THALIDOMIDE CELGENE Hard capsule Ref.[8640] Active ingredients: Thalidomide
Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Celgene Europe B.V., Winthontlaan 6 N, 3526 KV Utrecht, Netherlands
Pharmacodynamic properties
Pharmacotherapeutic group: immunosuppressants, other immunosuppressants
ATC code: L04AX02
Thalidomide has a chiral centre and is used clinically as a racemate of (+) - (R) and (-) - (S)-thalidomide. The spectrum of activity of thalidomide is not fully characterised.
Mechanism of action
Thalidomide shows immunomodulatory, anti-inflammatory and potential anti-neoplastic activities. Data from in vitro studies and clinical trials suggest that the immunomodulatory, anti-inflammatory and anti-neoplastic effects of thalidomide may be related to suppression of excessive tumour necrosis factor-alpha (TNF-α) production, down-modulation of selected cell surface adhesion molecules involved in leukocyte migration and anti-angiogenic activity. Thalidomide is also a non-barbiturate centrally active hypnotic sedative. It has no antibacterial effects.
Clinical efficacy and safety
Results from IFM 99-06, a Phase 3, randomised, open label, parallel group, multicentre study have demonstrated a survival advantage when thalidomide is used in combination with melphalan and prednisone for 12 cycles of 6 weeks in the treatment of newly diagnosed multiple myeloma patients. In this study the age range of patients was 65-75 years, with 41% (183/447) of patients 70 years old or older. The median dose of thalidomide was 217 mg and >40% of patients received 9 cycles. Melphalan and prednisone were dosed at 0.25 mg/kg/day and 2 mg/kg/day respectively on days 1 to 4 of each 6 weeks cycle.
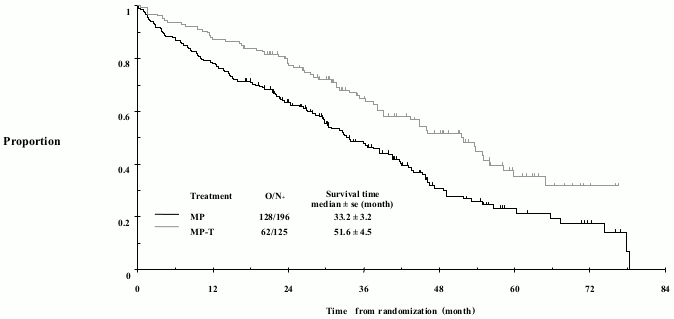
Further to the per protocol analysis, an update was conducted for the IFM 99-06 study providing an additional 15 months follow-up data. The median overall survival (OS) was 51.6 ± 4.5 and 33.2 ± 3.2 months in the MPT and MP groups, respectively (97.5% CI 0.42 to 0.84). This 18 month difference was statistically significant with a hazard ratio of reduction of risk of death in the MPT arm of 0.59, 97.5% confidence interval of 0.42-0.84 and p-value of <0.001 (see Figure 1).
Figure 1. Overall survival according to treatment:
Paediatric Population
The European Medicines Agency has waived the obligation to submit the results of studies with thalidomide in all subsets of the paediatric population in multiple myeloma (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
Absorption
Absorption of thalidomide is slow after oral administration. The maximum plasma concentrations are reached 1-5 hours after administration. Co-administration of food delayed absorption but did not alter the overall extent of absorption.
Distribution
The plasma protein binding of the (+) - (R) and (-) - (S) enantiomers was found to be 55 % and 65 % respectively. Thalidomide is present in the semen of male patients at levels similar to plasma concentrations (see section 4.4). The distribution of thalidomide is not influenced by age, gender, renal function and blood chemistry variables, to any significant level.
Biotransformation
Thalidomide is metabolised almost exclusively by non-enzymatic hydrolysis. In plasma, unchanged thalidomide represents 80% of the circulatory components. Unchanged thalidomide was a minor component (<3% of the dose) in urine. In addition to thalidomide, hydrolytic products N-(o-carboxybenzoyl) glutarimide and phthaloyl isoglutamine formed via non-enzymatic processes are also present in plasma and in majority in urine. Oxidative metabolism does not contribute significantly to the overall metabolism of thalidomide. There is minimal cytochrome P450 catalysed hepatic metabolism of thalidomide. There are in vitro data indicating that prednisone may give rise to enzyme induction which could reduce the systemic exposure of concomitantly used medicinal products. The in vivo relevance of these findings is unknown.
Elimination
The mean elimination half-life of thalidomide in plasma following single oral doses between 50 mg and 400 mg was 5.5 to 7.3 hours. Following a single oral dose of 400 mg of radio-labelled thalidomide, the total mean recovery was 93.6% of the administered dose by day 8. The majority of the radioactive dose was excreted within 48 hour following dose administration. The major route of excretion was via the urine (>90%) while faecal excretion was minor.
There is a linear relationship between body weight and estimated thalidomide clearance; in multiple myeloma patients with body weight from 47-133 kg, thalidomide clearance ranged from approximately 6-12 L/h, representing an increase in thalidomide clearance of 0.621 L/h per 10 kg body weight increase.
Linearity/non-linearity
Total systemic exposure (AUC) is proportional to dose at single-dose conditions. No time dependency of the pharmacokinetics has been observed.
Hepatic and renal impairment
The extent of thalidomide metabolism by the liver cytochrome P450 system is minimal and intact thalidomide is not excreted by the kidney. Measures of renal function (CrCl) and liver function (blood chemistry) indicate minimal effect of kidney and liver function on the pharmacokinetics of thalidomide. As such the metabolism of thalidomide is not expected to be affected by hepatic or renal dysfunction. Data from patients with end-stage renal disease suggest no impact of kidney function on thalidomide pharmacokinetics.
Preclinical safety data
In the male dog, after one year of dosing, reversible bile plugs in canaliculi were observed at exposures greater than 1.9-fold the human exposure.
Decreased platelet counts were noted in the mouse and rat studies. The latter appears to be related to thalidomide and occurred at exposures greater than 2.4-fold the human exposure. This decrease did not result in clinical signs.
In a one-year dog study, enlarged and/or blue discoloration of mammary glands and prolonged estrus were observed in females at exposures equal to 1.8 or greater than 3.6-fold the human exposure, respectively. The relevance to humans is unknown.
The effect of thalidomide on thyroid function was assessed in both rats and dogs. No effects were observed in dogs; however in rats, there was an apparent dose-dependent decrease in total and free T4 that was more consistent in the female.
No mutagenic or genotoxic effect has been revealed when thalidomide was assayed in a standard battery of genotoxicity tests. No evidence of carcinogenicity was observed at exposures approximately 15, 13 and 39 times the estimated clinical AUC at the recommended starting dose in mice, male rats and female rats respectively.
Animal studies have demonstrated differences in species susceptibility to the teratogenic effects of thalidomide. In humans, thalidomide is a proven teratogen.
A study in rabbits demonstrated no effect on fertility indices in males or females although testicular degeneration was observed in males.
A peri- and postnatal toxicity study performed in rabbits with thalidomide administered at doses up to 500 mg/kg/day resulted in abortions, increased stillbirths and decreased pup viability during lactation. Pups from mothers treated with thalidomide had increased abortions, reduced body weight gain, alterations in learning and memory, decreased fertility, and reduced pregnancy index.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.