients were required to have an Asthma Control Questionnaire 6 (ACQ-6) score of 1.5 or more at screening, and reduced lung function at baseline (pre-bronchodilator FEV1 below 80% predicted in adults, and below 90% predicted in adolescents). Patients were required to have been on regular treatment with medium- or high-dose inhaled corticosteroids (ICS) and at least one additional asthma control therapy with or without oral corticosteroids (OCS). High ICS dose was defined as >500 mcg fluticasone propionate or equivalent per day. Medium ICS dose was defined as >250 to 500 mcg fluticasone propionate or equivalent per day in PATHWAY and as 500 mcg fluticasone propionate or equivalent per day in NAVIGATOR. Patients continued background asthma therapy throughout the duration of the trials.
The demographics and baseline characteristics of these two trials are provided in Table 2 below.
Table 2. Demographics and baseline characteristics of asthma trials:
| PATHWAY N=550 | NAVIGATOR N=1059 | |
|---|---|---|
| Mean age (year) (SD) | 52 (12) | 50 (16) |
| Female (%) | 66 | 64 |
| White (%) | 92 | 62 |
| Black or African American (%) | 3 | 6 |
| Asian (%) | 3 | 28 |
| Hispanic or Latino (%) | 1 | 15 |
| Mean duration of asthma, (years) (SD) | 17 (12) | 22 (16) |
| Never smoked (%) | 81 | 80 |
| High-dose ICS use (%) | 49 | 75 |
| OCS use (%) | 9 | 9 |
| Mean number of exacerbations in previous year (SD) | 2.4 (1.2) | 2.8 (1.4) |
| Mean baseline % predicted FEV1 (SD) | 60 (13) | 63 (18) |
| Mean pre-bronchodilator FEV1 (L) (SD) | 1.9 (0.6) | 1.8 (0.7) |
| Mean post-bronchodilator FEV1 reversibility (%) (SD) | 23 (20) | 15 (15) |
| Mean baseline blood EOS count (cells/µL) (SD) | 371 (353) | 340 (403) |
| Blood EOS count ≥150 cells/µL (%) | 76 | 74 |
| Positive allergic status (%)a | 46 | 64 |
| Mean FeNO (ppb) (SD) | 35 (39) | 44 (41) |
| FeNO ≥25 ppb (%) | 44 | 59 |
| Mean ACQ-6 (SD) | 2.7 (0.8) | 2.8 (0.8) |
| Blood EOS count ≥150 cells/µL and FeNO ≥25 ppb (%) | 38 | 47 |
a Positive allergic status as defined by a positive serum IgE result specific to any perennial aeroallergen in the FEIA panel.
ACQ-6, Asthma Control Questionnaire 6; EOS, Eosinophils; FEIA, Fluorescent enzyme immunoassay; FeNO, Fractional exhaled nitric oxide; FEV1, Forced expiratory volume in one second; ICS, Inhaled corticosteroid; IgE, Immunoglobulin E; OCS, Oral corticosteroid; ppb, Parts per billion; SD, Standard deviation.
The results summarised below are for the recommended tezepelumab 210 mg subcutaneous Q4W dosing regimen.
Exacerbations
The primary endpoint for PATHWAY and NAVIGATOR was the rate of severe asthma exacerbations measured over 52 weeks. Severe asthma exacerbations were defined as worsening of asthma requiring the use of or increase in oral or systemic corticosteroids for at least 3 days or a single depo-injection of corticosteroids, and/or emergency department visits requiring use of oral or systemic corticosteroids and/or hospitalisation.
In both PATHWAY and NAVIGATOR, patients receiving tezepelumab had significant reductions in the annualised rate of severe asthma exacerbations compared with placebo (Table 3 and Table 4). There were also fewer exacerbations requiring emergency room visits and/or hospitalisation in patients treated with tezepelumab compared with placebo. In PATHWAY and NAVIGATOR, severe asthma exacerbations requiring emergency room visits and/or hospitalisation were reduced by 85% and 79% with tezepelumab 210 mg subcutaneous Q4W, respectively.
Table 3. Rate of severe exacerbations at week 52 in NAVIGATORa:
| Tezepelumab (N=528) | Placebo (N=531) | |
|---|---|---|
| Annualised severe asthma exacerbation rate | ||
| Rate | 0.93 | 2.10 |
| Rate ratio (95% CI) | 0.44 (0.37, 0.53) | |
| p-value | <0.001 | |
a Time at risk is defined as the total duration of time in which a new exacerbation can occur (i.e. total follow-up time minus time during exacerbation and 7 days after).
