VICTOZA Solution for injection Ref.[6953] Active ingredients: Liraglutide
Source: European Medicines Agency (EU) Revision Year: 2023 Publisher: Novo Nordisk A/S, Novo Allé, DK-2880 Bagsværd, Denmark
Pharmacodynamic properties
Pharmacotherapeutic group: Drugs used in diabetes, glucagon-like peptide-1 (GLP-1) analogues
ATC code: A10BJ02
Mechanism of action
Liraglutide is a GLP-1 analogue with 97% sequence homology to human GLP-1 that binds to and activates the GLP-1 receptor. The GLP-1 receptor is the target for native GLP-1, an endogenous incretin hormone that potentiates glucose-dependent insulin secretion from the pancreatic beta cells. Unlike native GLP-1, liraglutide has a pharmacokinetic and pharmacodynamic profile in humans suitable for once daily administration. Following subcutaneous administration, the protracted action profile is based on three mechanisms: self-association, which results in slow absorption; binding to albumin; and higher enzymatic stability towards the dipeptidyl peptidase-4 (DPP-4) and neutral endopeptidase (NEP) enzymes, resulting in a long plasma half-life.
Liraglutide action is mediated via a specific interaction with GLP-1 receptors, leading to an increase in cyclic adenosine monophosphate (cAMP). Liraglutide stimulates insulin secretion in a glucosedependent manner. Simultaneously, liraglutide lowers inappropriately high glucagon secretion, also in a glucose-dependent manner. Thus, when blood glucose is high, insulin secretion is stimulated and glucagon secretion is inhibited. Conversely, during hypoglycaemia liraglutide diminishes insulin secretion and does not impair glucagon secretion. The mechanism of blood glucose lowering also involves a minor delay in gastric emptying. Liraglutide reduces body weight and body fat mass through mechanisms involving reduced hunger and lowered energy intake, GLP-1 is a physiological regulator of appetite and food intake, but the exact mechanism of action is not entirely clear.
In animal studies, peripheral administration of liraglutide led to uptake in specific brain regions involved in regulation of appetite, where liraglutide via specific activation of the GLP-1 receptor (GLP-1R) increased key satiety and decreased key hunger signals, thereby leading to lower body weight.
GLP-1 receptors are also expressed in specific locations in the heart, vasculature, immune system, and kidneys. In mouse models of atherosclerosis, liraglutide prevented aortic plaque progression and reduced inflammation in the plaque. In addition, liraglutide had a beneficial effect on plasma lipids. Liraglutide did not reduce the plaque size of already established plaques.
Pharmacodynamic effects
Liraglutide has 24-hour duration of action and improves glycaemic control by lowering fasting and postprandial blood glucose in patients with type 2 diabetes mellitus.
Clinical efficacy and safety
Both improvement of glycaemic control and reduction of cardiovascular morbidity and mortality are an integral part of the treatment of type 2 diabetes.
Five double-blind, randomised, controlled clinical phase 3a trials were conducted to evaluate the effects of liraglutide on glycaemic control (Table 2). Treatment with liraglutide produced clinically and statistically significant improvements in glycosylated haemoglobin A1c (HbA1c), fasting plasma glucose and postprandial glucose compared with placebo.
These trials included 3,978 exposed patients with type 2 diabetes mellitus (2,501 patients treated with liraglutide), 53.7% men and 46.3% women, 797 patients (508 treated with liraglutide) were ≥65 years of age and 113 patients (66 treated with liraglutide) were ≥75 years of age.
Additional trials were conducted with liraglutide that included 1,901 patients in four unblinded, randomised, controlled clinical trials (including 464, 658, 323 and 177 patients per trial) and one double-blind, randomised, controlled clinical trial in patients with type 2 diabetes mellitus and moderate renal impairment (279 patients).
A large cardiovascular outcomes trial (the LEADER trial) was also conducted with liraglutide in 9,340 patients with type 2 diabetes mellitus at high cardiovascular risk.
