Source: FDA, National Drug Code (US) Revision Year: 2020
The mechanism of action of clozapine is unknown. However, it has been proposed that the therapeutic efficacy of clozapine in schizophrenia is mediated through antagonism of the dopamine type 2 (D2) and the serotonin type 2A (5-HT2A) receptors. VERSACLOZ also acts as an antagonist at adrenergic, cholinergic, histaminergic and other dopaminergic and serotonergic receptors.
Clozapine demonstrated binding affinity to the following receptors: histamine H1 (Ki 1.1 nM), adrenergic α1A (Ki 1.6 nM), serotonin 5-HT6 (Ki 4 nM), serotonin 5-HT2A (Ki 5.4 nM), muscarinic M1 (Ki 6.2 nM), serotonin 5-HT7 (Ki 6.3 nM), serotonin 5-HT2C (Ki 9.4 nM), dopamine D4 (Ki 24 nM), adrenergic α2A (Ki 90 nM), serotonin 5-HT3 (Ki 95 nM), serotonin 5-HT1A (Ki 120 nM), dopamine D2 (Ki 160 nM), dopamine D1 (Ki 270 nM), dopamine D5 (Ki 454 nM), and dopamine D3 (Ki 555 nM).
Clozapine causes little or no prolactin elevation.
Clinical electroencephalogram (EEG) studies demonstrated that clozapine increases delta and theta activity and slows dominant alpha frequencies. Enhanced synchronization occurs. Sharp wave activity and spike and wave complexes may also develop. Patients have reported an intensification of dream activity during clozapine therapy. REM sleep was found to be increased to 85% of the total sleep time. In these patients, the onset of REM sleep occurred almost immediately after falling asleep.
In man, clozapine tablets (25 mg and 100 mg) are equally bioavailable relative to a clozapine solution. VERSACLOZ Oral Suspension is bioequivalent to clozapine marketed tablets.
Following oral administration of 100 mg to 800 mg VERSACLOZ, once daily, the average steady-state peak plasma concentration was 275 ng/mL (range: 105-723 ng/mL), occurring at the average of 2.2 hours (range: 1-3.5 hours) after dosing. The average minimum concentration at steady-state was 75 ng/mL (range: 11-198 ng/mL).
When VERSACLOZ was administered after a high fat meal there was no effect on the AUCss or Cmin,ss, however Cmax was reduced about 20%, and there was a slight delay in Tmax of 0.5 hour from a median Tmax of 2.0 hours under fasted conditions to 2.5 hours under fed conditions. The decrease in Cmax is not considered clinically relevant. Therefore VERSACLOZ may be taken without regard to meals.
Clozapine is approximately 97% bound to serum proteins. The interaction between clozapine and other highly protein-bound drugs has not been fully evaluated but may be important [see Drug Interactions (7)].
VERSACLOZ is almost completely metabolized prior to excretion, and only trace amounts of unchanged drug are detected in the urine and feces. VERSACLOZ is a substrate for many cytochrome P450 isozymes, in particular CYP1A2, CYP2D6, and CYP3A4. Approximately 50% of the administered dose is excreted in the urine and 30% in the feces. The demethylated, hydroxylated, and N-oxide derivatives are components in both urine and feces. Pharmacological testing has shown the desmethyl metabolite (norclozapine) to have only limited activity, while the hydroxylated and N-oxide derivatives were inactive. The mean elimination half-life of clozapine after a single 75 mg dose was 8 hours (range: 4-12 hours), compared to a mean elimination half-life of 12 hours (range: 4-66 hours), after achieving steady-state with 100 mg twice daily dosing.
A comparison of single-dose and multiple-dose administration of clozapine demonstrated that the elimination half-life increased significantly after multiple dosing relative to that after single-dose administration, suggesting the possibility of concentration-dependent pharmacokinetics. However, at steady-state, approximately dose-proportional changes with respect to AUC (area under the curve), peak, and minimum clozapine plasma concentrations were observed after administration of 37.5, 75, and 150 mg twice daily.