CI, Confidence interval
Table 4. Rate of severe exacerbations at week 52 in PATHWAYa:
| Tezepelumab (N=137) | Placebo (N=138) | |
|---|---|---|
| Annualised severe asthma exacerbation rate | ||
| Rate | 0.20 | 0.72 |
| Rate ratio (95% CI) | 0.29 (0.16, 0.51) | |
|p-value|\2<> <0.001
a Time at risk is defined as the total follow-up time.
CI, Confidence interval
Subgroup analysis
In NAVIGATOR, tezepelumab demonstrated a reduction in the rate of severe asthma exacerbations regardless of the baseline levels of blood eosinophils, FeNO, as well as allergic status (determined by a perennial aeroallergen specific IgE). Similar results were seen in PATHWAY. See Figure 1.
In NAVIGATOR, reductions in the rate of severe asthma exacerbations were greater with increasing baseline blood eosinophil counts and FeNO values (rate ratio = 0.79 [95% CI: 0.48, 1.28] for patients with both baseline blood eosinophil count <150 cells/µL and baseline FeNO <25 ppb; rate ratio = 0.30 [95% CI: 0.23, 0.40] for patients with both baseline blood eosinophil count ≥150 cells/µL and baseline FeNO ≥25 ppb).
Figure 1. Annualised asthma exacerbation rate ratio over 52 weeks across different baseline biomarkers for the Full Analysis Set (pooled NAVIGATOR and PATHWAY)a:
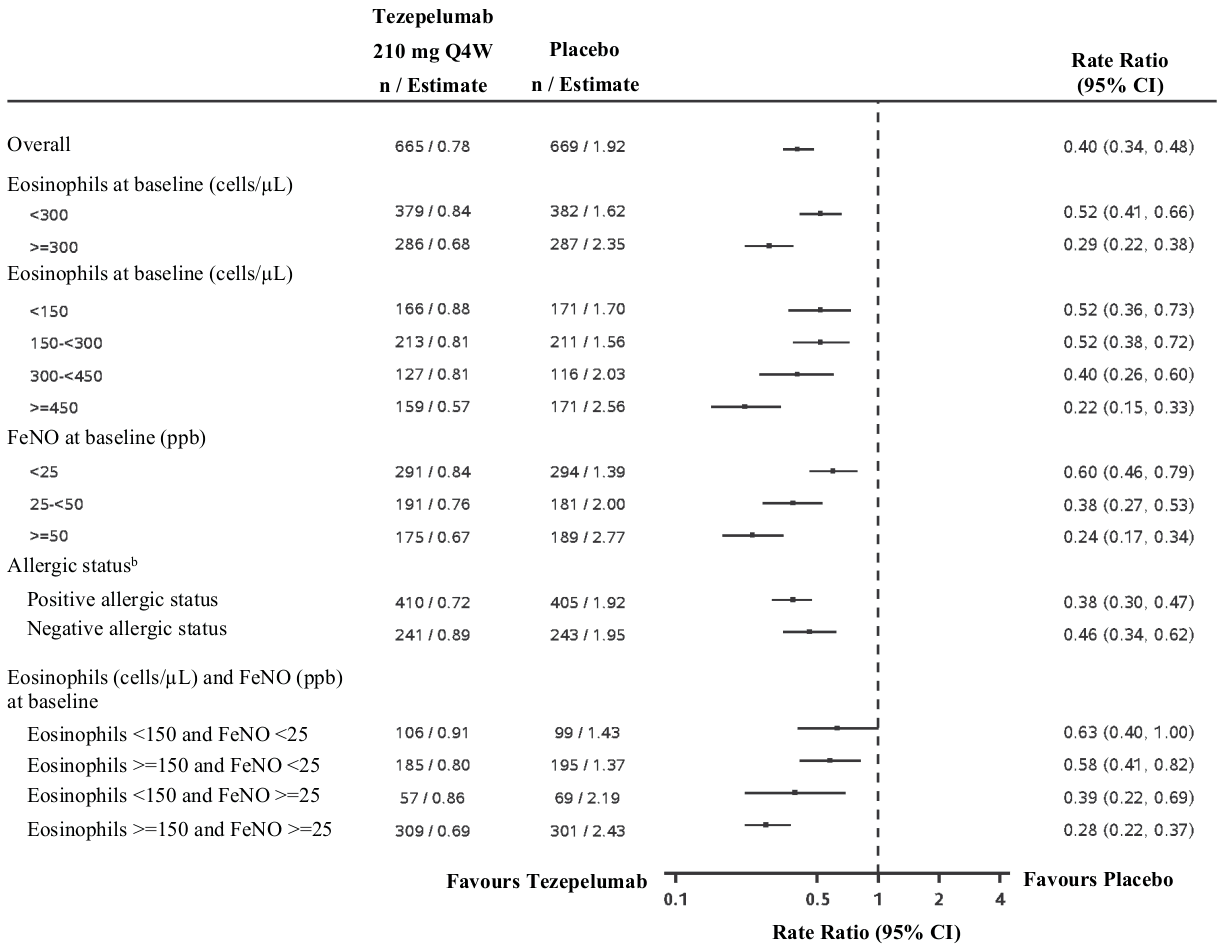
a Time at risk is defined as the total duration of time in which a new exacerbation can occur (i.e. total follow-up time minus time during exacerbation and 7 days after).
