Source: European Medicines Agency (EU) Revision Year: 2020 Publisher: medac, Gesellschaft für klinische Spezialpräparate mbH, Theaterstr. 6, 22880, Wedel, Germany
Pharmacotherapeutic group: Antineoplastic agents, alkylating agents
ATC code: L01AB02
Treosulfan is a prodrug of a bifunctional alkylating agent with cytotoxic activity to haematopoietic precursor cells. The activity of treosulfan is due to the spontaneous conversion into a mono-epoxide intermediate and L-diepoxybutan (see section 5.2). The epoxides formed alkylate nucleophilic centres of deoxyribonucleic acid (DNA) and are able to induce DNA cross-links which are considered responsible for the stem cell depleting and antineoplastic effects.
Treosulfan has a broad antineoplastic and antileukaemic activity. This was demonstrated against transplanted mouse and rat lymphomas/leukaemias, sarcomas and hepatomas, human tumour xenografts, human tumour biopsies and cell lines.
The immunosuppressive effects of treosulfan are attributed to its toxicity against primitive and committed progenitor cells, T and NK cells, reduction of cellularity of primary and secondary lymphatic organs and a preclusive effect on the ‘cytokine storm’ that precedes the development of Graft-versus-Host-Disease (GvHD) and is involved in the pathogenesis of veno-occlusive disease.
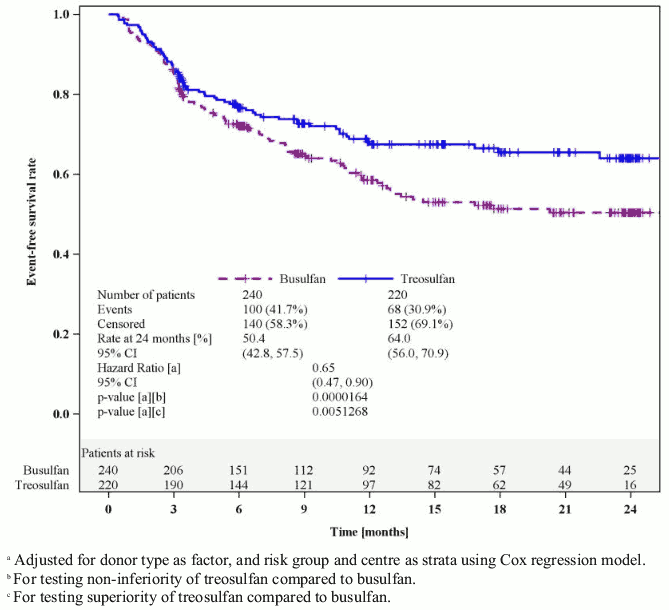
In the pivotal phase III trial, adult patients with acute myeloid leukaemia (AML) or myelodysplastic syndrome (MDS) and increased risk for standard conditioning therapies because of higher age (≥50 years) or comorbidities (haematopoietic cell transplantation comorbidity index [HCT-CI] score >2) were randomised to receive a conditioning regimen with 3 × 10 g/m² treosulfan combined with fludarabine (FT10; n=220) or a regimen of intravenous busulfan (total dose 6.4 mg/kg) combined with fludarabine (FB2; n=240), followed by alloHSCT. 64% of patients had AML and 36% MDS. The median age of patients was 60 years (range 31–70 years); 25% of patients were older than 65 years. The primary endpoint of this study was event-free survival (EFS) after 2 years. Events were defined as relapse of disease, graft failure or death (whatever occurred first). Non-inferiority of FT 10 versus the reference FB2 was statistically proven (Figure 1).
Figure 1. Kaplan-Meier estimates of event-free survival (Full Analysis Set):
Analyses of EFS at 2 years for various pre-defined subgroups (donor type, risk group, disease, age group, HCT-CI score, remission status at study entry, and various combinations of these parameters) were always in favour of the treosulfan regimen (hazard ratio [HR] of FT 10 vs. FB2 <1), with only one exception (risk group I of MDS patients; HR 1.14 [95% CI 0.48, 2.63]). Further results are shown in Table 1.
