VAZKEPA Soft capsule Ref.[50397] Active ingredients: Eicosapentaenoic acid
Source: European Medicines Agency (EU) Revision Year: 2026 Publisher: Recordati Industria Chimica e Farmaceutica S.p.A., Via Matteo Civitali 1, 20148 Milan, Italy
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: Lipid modifying agents, Other lipid modifying agents
ATC code: C10AX06
Mechanism of action
Icosapent ethyl is a stable ethyl ester of the omega-3 fatty acid, eicosapentaenoic acid (EPA). The mechanisms of action contributing to reduction of cardiovascular events with icosapent ethyl are not completely understood. The mechanisms are likely multi-factorial including improved lipoprotein profile with reduction of triglyceride-rich lipoproteins, anti-inflammatory, and antioxidant effects, reduction of macrophage accumulation, improved endothelial function, increased fibrous cap thickness/stability, and antiplatelet effects. Each of these mechanisms can beneficially alter the development, progression, and stabilisation of atherosclerotic plaque, as well as the implications of plaque rupture, and preclinical and clinical studies support such benefits with EPA. Systemic and localised anti-inflammatory effects of EPA may result from displacement of pro-inflammatory arachidonic acid (AA), directing catabolism away from eicosanoids (2-series prostaglandins and thromboxanes, and 4-series leukotrienes) to non- or anti-inflammatory mediators. However, the direct clinical meaning of individual findings is not clear.
Pharmacodynamic effects
Icosapent ethyl improves the lipoprotein profile by suppressing cholesterol-, fatty acid- and triglyceride (TG)-synthesising enzymes, increasing fatty acid β-oxidation, and reducing microsomal triglyceride transfer (MTP) protein, resulting in decreased hepatic TG and very low-density lipoprotein (VLDL) synthesis and release. Icosapent ethyl also increases expression of lipoprotein lipase leading to increased TG removal from circulating VLDL and chylomicron particles. In patients with elevated TG levels, icosapent ethyl lowers TG, VLDL, remnant lipoprotein cholesterol, and levels of inflammatory markers such as C-reactive protein. However, TG reduction appears to provide only a minor contribution to the reduction in risk of cardiovascular events with icosapent ethyl.
Clinical efficacy and safety
REDUCE-IT was a multinational, double-blind, randomised, placebo-controlled, event-driven trial in 8,179 (4,089 icosapent ethyl, 4,090 placebo) statin-treated adult patients enrolled with low-density lipoprotein cholesterol (LDL-C) >1.03 mmol/L (40 mg/dL) and ≤2.59 mmol/L (100 mg/dL) and moderately elevated triglyceride (TG) levels (≥1.53 mmol/L and <5.64 mmol/L [≥135 mg/dL and <500 mg/dL] as measured during patient screening, i.e. qualifying visits pre-enrolment) and either established cardiovascular disease (70.7%) or diabetes and other risk factors for cardiovascular disease (29.3%). Patients with established cardiovascular disease were defined as being at least 45 years of age and having a documented history of coronary artery disease, cerebrovascular or carotid disease, or peripheral artery disease. Patients in the other risk group were defined as being at least 50 years of age with diabetes requiring medical treatment and at least one additional risk factor i.e., hypertension or on an antihypertensive medicinal product; age at least 55 years (men) or at least 65 years (women); low high-density lipoprotein cholesterol levels; smoking; raised high-sensitivity C-reactive protein levels; renal impairment; micro or macroalbuminuria; retinopathy; or reduced ankle brachial index. Patients were randomly assigned 1:1 to receive either icosapent ethyl or placebo (as 4 capsules daily). The median follow-up duration was 4.9 years. Overall, 99.8% of patients were followed for vital status until the end of the trial or death.