b Allergic status as defined by a serum IgE result specific to any perennial aeroallergen in the FEIA panel.
Lung function
Change from baseline in FEV1 was assessed as a secondary endpoint in NAVIGATOR. Compared with placebo, tezepelumab provided clinically meaningful improvements in the mean change from baseline in FEV1 (Table 5).
Patient reported outcomes
Changes from baseline in ACQ-6, Standardised Asthma Quality of Life Questionnaire for ages 12 and older [AQLQ(S)+12] and weekly mean Asthma Symptom Diary (ASD) scores were assessed as secondary endpoints in NAVIGATOR. Severity of wheezing, shortness of breath, cough, and chest tightness were assessed twice daily (morning and evening). Night-time awakening and activity were assessed on a daily basis. The total ASD score was calculated as the mean of 10 items (Table 5).
Improvements in ACQ-6 and AQLQ(S)+12 were seen as early as 2 weeks and 4 weeks after administration of tezepelumab, respectively, and sustained through week 52 in both trials.
Table 5. Results of key secondary endpoints at week 52 in NAVIGATORa:
| Tezepelumab | Placebo | |
|---|---|---|
| Pre-bronchodilator FEV1 | ||
| N | 527 | 531 |
| LS Mean Change from Baseline (L) | 0.23 | 0.10 |
| LS Mean Difference from Placebo (L) (95% CI) | 0.13 (0.08, 0.18) | |
| p-value | <0.001 | |
| AQLQ(S)+12 total score | ||
| N | 525 | 526 |
| LS Mean Change from Baseline | 1.48 | 1.14 |
| Difference from Placebo (95% CI) | 0.33 (0.20, 0.47) | |
| p-value | <0.001 | |
| ACQ-6 score | ||
| N | 527 | 531 |
| LS Mean Change from Baseline | -1.53 | -1.20 |
| Difference from Placebo (95% CI) | -0.33 (-0.46, -0.20) | |
| p-value | <0.001 | |
| ASD | ||
| N | 525 | 531 |
| LS Mean Change from Baseline | -0.70 | -0.59 |
| Difference from Placebo (95% CI) | -0.11 (-0.19, -0.04) | |
| p-value | 0.004 | |
a Estimates are derived from a Mixed Model for Repeated Measures (MMRM) using all available data from patients with at least 1 change from baseline value, including data post-discontinuation.
ACQ-6, Asthma Control Questionnaire 6; AQLQ(S)+12, Standardised Asthma Quality of Life Questionnaire for 12 years and older; ASD Asthma Symptom Diary; CI, Confidence interval; FEV1, Forced expiratory volume in one second; LS, Least square; N, Number of patients contributing to the analysis (FA) with at least 1 change from baseline value
Elderly patients (≥65 years of age)
Of the 665 patients with asthma exposed to tezepelumab 210 mg subcutaneous Q4W in PATHWAY and NAVIGATOR, a total of 119 patients were 65 years of age or older, of which 32 patients were 75 years of age or older. Safety in these age groups were similar to the overall study population. Efficacy in these age groups were similar to the overall study population in NAVIGATOR. PATHWAY did not include sufficient numbers of patients aged 65 and over to determine efficacy in this age group.