Glycaemic control
Monotherapy
Liraglutide monotherapy for 52 weeks resulted in statistically significant and sustained reductions in HbA1c compared with glimepiride 8 mg (-0.84% for 1.2 mg, -1.14% for 1.8 mg vs -0.51% for comparator) in patients previously treated with either diet and exercise or OAD monotherapy at no more than half-maximal dose (Table 2).
Combination with oral antidiabetics
Liraglutide in combination therapy, for 26 weeks, with metformin, glimepiride or metformin and rosiglitazone or SGLT2i ± metformin resulted in statistically significant and sustained reductions in HbA1c compared with patients receiving placebo (Table 2).
Table 2. Liraglutide clinical phase 3a trials in monotherapy (52 weeks) and in combination with oral antidiabetics (26 weeks):
| N | Mean baseline HbA1c (%) | Mean HbA1c change from baseline (%) | Patients (%) achieving HbA1c<7% | Mean baseline weight (kg) | Mean weight change from baseline (kg) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Monotherapy | |||||||||||||
| Liraglutide 1.2 mg | 251 | 8.18 | -0.84* | 42.81, 58.33 | 92.1 | -2.05** | |||||||
| Liraglutide 1.8 mg | 246 | 8.19 | -1.14** | 50.91, 62.03 | 92.6 | -2.45** | |||||||
| Glimepiride 8 mg/day | 248 | 8.23 | -0.51 | 27.81, 30.83 | 93.3 | 1.12 | |||||||
| Add-on to metformin (2,000 mg/day) | |||||||||||||
| Liraglutide 1.2 mg | 240 | 8.3 | -0.97† | 35.31, 52.82 | 88.5 | -2.58** | |||||||
| Liraglutide 1.8 mg | 242 | 8.4 | -1.00† | 42.41, 66.32 | 88.0 | -2.79** | |||||||
| Placebo | 121 | 8.4 | 0.09 | 10.81, 22.52 | 91.0 | -1.51 | |||||||
| Glimepiride 4 mg/day | 242 | 8.4 | -0.98 | 36.31, 56.02 | 89.0 | 0.95 | |||||||
| Add-on to glimepiride (4 mg/day) | |||||||||||||
| Liraglutide 1.2 mg | 228 | 8.5 | -1.08** | 34.51, 57.42 | 80.0 | 0.32** | |||||||
| Liraglutide 1.8 mg | 234 | 8.5 | -1.13** | 41.61, 55.92 | 83.0 | -0.23** | |||||||
| Placebo | 114 | 8.4 | 0.23 | 7.51, 11.82 | 81.9 | -0.10 | |||||||
| Rosiglitazone 4 mg/day | 231 | 8.4 | -0.44 | 21.91, 36.12 | 80.6 | 2.11 | |||||||
| Add-on to metformin (2,000 mg/day) + rosiglitazone (4 mg twice daily) | |||||||||||||
| Liraglutide 1.2 mg | 177 | 8.48 | -1.48 | 57.51 | 95.3 | -1.02 | |||||||
| Liraglutide 1.8 mg | 178 | 8.56 | -1.48 | 53.71 | 94.9 | -2.02 | |||||||
| Placebo | 175 | 8.42 | -0.54 | 28.11 | 98.5 | 0.60 | |||||||
| Add-on to metformin (2,000 mg/day) + glimepiride (4 mg/day) | |||||||||||||
| Liraglutide 1.8 mg | 230 | 8.3 | -1.33* | 53.11 | 85.8 | -1.81** | |||||||
| Placebo | 114 | 8.3 | -0.24 | 15.31 | 85.4 | -0.42 | |||||||
| Insulin glargine4 | 232 | 8.1 | -1.09 | 45.81 | 85.2 | 1.62 | |||||||
| Add-on to SGLT2i5 ± metformin (≥1500 mg/day) | |||||||||||||
| Liraglutide 1.8 mg | 203 | 8.00 | -1.02*** | 54.8*** | 91.0 | -2.92 | Placebo | 100 | 7.96 | -0.28 | 13.9 | 91.4 | -2.06 |
* Superiority (p<0.01) vs active comparator; *Superiority (p<0.0001) vs active comparator; **Superiority (p<0.001) vs active comparator, † Non-inferiority (p<0.0001) vs active comparator
1 all patients; 2 previous OAD monotherapy; 3 previous diet treated patients
5 Victoza add-on to SGLT2i was investigated at all approved doses of SGLT2i
4 the dosing of insulin glargine was open-labelled and was applied according to Guideline for titration of insulin glargine. Titration of the insulin glargine dose was managed by the patient after instruction by the investigator:
Guideline for titration of insulin glargine:
| Self-measured FPG | Increase in insulin glargine dose (IU) |
| ≤5.5 mmol/l (≤100 mg/dl) Target | No adjustment |
| >5.5 and <6.7 mmol/l (>100 and <120 mg/dl) | 0–2 IUa |
| ≥6.7 mmol/l (≥120 mg/dl) | 2 IU |
a According to the individualised recommendation by the investigator at the previous visit, for example depending on whether the patient has experienced hypoglycaemia.
