TRUTAKNA Solution for injection Ref.[116723] Active ingredients:
Source: FDA, National Drug Code (US) Revision Year: 2026
12.1. Mechanism of Action
Atacicept-vymj, a BLyS-specific inhibitor and APRIL blocker, is a TACI-Fc fusion glycoprotein that binds B cell activating factor (BAFF) and APRIL with dissociation constants (Kd) of 106 pM and 33 pM, respectively, and reduces BAFF- and APRIL-mediated signaling. BAFF is also known as BlyS.
Reduction in BAFF- and APRIL-mediated signaling decreases production of serum galactose-deficient IgA1 (Gd-IgA1), which is implicated in the pathophysiology of IgAN.
12.2. Pharmacodynamics
Immunoglobulins
In IgAN patients treated with TRUTAKNA once weekly in the Origin 3 study, serum Gd-IgA1, Immunoglobulin A (IgA), Immunoglobulin G (IgG), and Immunoglobulin M (IgM) levels decreased within 4 weeks and these reductions were sustained through Week 36. By Week 36, mean serum levels were reduced from baseline by 68% for Gd-IgA1, 64% for IgA, 36% for IgG, and 75% for IgM.
12.3. Pharmacokinetics
Absorption
Following once weekly SC administration of TRUTAKNA 150 mg in IgAN patients, atacicept-vymj pharmacokinetics increased proportionally over a dose range of 75 to 150 mg. Steady state was achieved after approximately 24 weeks. Following the first SC dose, the maximum atacicept-vymj concentrations were reached approximately 36 hours after atacicept-vymj administration.
Distribution
Central and peripheral volume of distribution were 44 L and 61 L, respectively, in patients with IgAN.
Metabolism/Elimination
No drug metabolism studies have been conducted. Atacicept-vymj is a therapeutic protein that is expected to be catabolized into small peptides and amino acids by general catabolic degradation processes in multiple tissues.
The estimated clearance of atacicept-vymj is 3.2 L/day, and the elimination half-life is approximately 40 days in IgAN patients.
Specific Populations
No clinically significant differences in the pharmacokinetics of atacicept-vymj were observed based on sex, age (18 to 74 years), weight (38.4 to 138 kg), race, and mild to severe renal impairment (eGFR: 22 to 89 mL/min).
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
No carcinogenicity studies have been conducted with atacicept-vymj.
Mutagenesis
Atacicept-vymj was not mutagenic or clastogenic in in vitro Ames, in vitro chromosomal aberration, and in vivo micronucleus assays.
Impairment of Fertility
No effects on male fertility were observed in mice dosed once every two days for 4 weeks prior to mating and throughout the mating period with SC atacicept-vymj up to 80 mg/kg, at exposures approximately 20 times the clinical exposure at the RHD, based on AUC.
Increased pre- and post-implantation losses and reduced number of live fetuses were observed in female mice dosed with SC atacicept-vymj once every two days from 14 days prior to mating to GD 7 at ≥20 mg/kg, at exposures approximately 4 times the clinical exposure at the RHD, based on AUC.
14. Clinical Studies
The effect of TRUTAKNA on proteinuria was evaluated in a randomized, double-blind, placebo-controlled study (Origin 3, NCT04716231) in adults with biopsy-proven IgAN, estimated glomerular filtration rate (eGFR) ≥30 mL/min/1.73 m², proteinuria (defined as either a urine protein-to-creatinine ratio [UPCR] based on a 24-hour urine sample ≥1 g/g or total urine protein excretion ≥1.0 g per 24 hours), on a stable dose of maximally-tolerated renin-angiotensin system (RAS) inhibitor therapy with or without a stable dose of a sodium-glucose cotransporter 2 inhibitor (SGLT2i) and/or a mineralocorticoid receptor antagonist (MRA). Patients with other glomerulopathies or those who had been treated with systemic immunosuppressants in the 12 weeks prior to screening were excluded. Patients were randomized (1:1) to receive either TRUTAKNA 150 mg or placebo once a week via SC injection. Rescue immunosuppressive treatment could be initiated per investigator discretion during the trial.