Chronic rhinosinusitis with nasal polyps (CRSwNP)
The efficacy of tezepelumab was evaluated in a randomised, double-blind, parallel group, multicentre, placebo-controlled trial (WAYPOINT) of 52 weeks treatment duration conducted in 408 patients aged 18 years and older on standard of care treatment for CRSwNP. This study included patients with symptomatic CRSwNP despite treatment with systemic corticosteroids within the past 12 months and/or any history of sino-nasal surgery, or contraindications/intolerance to either.
Patients received tezepelumab 210 mg or placebo subcutaneously Q4W for 52 weeks in addition to intranasal corticosteroid treatment (e.g. mometasone furoate nasal spray) for CRSwNP.
The demographics and baseline characteristics of WAYPOINT are provided in Table 6 below.
Table 6. Demographics and baseline characteristics of WAYPOINT:
| WAYPOINT N=408a | |
|---|---|
| Mean age (years) (SD) | 50 (14) |
| Male (%) | 65 |
| Mean CRSwNP duration (years) (SD) | 13 (10) |
| Patients with ≥1 prior surgery (%) | 71 |
| Patients with systemic corticosteriod use for CRSwNP in the previous year (%) | 58 |
| Mean total NPSb (SD), range 0-8 | 6.1 (1.2) |
| Mean bi-weekly NCSb, c (SD), range 0-3 | 2.6 (0.5) |
| Mean LMK sinus CT total scoreb (SD), range 0-24 | 19 (4) |
| Mean bi-weekly loss of smellb, d (SD), range 0-3 | 2.9 (0.4) |
| Mean SNOT-22 total scoreb (SD), range 0-110 | 69 (18) |
| Mean blood eosinophils (cells/μL) (SD) | 360 (235) |
| Mean total IgE IU/mL (SD) | 176 (285) |
| Asthma/NSAID-ERD/AERDe (%) | 61 |
| NSAID-ERD/AERD (%) | 17 |
| Allergic rhinitis (%) | 14 |
a Number of patients (N) =407 for mean total NPS; N=406 for mean bi-weekly NCS and mean bi-weekly loss of smell; N=404 for mean LMK sinus CT total score and mean blood eosinophils; N=389 for mean total IgE.
b Higher scores indicate greater disease severity or symptom severity.
c Evaluated as part of the Nasal Polyposis Symptom Diary (NPSD).
d Evaluated via difficulty with sense of smell score in the NPSD.
e All but 3 patients with AERD or NSAID-ERD included in this subgroup also had a diagnosis of asthma reported.
AERD, Aspirin exacerbated respiratory disease; CRSwNP, Chronic rhinosinusitis with nasal polyps; CT, Computed tomography; IgE, Immunoglobulin E; IU, International units; LMK, Lund-Mackay; NCS, Nasal congestion score; NPS, Nasal polyp score; NSAID-ERD, Nonsteroidal anti-inflammatory drug exacerbated respiratory disease; SD, Standard deviation; SNOT-22, 22-item Sino-Nasal Outcome Test
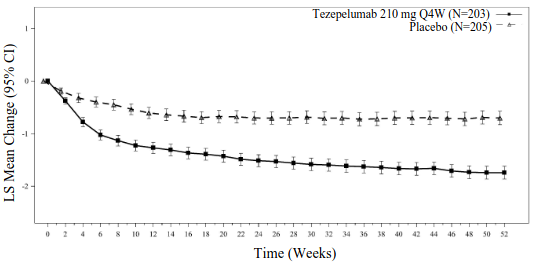
The co-primary efficacy endpoints were change from baseline in total nasal polyp score (NPS) evaluated by nasal endoscopy at week 52 as graded by independent blinded assessors, and change from baseline in bi-weekly mean nasal congestion score (NCS) evaluated as part of the Nasal Polyposis Symptom Diary (NPSD) at week 52. Total NPS was graded on a categorical scale (0-8). Nasal congestion was rated daily by the patients on a 0 to 3 categorical severity scale. Unadjusted p-values are presented for WAYPOINT.
Patients who received tezepelumab had statistically significant improvements in total NPS and bi-weekly mean NCS at week 52 compared with placebo (see Table 7).
The results for the co-primary and key secondary endpoints in WAYPOINT are presented in Table 7.