Combination with insulin
In a 104-week clinical trial, 57% of patients with type 2 diabetes treated with insulin degludec in combination with metformin achieved a target HbA1c <7% and the remaining patients continued in a 26-week open label trial and were randomised to add liraglutide or a single dose of insulin aspart (with the largest meal). In the insulin degludec + liraglutide arm, the insulin dose was reduced by 20% in order to minimize the risk of hypoglycaemia. Addition of liraglutide resulted in a statistically significantly greater reduction of HbA1c (-0.73% for liraglutide vs -0.40% for comparator) and body weight (-3.03 vs 0.72 kg). The rate of hypoglycaemic episodes (per patient year of exposure) was statistically significantly lower when adding liraglutide compared to adding a single dose of insulin aspart (1.0 vs 8.15; ratio: 0.13; 95% CI: 0.08 to 0.21).
In a 52-week clinical trial, the addition of insulin detemir to liraglutide 1.8 mg and metformin in patients not achieving glycaemic targets on liraglutide and metformin alone resulted in a HbA1c decrease from baseline of 0.54%, compared to 0.20% in the liraglutide 1.8 mg and metformin control group. Weight loss was sustained. There was a small increase in the rate of minor hypoglycaemic episodes (0.23 versus 0.03 events per patient years).
In the LEADER trial, (see subsection Cardiovascular evaluation), 873 patients were on premix insulin (with or without OAD(s)) at baseline and at least for the following 26 weeks. The mean HbA1c at baseline was 8.7% for liraglutide and placebo. At week 26, the estimated mean change in HbA1c was -1.4% and -0.5% for liraglutide and placebo, respectively, with an estimated treatment difference of -0.9 [-1.00; -0.70] 95% CI . The safety profile of liraglutide in combination with premix insulin was overall comparable to that observed for placebo in combination with premix insulin (see section 4.8).
Use in patients with renal impairment
In a double-blind trial comparing the efficacy and safety of liraglutide 1.8 mg versus placebo as add-on to insulin and/or OAD in patients with type 2 diabetes and moderate renal impairment, liraglutide was superior to placebo treatment in reducing HbA1c after 26 weeks (-1.05% vs -0.38%). Significantly more patients achieved HbA1c below 7% with liraglutide compared with placebo (52.8% vs 19.5%). In both groups a decrease in body weight was seen: -2.4 kg with liraglutide vs -1.09 kg with placebo. There was a comparable risk of hypoglycaemic episodes between the two treatment groups. The safety profile of liraglutide was generally similar to that observed in other studies with liraglutide.
Proportion of patients achieving reductions in HbA1c
Liraglutide alone resulted in a statistically significant greater proportion of patients achieving HbA1c ≤6.5% at 52 weeks compared with patients receiving glimepiride (37.6% for 1.8 mg and 28.0% for 1.2 mg vs 16.2% for comparator).