Table 1. Treatment results at 24 months (Full analysis set):
| Parameter | Treosulfan | Busulfan | Hazard ratiob (95% CI) | P valueb |
|---|---|---|---|---|
| Number of patients | 220 | 240 | ||
| Overall survivala, % (95% CI) | 71.3 (63.6, 77.6) | 56.4 (48.4, 63.6) | 0.61 (0.42, 0.88) | 0.0082 |
| Cumulative incidence of relapse/progression, % (95% CI) | 24.6 (17.8, 31.3) | 23.3 (17.6, 29.0) | 0.87 (0.59, 1.30) | 0.5017 |
| Cumulative incidence of transplant-related mortality, % (95% CI) | 12.1 (8.1, 17.7) | 28.2 (21.4, 36.5) | 0.54 (0.32, 0.91) | 0.0201 |
a Based on Kaplan-Meier estimates; badjusted for donor type, risk group and centre using Cox regression model
Results of GvHD are shown in Table 2.
Table 2. Cumulative incidence of GvHD (Full analysis set):
| Parameter | Treosulfan | Busulfan | P value |
|---|---|---|---|
| Number of patients | 220 | 240 | |
| Acute GvHD, all Grades; % (95% CI) | 52.1 (45.5, 58.7) | 58.8 (52.5, 65.0) | 0.1276 |
| Acute GvHD, Grades III/IV; % (95% CI) | 6.4 (3.2, 9.6) | 9.6 (5.9, 13.3) | 0.2099 |
| Chronic GvHDa, % (95% CI) | 60.1 (49.8, 70.3) | 60.7 (53.1, 68.4) | 0.5236 |
| Extensive chronic GvHDa, % (95% CI) | 18.4 (12.0, 24.8) | 26.1 (19.2, 33.1) | 0.1099 |
a Up to 2 years after alloHSCT
There is limited information available on treosulfan-based conditioning (FT14 regimen ± thiotepa; see section 4.2) in adult patients with non-malignant disorders (NMD). The main indications for an alloHSCT with treosulfan conditioning in adult NMD patients are haemoglobinopathies (e.g. sickle cell disease, thalassaemia major [TM]), primary immune deficiency, hemophagocytic disorder, immune dysregulatory disorder and bone marrow failure).
In one study, 31 NMD patients were treated with the FT14 regimen plus anti-thymocyte globulin. The age of the patients ranged from 0.4 to 30.5 years, and 29% had HCT-CI scores >2. All patients engrafted, with a median time to neutrophil engraftment of 21 (range, 12–46) days. The two-year projected overall survival was 90%. Complete disease responses were observed in 28 patients (90%), as measured by clinical symptoms and laboratory assays (Burroughs LM et al., Biology of Blood and Marrow Transplantation 2014; 20(12):1996-2003).
An Italian group treated 60 TM patients (age range 1-37 years; including 12 adults) with the FT14 plus thiotepa regimen. All patients engrafted except one, who died on day +11; the median time to neutrophil and platelet recovery was 20 days. With a median follow-up of 36 months (range, 4-73), the 5-year overall survival probability was 93% (95% CI 83-97%). No difference in terms of outcome was observed between children and adults (Bernardo ME et al.; Blood 2012; 120(2):473-6).
A retrospective comparison of treosulfan-based (n=16) versus busulfan-based (n=81) conditioning in adult patients revealed quite comparable survival rates (70.3 ± 15.1% vs. 69.3 ± 5.5%), while risk for acute GvHD was lower in the treosulfan group (odds ratio 0.28; 95% CI 0.12-0.67; P=0.004) (Caocci G et al.; American Journal of Hematology 2017; 92(12):1303-1310).
The efficacy and safety of treosulfan-based conditioning was evaluated in 70 patients with acute lymphoblastic leukaemia (ALL), AML, MDS, or juvenile myelomonocytic leukaemia (JMML) who received a conditioning regimen with treosulfan and fludarabine with (n=65) or without (n=5) thiotepa (see section 4.2). A total of 37 patients (52.9%) were younger than 12 years.
No patient experienced a primary graft failure but one patient with ALL experienced a secondary graft failure. The incidence of complete donor-type chimerism was 94.2% (90% CI 87.2-98.0%) at day +28 visit, 91.3% (90% CI 83.6-96.1%) at day +100 visit and 91.2% (90% CI 82.4-96.5%) at month 12 visit.