The efficacy analysis included the first 203 patients who reached the Week 36 visit. At baseline, the mean age was 40 years (range: 18 to 72 years), 57% were male, 43% were White, 55% were Asian, <1% were Black, and 15% were from the United States. At baseline, the geometric mean UPCR was 1.5 g/g, mean eGFR was 65 mL/min/1.73 m², and 60% had hematuria based on urine dipstick. Approximately 62% of patients had a history of hypertension and 8% had a history of type 2 diabetes mellitus. At baseline, nearly all patients were treated with an angiotensin converting enzyme (ACE) inhibitor and/or an angiotensin II receptor blocker (ARB), and 53% of patients were on an SGLT2i. No patients received rescue immunosuppressive therapy during the 36-week study period.
The primary efficacy endpoint was the percent reduction in UPCR based on a 24-hour urine sample at Week 36 relative to baseline (Table 1). The mean percent change from baseline in UPCR over time is shown in Figure 1.
Table 1. Percent Reduction in UPCR at Week 36 in Origin 3:
| TRUTAKNA (N=106) | Placebo (N=97) | |
| Percent reduction in UPCR at Week 36 relative to baseline (95% CI)a | 46 (38, 53) | 7 (-8, 19) |
| TRUTAKNA versus placebo: Percent reduction in UPCR at Week 36 relative to baseline (95% CI)b | 42 (29, 52) | |
| p value | <0.0001 | |
a Percent reduction in UPCR was obtained from the geometric mean ratios, where the natural log–transformed ratio to baseline in UPCR (based on 24-hour urine collection) was analyzed using an MMRM adjusted by stable SGLT2i use at baseline, region, baseline eGFR category, and baseline natural log–transformed UPCR. MMRM analysis included double-blind period data up to Week 36, regardless of treatment discontinuation or initiation of rescue immunosuppressive treatment for IgAN or prohibited therapy; missing values were imputed with jump to reference approach.
b The 99% CI for the treatment effect vs. placebo is (24, 55), corresponding to the two-sided significance level of 0.01 for the primary endpoint at the interim analysis.
Abbreviations: g/g, gram per gram; CI, confidence interval; N, number of randomized subjects in each group; UPCR, urine protein-to-creatinine ratio; MMRM, Mixed Model for Repeated Measures; eGFR, estimated glomerular filtration rate; IgAN, immunoglobulin A nephropathy.
Figure 1. Geometric Mean (95% CI) Percent Change from Baseline in UPCR by Visit in Origin 3:
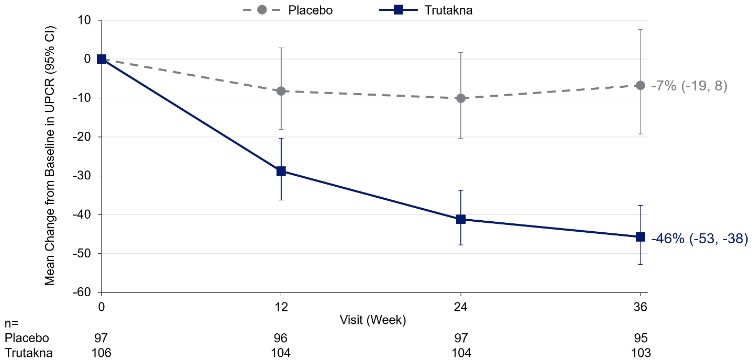
Adjusted percent change relative to baseline in UPCR (sampled from a 24-hour urine collection) with 95% CI reported in the figure were estimated based on the MMRM analysis in Table 1.
"n" represents the number of subjects with observed data for each visit and treatment group.
Abbreviations: CI, confidence interval; MMRM, mixed model repeated measures; UPCR, urine protein-to-creatinine ratio.
The treatment effect on UPCR at Week 36 was generally consistent across subgroups including age, sex, race, and baseline disease characteristics (such as baseline eGFR and proteinuria levels). The treatment effect on UPCR at Week 36 was also similar in patients regardless of concomitant use with an SGLT2i.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.