The baseline characteristics were balanced between the groups, median age at baseline was 64 years (range: 44 years to 92 years), with 46% being at least 65 years old; 28.8% were women. The trial population was 90.2% White, 5.5% Asian, 4.2% identified as Hispanic ethnicity, and 1.9% were Black. Regarding prior diagnoses of cardiovascular disease, 46.7% had prior myocardial infarction, 9.2% had symptomatic peripheral arterial disease, and 6.1% prior unknown stroke or transient ischemic attack (TIA). Selected additional baseline risk factors included hypertension (86.6%), diabetes mellitus (0.7% type 1; 57.8% type 2), eGFR <60 mL/min per 1.73 m² (22.2%), congestive heart failure (17.7%), and current daily cigarette smoking (15.2%). Most patients were taking moderate-intensity (63%) or high-intensity (31%) statin therapy at baseline. Most patients at baseline were taking at least one other cardiovascular medicinal product including antiplatelet and/or antithrombotic agents (85.5%), beta blockers (70.7%), antihypertensives (95.2%), angiotensin converting enzyme (ACE) inhibitors (51.9%), or angiotensin receptor blockers (ARB; 26.9%); 77.5% were taking an ACE inhibitor or ARB. The protocol excluded patients taking PCSK9 inhibitors. On stable background lipid-lowering therapy, the median [Q1, Q3] LDL-C at baseline was 1.9 [1.6, 2.3] mmol/L (75.0 [62.0, 89.0] mg/dL); the mean (SD) was 2.0 (0.5) mmol/L (76.2 [20.3] mg/dL). On stable background lipid-lowering therapy, the median [Q1, Q3] fasting TG was 2.4 [2.0, 3.1] mmol/L (216.0 [176.0, 272.5] mg/dL); the mean (SD) was 2.6 (0.9) mmol/L (233.2 [80.1] mg/dL).
Icosapent ethyl significantly reduced the risk for the primary composite endpoint (time to first occurrence of cardiovascular death, myocardial infarction, stroke, coronary revascularisation, or hospitalisation for unstable angina; p<0.0001) and the key secondary composite endpoint (time to first occurrence of cardiovascular death, myocardial infarction, or stroke; p<0.0001). The results of the primary and secondary efficacy endpoints are shown in Table 2. The Kaplan-Meier estimates of the cumulative incidence of the key secondary composite endpoint over time are shown in Figure 1.
Table 2. Effect of icosapent ethyl on time to first occurrence of cardiovascular events in patients with elevated triglyceride levels and cardiovascular disease or diabetes and other risk factors in REDUCE-IT:
| Icosapent ethyl | Placebo | Icosapent ethyl vs Placebo | |
| N=4 089 n (%) | N=4 090 n (%) | Hazard ratio (95 % CI) | |
| Primary composite endpoint | |||
| Cardiovascular death, myocardial infarction, stroke, coronary revascularisation, hospitalisation for unstable angina (5-point MACE) | 705 (17.2) | 901 (22) | 0.75 (0.68, 0.83) |
| Key secondary composite endpoint | |||
| Cardiovascular death, myocardial infarction, stroke (3-point MACE) | 459 (11.2) | 606 (14.8) | 0.74 (0.65, 0.83) |
| Other secondary endpoints | |||
| Cardiovascular death1 | 174 (4.3) | 213 (5.2) | 0.80 (0.66, 0.98) |
| Death by any cause2 | 274 (6.7) | 310 (7.6) | 0.87 (0.74, 1.02) |
| Fatal or non-fatal myocardial infarction | 250 (6.1) | 355 (8.7) | 0.69 (0.58, 0.81) |
| Fatal or non-fatal stroke | 98 (2.4) | 134 (3.3) | 0.72 (0.55, 0.93) |
| Emergent or urgent coronary revascularisation | 216 (5.3) | 321 (7.8) | 0.65 (0.55, 0.78) |
| Coronary revascularisation3 | 376 (9.2) | 544 (13.3) | 0.66 (0.58, 0.76) |
| Hospitalisation for unstable angina4 | 108 (2.6) | 157 (3.8) | 0.68 (0.53, 0.87) |
1 Cardiovascular death includes adjudicated cardiovascular deaths and deaths of undetermined causality.
2 Death by any cause, or total mortality, is not a component of either the primary composite endpoint or key secondary composite endpoint.