Liraglutide in combination with metformin, glimepiride, or metformin and rosiglitazone resulted in a statistically significant greater proportion of patients achieving an HbA1c ≤6.5% at 26 weeks compared with patients receiving these agents alone.
Fasting plasma glucose
Treatment with liraglutide alone and in combination with one or two oral antidiabetic drugs resulted in a reduction in fasting plasma glucose of 13–43.5 mg/dl (0.72–2.42 mmol/l). This reduction was observed within the first two weeks of treatment.
Postprandial glucose
Liraglutide reduced postprandial glucose across all three daily meals by 31–49 mg/dl (1.68– 2.71 mmol/l).
Beta-cell function
Clinical trials with liraglutide indicate improved beta-cell function based on measures such as the homeostasis model assessment for beta-cell function (HOMA-B) and the proinsulin to insulin ratio. Improved first and second phase insulin secretion after 52 weeks treatment with liraglutide was demonstrated in a subset of patients with type 2 diabetes (n=29).
Body weight
Treatment with liraglutide in combination with metformin, metformin and glimepiride, metformin and rosiglitazone or SGLT2i with or without metformin was associated with a sustained weight reduction in the range from 0.86 kg to 2.62 kg compared with placebo.
Larger weight reduction was observed with increasing body mass index (BMI) at baseline.
Cardiovascular evaluation
Post-hoc analysis of serious major adverse cardiovascular events (cardiovascular death, myocardial infarction, stroke) from all intermediate and long-term phase 2 and 3 trials (ranging from 26 and up to 100 weeks duration) including 5,607 patients (3,651 exposed to liraglutide), showed no increase in cardiovascular risk (incidence ratio of 0.75 (95% CI 0.35; 1.63)) for liraglutide versus all comparators.
The Liraglutide Effect and Action in Diabetes Evaluation of Cardiovascular Outcome Results (LEADER) trial, was a multicentre, placebo-controlled, double-blind clinical trial. 9,340 patients were randomly allocated to either liraglutide (4,668) or placebo (4,672), both in addition to standards of care for HbA1c and cardiovascular (CV) risk factors. Primary outcome or vital status at end of trial was available for 99.7% and 99.6% of participants randomised to liraglutide and placebo, respectively. The duration of observation was a minimum of 3.5 years and up to a maximum of 5 years. The study population included patients ≥65 years (n=4,329) and ≥75 years (n=836) and patients with mild (n=3,907), moderate (n=1,934) or severe (n=224) renal impairment. The mean age was 64 years and the mean BMI was 32.5 kg/m². The mean duration of diabetes was 12.8 years.
The primary endpoint was the time from randomisation to first occurrence of any major adverse cardiovascular events (MACE): CV death, non-fatal myocardial infarction or non-fatal stroke. Liraglutide was superior in preventing MACE vs placebo (Figure 1). The estimated hazard ratio was consistently below 1 for all 3 MACE components.
Liraglutide also significantly reduced the risk of expanded MACE (primary MACE, unstable angina pectoris leading to hospitalisation, coronary revascularisation, or hospitalisation due to heart failure) and other secondary endpoints (Figure 2).
Figure 1. Kaplan Meier plot of time to first MACE – FAS population:
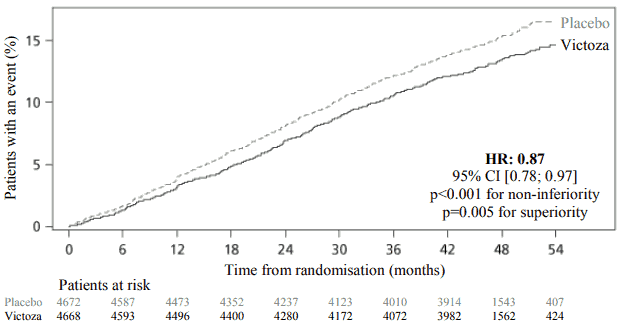
FAS: full analysis set.