The overall survival at 12 months is 91.4% (90% CI 83.9-95.5%). A total of 7 of the 70 patients (10.0%) died, two patients because of relapse/progression, three patients transplant-related and two further patients for other reasons. The freedom from transplant-related mortality until day +100 after HSCT (primary endpoint) is 98.6% (90% CI 93.4–99.7%) because one of the 70 patients died due to transplantation/treatment-related cause until day +100 after HSCT. Transplant-related mortality at 12 months is 2.9% (90% CI 0.9–8.9%). Eleven patients had a relapse/progression. The cumulative incidence of relapse/progression is 15.7% (90% CI 8.6-22.9%) at month +12.
The European Medicines Agency has deferred the obligation to submit the results of a study with treosulfan-based conditioning in paediatric patients with non-malignant diseases (see section 4.2 for information on paediatric use).
Treosulfan is a prodrug that is spontaneously converted under physiological conditions (pH 7.4; 37°C) into a monoepoxide intermediate and L-diepoxybutane with a half-life of 2.2 hours.
After intravenous administration, peak plasma levels are reached at the end of the infusion time. Maximum plasma levels (mean ± SD) in adult patients after a 2-hour intravenous infusion of 10, 12, or 14 g/m² treosulfan were 306 ± 94 μg/mL, 461 ± 102 μg/mL, and 494 ± 126 μg/mL, respectively.
Treosulfan is rapidly distributed in the body; however, its penetration through the blood-brain-barrier is quite limited (see section 5.3). The volume of distribution in adult patients is about 20–30 litres. No dose accumulation with the recommended daily treatment on three consecutive days was observed. Treosulfan does not bind to plasma proteins.
Under physiological conditions (pH 7.4, temperature 37°C), the pharmacologically inactive treosulfan is converted spontaneously (non-enzymatically) into the active monoepoxide intermediate (S,S-EBDM = (2S,3S)-1,2-epoxybutane-3,4-diol-4-methanesulfonate) and finally to L-diepoxibutane (S,S-DEB = (2S,3S)-1,2:3,4-diepoxybutane). At concentrations up to 100 μM, treosulfan has no unequivocal effect on CYP1A2, 2C9, 2C19, 2D6, or 3A4 activities in vitro. Therefore, treosulfan is unlikely to participate in, or contribute to, potential CYP450-mediated interactions in vivo.
Plasma concentrations of treosulfan decline exponentially and are best described by a first order elimination process fitted by a two-compartment model. The terminal half-life (T1/2β) of intravenously administered treosulfan (up to 47 g/m²) is approximately 2 hours. Approximately 25–40% of the treosulfan dose is excreted unchanged with the urine within 24 hours, nearly 90% of which within the first 6 hours after administration.
Regression analysis of the area under the curve (AUC0-∞) versus treosulfan dose indicated a linear correlation.
No pharmacokinetic studies with treosulfan were done in patients with severe renal or hepatic impairment, because such patients are generally excluded from alloHSCT. About 25–40% of treosulfan is excreted in urine; however, an influence of renal function on renal clearance of treosulfan was not observed.
Conventional dose calculation simply based on BSA results in a significantly higher exposure (AUC) of smaller children and infants with low BSA compared to adolescents or adults. Therefore, dosing of treosulfan in paediatric patients has to be adapted to the BSA (see section 4.2). Mean apparent terminal half-life of treosulfan was comparable between the different age groups and ranged between 1.3 and 1.6 hours.
Due to its alkylating mechanism of action treosulfan is characterised as a genotoxic compound with carcinogenic potential. Specific reproductive and developmental toxicity studies on treosulfan in animals were not conducted. However, during chronic toxicity tests in rats spermatogenesis and ovarian function were significantly affected. Published literature data report on gonadotoxicity of treosulfan in pre-pubertal and pubertal male and female mice. Published data concerning treatment of mice and rats with L-diepoxibutane (the alkylating transformation product of treosulfan) revealed impairment of fertility, uterine-ovarian and sperm development.
In juvenile rat toxicity studies treosulfan induced slight retardation of physical development and a slightly delayed time-point of vaginal opening in females. A very low penetration of blood-brain-barrier by treosulfan was observed in rats. The treosulfan concentrations in brain tissue were 95%–98% lower than in plasma. However, an approximately 3-fold higher exposure in brain tissue of juvenile rats in comparison to young adults was found.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.