A pharmacokinetic study was conducted in 16 schizophrenic patients who received clozapine under steady-state conditions. After coadministration of fluvoxamine for 14 days, mean trough concentrations of clozapine and its metabolites, N-desmethylclozapine and clozapine N-oxide, were elevated about three-fold compared to baseline steady-state concentrations.
In a study of schizophrenic patients (n=14) who received clozapine under steady-state conditions, coadministration of paroxetine produced only minor changes in the levels of clozapine and its metabolites. However, other published reports describe modest elevations (less than two-fold) of clozapine and metabolite concentrations when clozapine was taken with paroxetine, fluoxetine, and sertraline.
No specific pharmacokinetic studies were conducted to investigate the effects of renal or hepatic impairment on the pharmacokinetics of clozapine. Higher clozapine plasma concentrations are likely in patients with significant renal or hepatic impairment when given usual doses.
A subset (3%–10%) of the population has reduced activity of CYP2D6 (CYP2D6 poor metabolizers). These individuals may develop higher than expected plasma concentrations of clozapine when given usual doses.
No carcinogenic potential was demonstrated in long-term studies in mice and rats at doses up to 0.3 times and 0.4 times, respectively, the maximum recommended human dose (MRHD) of 900 mg/day on a mg/m² body surface area basis.
Clozapine was not genotoxic when tested in the following gene mutation and chromosomal aberration tests: the bacterial Ames test, the in vitro mammalian V79 in Chinese hamster cells, the in vitro unscheduled DNA synthesis in rat hepatocytes, or the in vivo micronucleus assay in mice.
Clozapine had no effect on any parameters of fertility, pregnancy, fetal weight, or postnatal development when administered orally to male rats 70 days before mating and to female rats for 14 days before mating at doses up to 0.4 times the MRHD of 900 mg/day on a mg/m² body surface area basis.
The efficacy of clozapine in treatment-resistant schizophrenia was established in a multicenter, randomized, double-blind, active-controlled (chlorpromazine) study in patients with a DSM-III diagnosis of schizophrenia who had inadequate responses to at least 3 different antipsychotics (from at least 2 different chemical classes) during the preceding 5 years. The antipsychotic trials must have been judged adequate; the antipsychotic dosages must have been equivalent to or greater than 1000 mg per day of chlorpromazine for a period of at least 6 weeks, each without significant reduction of symptoms. There must have been no period of good functioning within the preceding 5 years. Patients must have had a baseline score of at least 45 on the investigator-rated Brief Psychiatric Rating Scale (BPRS). On the 18-item BPRS, 1 indicates the absence of symptoms, and 7 indicates severe symptoms; the maximum potential total BPRS score is 126. At baseline, the mean BPRS score was 61. In addition, patients must have had a score of at least 4 on at least two of the following four individual BPRS items: conceptual disorganization, suspiciousness, hallucinatory behavior, and unusual thought content. Patients must have had a Clinical Global Impressions – Severity Scale score of at least 4 (moderately ill).
In the prospective, lead-in phase of the trial, all patients (N=305) initially received single-blind treatment with haloperidol (the mean dose was 61 mg per day) for 6 weeks. More than 80% of patients completed the 6-week trial. Patients with an inadequate response to haloperidol (n=268) were randomized to double-blind treatment with clozapine (N=126) or chlorpromazine (N=142). The maximum daily clozapine dose was 900 mg; the mean daily dose was >600 mg). The maximum daily chlorpromazine dose was 1800 mg; the mean daily dose was >1200 mg.
The primary endpoint was treatment response, predefined as a decrease in BPRS score of at least 20% and either (1) a CGI-S score of ≤3 (mildly ill), or (2) a BPRS score of ≤35, at the end of 6 weeks of treatment. Approximately 88% of patients from the clozapine and chlorpromazine groups completed the 6-week trial. At the end of six weeks, 30% of the clozapine group responded to treatment, and 4% of the chlorpromazine group responded to treatment. The difference was statistically significant (p<0.001). The mean change in total BPRS score was -16 and -5 in the clozapine and chlorpromazine group, respectively; the mean change in the 4 key BPRS item scores was -5 and -2 in the clozapine and chlorpromazine group, respectively; and the mean change in CGI-S score was -1.2 and -0.4, in the clozapine and chlorpromazine group, respectively. These changes in the clozapine group were statistically significantly greater than in the chlorpromazine group (p<0.001 in each analysis).