Figure 2. Forest plot of analyses of individual cardiovascular event types – FAS population:
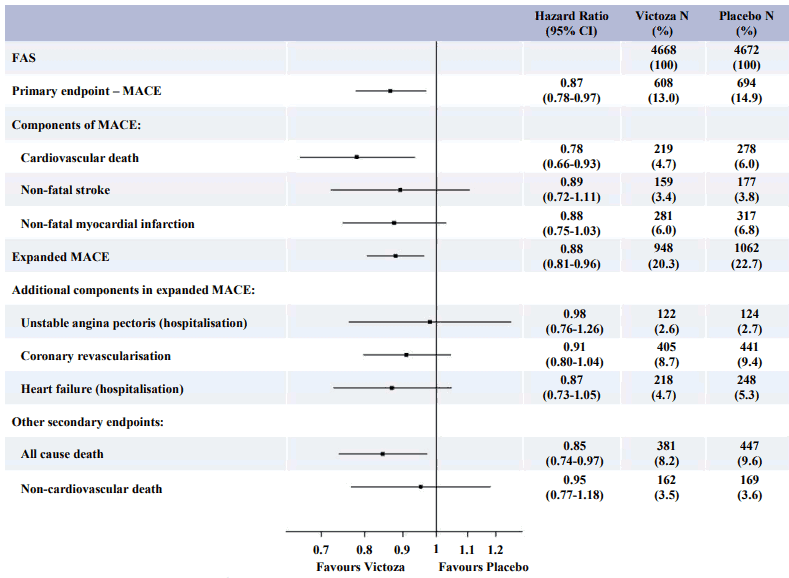
FAS: full analysis set
CI: confidence interval
MACE: major adverse cardiovascular event
%: proportion in percent of subjects with an event
N: number of subjects
A significant and sustained reduction in HbA1c from baseline to month 36 was observed with liraglutide vs placebo, in addition to standard of care (-1.16% vs -0.77%; estimated treatment difference [ETD] -0.40% [-0.45; -0.34]). The need for treatment intensification with insulin was reduced by 48% with liraglutide vs placebo in insulin-naive patients at baseline (HR 0.52 [0.48; 0.57]).
Blood pressure and heart rate
Over the duration of the phase 3a trials, liraglutide decreased the systolic blood pressure on average of 2.3 to 6.7 mmHg from baseline and compared to active comparator the decrease was 1.9 to 4.5 mmHg. A mean increase in heart rate from baseline of 2 to 3 beats per minute has been observed with liraglutide in long-term clinical trials including LEADER. In the LEADER trial, no long-term clinical impact of increased heart rate on the risk of cardiovascular events was observed.
Microvascular evaluation
In the LEADER trial, microvascular events comprised nephropathy and retinopathy outcomes. The analysis of time to first microvascular event for liraglutide vs placebo had a HR of 0.84 [0.73, 0.97]. The HR for liraglutide vs placebo was 0.78 [0.67, 0.92] for time to first nephropathy event and 1.15 [0.87, 1.52] for time to first retinopathy event.
Immunogenicity
Consistent with the potentially immunogenic properties of medicinal products containing proteins or peptides, patients may develop anti-liraglutide antibodies following treatment with liraglutide. On average, 8.6% of patients developed antibodies. Antibody formation has not been associated with reduced efficacy of liraglutide.
Paediatric population
In a double-blind study comparing the efficacy and safety of Victoza 1.8 mg versus placebo as add-on to metformin ± insulin in adolescents and children aged 10 years and above with type 2 diabetes, Victoza was superior to placebo treatment in reducing HbA1c after 26 weeks (-1.06, [-1.65, 0.46]). The treatment difference in HbA1c was 1.3% after additional 26 weeks of open label extension, confirming the sustained glycaemic control with Victoza.
The efficacy and safety profile of Victoza was comparable to that observed in the adult population treated with Victoza. Based on adequate glycaemic control or tolerability, 30% of trial subjects remained on a dose of 0.6 mg, 17% escalated to a dose of 1.2 mg and 53% escalated to a dose of 1.8 mg.