3 The predefined composite secondary endpoint included emergent or urgent revascularisation (p<0.0001); coronary revascularisations is the composite of all revascularisation and was predefined as a tertiary endpoint.
4 Determined to be caused by myocardial ischemia by invasive/non-invasive testing and requiring emergent hospitalisation.
Figure 1. Kaplan-Meier estimated incidence of key secondary composite endpoint in REDUCE-IT:
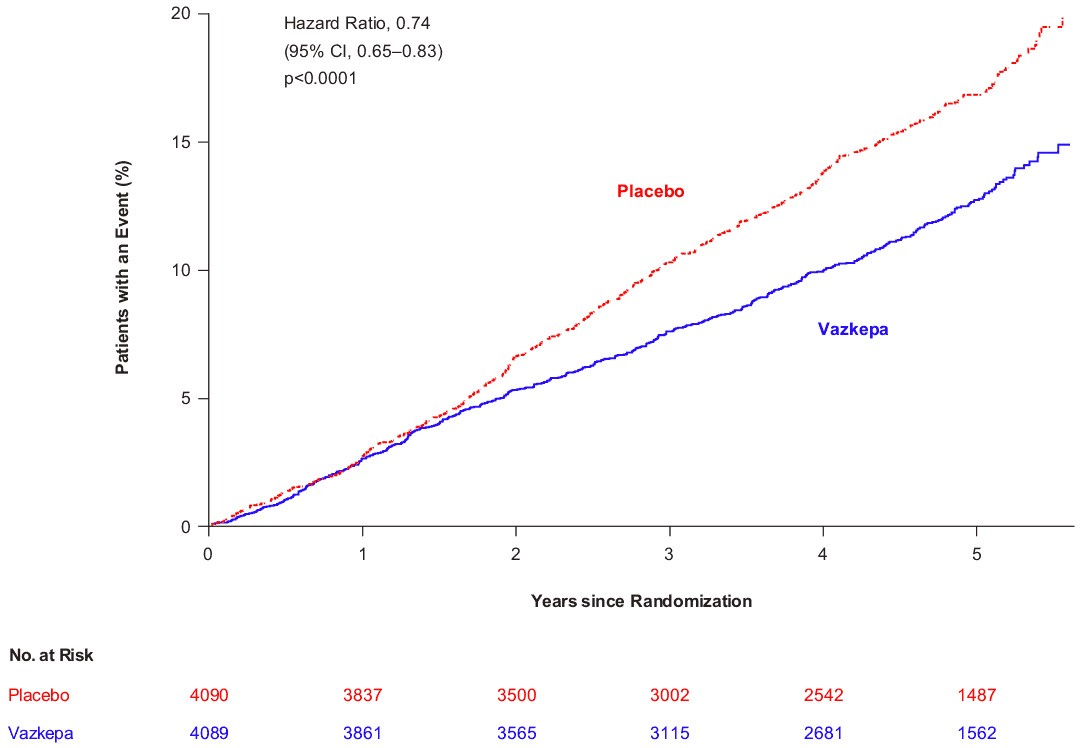
Key secondary composite endpoint consisted of cardiovascular death, myocardial infarction, or stroke (3-point MACE)
Abbreviation: CI confidence interval
The median TG and LDL-C baseline values were similar between the icosapent ethyl group and placebo group. The median change in TG from baseline to Year 1 was -0.4 mmol/L (-39 mg/dL, -18%) in the icosapent ethyl group and 0.1 mmol/L (5 mg/dL, 2%) in the placebo group. The median change in LDL-C from baseline to Year 1 was 0.1 mmol/L (2 mg/dL, 3%) in the icosapent ethyl group and 0.2 mmol/L (7 mg/dL, 10%) in the placebo group. Prespecified analyses of the effect of icosapent ethyl on cardiovascular outcomes in the REDUCE-IT trial showed little to no correlation between either TG or LDL-C response and cardiovascular effect based on baseline or on-study achieved TG or LDL-C levels. See section 5.1 mechanism of action for more information.