The effectiveness of clozapine in reducing the risk of recurrent suicidal behavior was assessed in the International Suicide Prevention Trial (InterSePT, a trademark of Novartis Pharmaceuticals Corporation). This was a prospective, randomized, open-label, active-controlled, multicenter, international, parallel-group comparison of clozapine (Clozaril) versus olanzapine (Zyprexa, a registered trademark of Eli Lilly and Company) in 956 patients with schizophrenia or schizoaffective disorder (DSM-IV) who were judged to be at risk for recurrent suicidal behavior. Only about one-fourth of these patients (27%) were considered resistant to standard antipsychotic drug treatment. To enter the trial, patients must have met one of the following criteria:
Dosing regimens for each treatment group were determined by individual investigators and were individualized by patient. Dosing was flexible, with a dose range of 200–900 mg/day for clozapine and 5–20 mg/day for olanzapine. For the 956 patients who received clozapine or olanzapine in this study, there was extensive use of concomitant psychotropics: 84% with antipsychotics, 65% with anxiolytics, 53% with antidepressants, and 28% with mood stabilizers. There was significantly greater use of concomitant psychotropic medications among the patients in the olanzapine group.
The primary efficacy measure was time to (1) a significant suicide attempt, including a completed suicide; (2) hospitalization due to imminent suicide risk, including increased level of surveillance for suicidality for patients already hospitalized; or (3) worsening of suicidality severity as demonstrated by “much worsening” or “very much worsening” from baseline in the Clinical Global Impression of Severity of Suicidality as assessed by the Blinded Psychiatrist (CGI-SS-BP) scale. A determination of whether or not a reported event met criterion 1 or 2 above was made by the Suicide Monitoring Board (SMB), a group of experts blinded to patient data.
A total of 980 patients were randomized to the study and 956 received study medication. Sixty-two percent of the patients were diagnosed with schizophrenia, and the remainder (38%) were diagnosed with schizoaffective disorder. Only about one-fourth of the total patient population (27%) was identified as “treatment-resistant” at baseline. There were more males than females in the study (61% of all patients were male). The mean age of patients entering the study was 37 years of age (range: 18–69). Most patients were Caucasian (71%), 15% were Black, 1% were Asian, and 13% were classified as being of “other” races.
Patients treated with clozapine had a statistically significant longer delay in the time to recurrent suicidal behavior in comparison with olanzapine. This result should be interpreted only as evidence of the effectiveness of clozapine in delaying time to recurrent suicidal behavior and not a demonstration of the superior efficacy of clozapine over olanzapine.
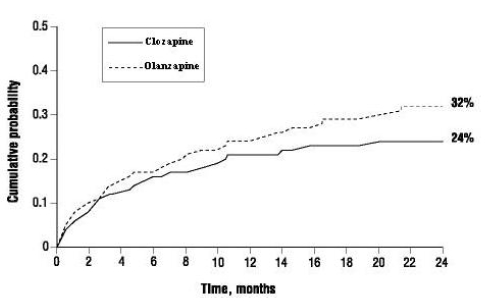
The probability of experiencing (1) a significant suicide attempt, including a completed suicide, or (2) hospitalization because of imminent suicide risk, including increased level of surveillance for suicidality for patients already hospitalized, was lower for clozapine patients than for olanzapine patients at Week 104: clozapine 24% versus olanzapine 32%; 95% CI of the difference: 2%, 14% (Figure 1).
Figure 1. Cumulative Probability of a Significant Suicide Attempt or Hospitalization to Prevent Suicide in Patients with Schizophrenia or Schizoaffective Disorder at High Risk of Suicidality:
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.