Other clinical data
In an open label trial comparing the efficacy and safety of liraglutide (1.2 mg and 1.8 mg) and sitagliptin (a DPP-4 inhibitor, 100 mg) in patients inadequately controlled on metformin therapy (mean HbA1c 8.5%), liraglutide at both doses was statistically superior to sitagliptin treatment in reducing HbA1c after 26 weeks (-1.24%, -1.50% vs -0.90%, p<0.0001). Patients treated with liraglutide had a significant decrease in body weight compared to that of patients treated with sitagliptin (-2.9 kg and -3.4 kg vs -1.0 kg, p<0.0001). Greater proportions of patients treated with liraglutide experienced transient nausea vs patients treated with sitagliptin (20.8% and 27.1% for liraglutide vs 4.6% for sitagliptin). The reductions in HbA1c and superiority vs sitagliptin observed after 26 weeks of liraglutide treatment (1.2 mg and 1.8 mg) were sustained after 52 weeks of treatment (-1.29% and -1.51% vs -0.88%, p<0.0001). Switching patients from sitagliptin to liraglutide after 52 weeks of treatment resulted in additional and statistically significant reduction in HbA1c (-0.24% and -0.45%, 95% CI: -0.41 to -0.07 and -0.67 to -0.23) at week 78, but a formal control group was not available.
In an open label trial comparing the efficacy and safety of liraglutide 1.8 mg once daily and exenatide 10 mcg twice daily in patients inadequately controlled on metformin and/or sulfonylurea therapy (mean HbA1c 8.3%), liraglutide was statistically superior to exenatide treatment in reducing HbA1c after 26 weeks (-1.12% vs -0.79%; estimated treatment difference: -0.33; 95% CI: -0.47 to -0.18). Significantly more patients achieved HbA1c below 7% with liraglutide compared with exenatide (54.2% vs 43.4%, p=0.0015). Both treatments resulted in mean body weight loss of approximately 3 kg. Switching patients from exenatide to liraglutide after 26 weeks of treatment resulted in an additional and statistically significant reduction in HbA1c (-0.32%, 95% CI: -0.41 to -0.24) at week 40, but a formal control group was not available. During the 26 weeks, there were 12 serious events in 235 patients (5.1%) using liraglutide, whereas there were 6 serious adverse events in 232 patients (2.6%) using exenatide. There was no consistent pattern with respect to system organ class of events.
In an open label trial comparing the efficacy and safety of liraglutide 1.8 mg with lixisenatide 20 mcg in 404 patients inadequately controlled on metformin therapy (mean HbA1c 8.4%), liraglutide was superior to lixisenatide in reducing HbA1c after 26 weeks of treatment (-1.83% vs -1.21%, p<0.0001). Significantly more patients achieved HbA1c below 7% with liraglutide compared to lixisenatide (74.2% vs 45.5%, p<0.0001), as well as the HbA1c target below or equal 6.5% (54.6% vs 26.2%, p<0.0001). Body weight loss was observed in both treatment arms (-4.3 kg with liraglutide and -3.7 kg with lixisenatide). Gastrointestinal adverse events were more frequently reported with liraglutide treatment (43.6% vs 37.1%).
Pharmacokinetic properties
Absorption
The absorption of liraglutide following subcutaneous administration is slow, reaching maximum concentration 8–12 hours post dosing. Estimated maximum liraglutide concentration was 9.4 nmol/l for a subcutaneous single dose of liraglutide 0.6 mg. At 1.8 mg liraglutide, the average steady state concentration of liraglutide (AUCτ/24) reached approximately 34 nmol/l. Liraglutide exposure increased proportionally with dose. The intra-subject coefficient of variation for liraglutide AUC was 11% following single dose administration. Absolute bioavailability of liraglutide following subcutaneous administration is approximately 55%.
Distribution
The apparent volume of distribution after subcutaneous administration is 11–17 l. The mean volume of distribution after intravenous administration of liraglutide is 0.07 l/kg. Liraglutide is extensively bound to plasma proteins (>98%).