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with icosapent ethyl in all subsets of the paediatric population for the treatment of hypertriglyceridemia and to reduce the risk of cardiovascular events (see section 4.2 for information on paediatric use).
5.2. Pharmacokinetic properties
Absorption
After oral administration, icosapent ethyl is de-esterified during the absorption process and the active metabolite EPA is absorbed in the small intestine and enters the systemic circulation mainly via the thoracic duct lymphatic system. Peak plasma concentrations of EPA were reached approximately 5 hours following oral doses of icosapent ethyl.
Icosapent ethyl was administered with or following a meal in all clinical studies; no food effect studies were performed (see section 4.2).
Distribution
The mean volume of distribution at steady-state of EPA is approximately 88 liters. The majority of EPA circulating in plasma is incorporated in phospholipids, triglycerides and cholesteryl esters, and <1% is present as the unesterified fatty acid. Greater than 99% of unesterified EPA is bound to plasma proteins.
Biotransformation and elimination
EPA is mainly metabolised by the liver via beta-oxidation similar to dietary fatty acids. Beta oxidation splits the long carbon chain of EPA into acetyl Coenzyme A, which is converted into energy via the Krebs cycle. Cytochrome P450-mediated metabolism is a minor pathway of elimination of EPA. The total plasma clearance of EPA at steady-state is 684 mL/hr. The plasma elimination half-life (t1/2) of EPA is approximately 89 hours. Icosapent ethyl does not undergo renal excretion.
Pharmacokinetic/pharmacodynamic relationship(s)
Triglycerides level/reduction in hypertriglyceridemia
A linear relationship between EPA levels in plasma or red blood cells (RBCs) and TG reduction was observed in two Phase III studies.
Cardiovascular risk reduction
Analyses of the primary (5-point) and key secondary (3-point) MACE endpoints suggest that ontreatment lipoprotein changes had limited influence on cardiovascular risk reductions, while on-treatment steady-state serum EPA levels accounted for the majority of the relative risk reduction observed in REDUCE-IT. Baseline serum EPA level was 26 μg/mL; compared to patients with an ontreatment steady-state serum EPA level below 100 μg/mL, patients with on-treatment EPA levels ≥175 μg/mL had a >50% reduced risk of a cardiovascular event.
Renal and hepatic impairment
The pharmacokinetics of icosapent ethyl has not been studied in patients with renal or hepatic impairment. Patients did not require routine dose adjustment due to hepatic or renal impairment in a well-controlled cardiovascular outcomes trial of icosapent ethyl.
Other special populations
Elderly
The pharmacokinetics of icosapent ethyl has not been studied in elderly patients (≥65 years of age). Elderly patients did not require routine dose adjustment in well-controlled clinical studies of icosapent ethyl.
Paediatric population
The pharmacokinetics of icosapent ethyl has not been studied in paediatric subjects.
5.3. Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of repeated dose toxicity, genotoxicity, carcinogenic potential and toxicity to reproduction and development.
At the highest dose levels in reproductive and developmental studies, no adverse reactions were observed in rats or rabbits at approximately 6 to 8 times the human equivalent dose based on body surface area comparison. In a rat embryo-foetal trial, no adverse reactions were observed at exposures 6.9-fold higher than the clinical exposure (based on AUC).
Animal studies indicate that icosapent ethyl crosses the placenta and is found in foetal plasma.
Animal studies indicate that icosapent ethyl is excreted in milk.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.