Table 7. Results of co-primary and key secondary endpoints in WAYPOINT:
| Tezepelumab (N=203) | Placebo (N=205) | p-valuea | |
|---|---|---|---|
| Co-primary endpoints | |||
| NPS at week 52 | |||
| Baseline Mean | 6.1 | 6.1 | |
| LS Mean Change | -2.46 | -0.38 | |
| LS Mean Difference vs. Placebo (95% CI) | -2.08 (-2.40, -1.76) | <0.0001 | |
| NCS at week 52 | |||
Baseline Mean |<>2.59 |<>2.55| |
LS Mean Change|<> -1.74|<> -0.70| |
LS Mean Difference vs. Placebo (95% CI) |\2<> -1.04 (-1.21, -0.87) |<> <0.0001 |
|\4< Key secondary endpoints |
|\4< Loss of smellb at week 52 |
|Baseline Mean |<>2.9 |<>2.8| |
|LS Mean Change |<> -1.26|<> -0.26| |
|LS Mean Difference vs. Placebo (95% CI) |\2<> -1.01 (-1.18, -0.83) |<> <0.0001|
|\4< SNOT-22 at week 52 |
|Baseline Mean |<>68.2 |<>69.2| |
|LS Mean Change|<> -45.02|<> -17.58| |
|LS Mean Difference vs. Placebo (95% CI) |\2<> -27.44 (-32.51, -22.37) |<> <0.0001|
|\4< Lund Mackay score (LMK) at week 52 |
|Baseline Mean |<>18.9 |<>18.5| |
|LS Mean Change|<> -6.27|<> -0.57| |
|LS Mean Difference vs. Placebo (95% CI) |\2<> -5.70 (-6.37, -5.03) |<> <0.0001|
|\4< Time to first sino-nasal surgery decision and/or SCS for CRSwNP up to week 52 |
|Proportion of Patients (%)c |<>5.7 |<>31.4|
| % Reduction vs. Placebo [Hazard ratio (95% CI)] |\2<>92% [0.08 (0.03, 0.16)] |<> <0.0001|
|\4< Time to first sino-nasal surgery decision up to week 52 |
|Proportion of Patients (%)c |<>0.5 |<>22.0|
| % Reduction vs. Placebo [Hazard ratio (95% CI)] |\2<>98% [0.02 (0.00, 0.09)] |<> <0.0001|
|\\4< Time to first SCS use for CRSwNP up to week 52 |
|Proportion of Patients (%)c |<>5.2 |<>19.3|
| % Reduction vs. Placebo [Hazard ratio (95% CI)] |\2<>89% [0.11 (0.04, 0.25)] |<> <0.0001|
|\4< Total Symptom Score (TSS) at week 52 |
|Baseline Mean |<>16.3 |<>16.4|
|LS Mean Change|<> -10.39|<> -3.43|
|LS Mean Difference vs. Placebo (95% CI) |\2<> -6.96 (-8.09, -5.83) |<> <0.0001|
a Unadjusted p-values are presented. Statistically significant after multiplicity adjustment.
b Change from baseline in loss of smell evaluated as bi-weekly mean difficulty with sense of smell item score in the NPSD.
c Kaplan–Meier estimates for the proportion of patients with events.
CRSwNP, Chronic rhinosinusitis with nasal polyps; CI, Confidence interval; LS mean change, Least squared mean change from baseline; reduction in score indicates improvement; NCS, Nasal congestion score; NPS, Nasal polyp score; SCS, Systemic corticosteroids; SD, Standard deviation; SNOT-22, 22-item Sino-Nasal Outcome Test.
Figure 2. LS mean change from baseline in total nasal polyp score (NPS) and bi-weekly mean nasal congestion score (NCS) up to week 52:
Figure 2a. Total NPS
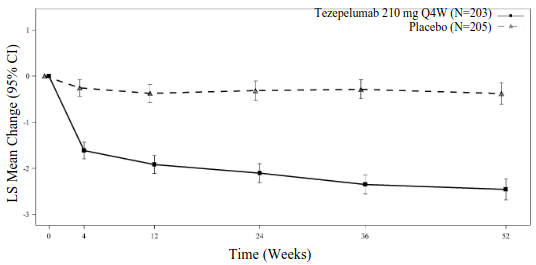
Figure 2b. Bi-weekly mean NCS
Improvement in loss of smell in patients treated with tezepelumab compared with those treated with placebo was seen as early as the first assessment at 2 weeks.