Biotransformation
During 24 hours following administration of a single radiolabelled [3H]-liraglutide dose to healthy subjects, the major component in plasma was intact liraglutide. Two minor plasma metabolites were detected (≤9% and ≤5% of total plasma radioactivity exposure). Liraglutide is metabolised in a similar manner to large proteins without a specific organ having been identified as major route of elimination.
Elimination
Following a [3H]-liraglutide dose, intact liraglutide was not detected in urine or faeces. Only a minor part of the administered radioactivity was excreted as liraglutide-related metabolites in urine or faeces (6% and 5%, respectively). The urine and faeces radioactivity was mainly excreted during the first 6–8 days, and corresponded to three minor metabolites, respectively.
The mean clearance following subcutaneous administration of a single dose liraglutide is approximately 1.2 l/h with an elimination half-life of approximately 13 hours.
Special populations
Elderly patients
Age had no clinically relevant effect on the pharmacokinetics of liraglutide based on the results from a pharmacokinetic study in healthy subjects and population pharmacokinetic data analysis of patients (18 to 80 years).
Gender
Gender had no clinically meaningful effect on the pharmacokinetics of liraglutide based on the results of population pharmacokinetic data analysis of male and female patients and a pharmacokinetic study in healthy subjects.
Ethnic origin
Ethnic origin had no clinically relevant effect on the pharmacokinetics of liraglutide based on the results of population pharmacokinetic analysis which included patients of White, Black, Asian and Hispanic groups.
Obesity
Population pharmacokinetic analysis suggests that body mass index (BMI) has no significant effect on the pharmacokinetics of liraglutide.
Hepatic impairment
The pharmacokinetics of liraglutide was evaluated in patients with varying degree of hepatic impairment in a single-dose trial. Liraglutide exposure was decreased by 13–23% in patients with mild to moderate hepatic impairment compared to healthy subjects.
Exposure was significantly lower (44%) in patients with severe hepatic impairment (Child Pugh score >9).
Renal impairment
Liraglutide exposure was reduced in patients with renal impairment compared to individuals with normal renal function. Liraglutide exposure was lowered by 33%, 14%, 27% and 26% in patients with mild (creatinine clearance, CrCl 50–80 ml/min), moderate (CrCl 30–50 ml/min), and severe (CrCl <30 ml/min) renal impairment and in end-stage renal disease requiring dialysis, respectively.
Similarly, in a 26-week clinical trial, patients with type 2 diabetes and moderate renal impairment (CrCL 30–59 ml/min, see section 5.1) had 26% lower liraglutide exposure when compared with a separate trial including patients with type 2 diabetes with normal renal function or mild renal impairment.
Paediatric population
Pharmacokinetic properties were assessed in clinical studies in the paediatric population with type 2 diabetes aged 10 years and above. The liraglutide exposure in adolescents and children was comparable to that observed in the adult population.
Preclinical safety data
Non-clinical data reveal no special hazards for humans based on conventional studies of safety pharmacology, repeat-dose toxicity or genotoxicity.
Non-lethal thyroid C-cell tumours were seen in 2-year carcinogenicity studies in rats and mice. In rats, a no observed adverse effect level (NOAEL) was not observed. These tumours were not seen in monkeys treated for 20 months. These findings in rodents are caused by a non-genotoxic, specific GLP-1 receptor-mediated mechanism to which rodents are particularly sensitive. The relevance for humans is likely to be low but cannot be completely excluded. No other treatment-related tumours have been found.
Animal studies did not indicate direct harmful effects with respect to fertility but slightly increased early embryonic deaths at the highest dose. Dosing with Victoza during mid-gestation caused a reduction in maternal weight and foetal growth with equivocal effects on ribs in rats and skeletal variation in the rabbit. Neonatal growth was reduced in rats while exposed to Victoza, and persisted in the post-weaning period in the high dose group. It is unknown whether the reduced pup growth is caused by reduced pup milk intake due to a direct GLP-1 effect or reduced maternal milk production due to decreased caloric intake.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.