Paediatric population
Asthma
A total of 82 adolescents aged 12 to 17 with severe, uncontrolled asthma were enrolled in NAVIGATOR and received treatment with tezepelumab (n=41) or placebo (n=41). Of the 41 adolescents receiving treatment with tezepelumab, 15 were taking high-dose ICS at baseline. The annualised asthma exacerbation rate observed in adolescents treated with tezepelumab was 0.68 versus 0.97 for placebo (rate ratio 0.70; 95% CI 0.34, 1.46). The LS mean change from baseline for FEV1 observed in adolescents treated with tezepelumab was 0.44 L versus 0.27 L for placebo (LS mean difference 0.17 L; 95% CI -0.01, 0.35). The pharmacodynamic responses in adolescents were generally similar to the overall study population.
The European Medicines Agency has deferred the obligation to submit the results of studies with Tezspire in one or more subsets of the paediatric population in asthma (see section 4.2 for information on paediatric use).
CRSwNP
The European Medicines Agency has waived the obligation to submit the results of studies with Tezspire in all subsets of the paediatric population in CRSwNP (see section 4.2 for information on paediatric use).
5.2. Pharmacokinetic properties
The pharmacokinetics of tezepelumab is similar in patients with asthma and CRSwNP.
The pharmacokinetics of tezepelumab were dose-proportional following subcutaneous administration over a dose range of 2.1 mg to 420 mg.
Absorption
Following a single subcutaneous administration, the maximum serum concentration was reached in approximately 3 to 10 days. Based on population pharmacokinetic analysis, the estimated absolute bioavailability was approximately 77%. There was no clinically relevant difference in bioavailability when administered to different injection sites (abdomen, thigh, or upper arm).
Distribution
Based on population pharmacokinetic analysis, central and peripheral volume of distribution of tezepelumab were 3.9 L and 2.2 L, respectively, for a 70 kg individual.
Metabolism
Tezepelumab is a human monoclonal antibody (IgG2λ) that is degraded by proteolytic enzymes widely distributed in the body and not metabolised by hepatic enzymes.
Elimination
As a human monoclonal antibody, tezepelumab is eliminated by intracellular catabolism and there is no evidence of target-mediated clearance. From population pharmacokinetic analysis, the estimated clearance for tezepelumab was 0.17 L/d for a 70 kg individual. The elimination half-life was approximately 26 days.
Special populations
Age, gender, race
Based on population pharmacokinetic analysis, age, gender and race had no clinically meaningful effects on the pharmacokinetics of tezepelumab.
Body weight
Based on population pharmacokinetic analysis, higher body weight was associated with lower exposure. However, the effect of body weight on exposure had no meaningful impact on efficacy or safety and does not require dose adjustment.
Paediatric patients
Based on the population pharmacokinetic analysis, there was no clinically meaningful age-related difference in the pharmacokinetics of tezepelumab between adults and adolescents aged 12 to 17 years with asthma. Tezepelumab has not been studied in children under 12 years of age for the treatment of asthma or in children under 18 years of age for the treatment of CRSwNP (see section 4.2).
Elderly patients (≥65 years of age)
Based on population pharmacokinetic analysis, there was no clinically meaningful difference in the pharmacokinetics of tezepelumab between patients 65 years of age or older and younger patients.
Renal impairment
No formal clinical studies have been conducted to investigate the effect of renal impairment on tezepelumab. Based on population pharmacokinetic analysis, tezepelumab clearance was similar in patients with mild renal impairment (creatinine clearance 60 to <90 mL/min), moderate renal impairment (creatinine clearance 30 to <60 mL/min) and those with normal renal function (creatinine clearance ≥90 mL/min). Tezepelumab has not been studied in patients with severe renal impairment (creatinine clearance <30 mL/min); however, tezepelumab is not cleared renally.
Hepatic impairment
No formal clinical studies have been conducted to investigate the effect of hepatic impairment on tezepelumab. IgG monoclonal antibodies are not primarily cleared via hepatic pathway; change in hepatic function is not expected to influence tezepelumab clearance. Based on population pharmacokinetic analysis, baseline hepatic function biomarkers (ALT, AST, and bilirubin) had no effect on tezepelumab clearance.
5.3. Preclinical safety data
Non-clinical data revealed no special hazard for humans based on repeated dose toxicity studies including safety pharmacology and fertility evaluations, and an ePPND (enhanced Pre- and Post-Natal Development) reproductive toxicity study in cynomolgus monkeys at doses of up to 300 mg/kg/week (producing exposures of greater than 100-times the clinical exposure at maximum recommended human dose [MRHD]).
Tezepelumab is excreted in milk in monkeys, although at low concentrations (<1%).
Tezepelumab is a monoclonal antibody, as such genotoxicity and carcinogenicity studies have not been conducted.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.