VILTEPSO Solution for injection Ref.[9908] Active ingredients:
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
VILTEPSO is designed to bind to exon 53 of dystrophin pre-mRNA resulting in exclusion of this exon during mRNA processing in patients with genetic mutations that are amenable to exon 53 skipping. Exon 53 skipping is intended to allow for production of an internally truncated dystrophin protein in patients with genetic mutations that are amenable to exon 53 skipping.
12.2. Pharmacodynamics
After treatment with VILTEPSO 80 mg/kg once weekly, all patients evaluated (N=8) were found to produce mRNA for a truncated dystrophin protein, as measured by reverse transcription polymerase chain reaction (RT-PCR), and demonstrated exon 53 skipping, as measured by DNA sequence analysis.
In Study 1, all patients who received VILTEPSO 80 mg/kg once weekly for 20 to 24 weeks showed an increase from baseline in dystrophin protein expression, as quantified by a validated Western blot method (mean 5.3%; median 3.8%; range 0.7% to 13.9% of normal levels when normalized to myosin heavy chain; p-value 0.01). Mass spectrometry, immunofluorescence staining, and RT-PCR results were supportive of the Western blot data [see Clinical Studies (14)]. Expected localization of truncated dystrophin to the sarcolemma in muscle fibers of patients treated with viltolarsen was confirmed by immunofluorescence staining.
12.3. Pharmacokinetics
The pharmacokinetics of viltolarsen was evaluated in DMD patients following administration of intravenous (IV) doses ranging from 1.25 mg/kg/week (0.016 times the recommended dosage) to 80 mg/kg/week (the recommended dosage). Viltolarsen exposure increased proportionally with dose, with minimal accumulation with once-weekly dosing. Inter-subject variability (as %CV) for Cmax and AUC ranged from 16% to 27% respectively.
VILTEPSO is administered as an IV infusion over 60 minutes. Bioavailability is assumed to be 100%, and median Tmax was around 1 hour (end of infusion).
Distribution
The mean viltolarsen steady-state volume of distribution was 300 mL/kg (%CV=14 at a dose of 80 mg/kg. Viltolarsen plasma protein binding ranged from 39% to 40% and is not concentration dependent.
Elimination
Metabolism
Data from in vitro metabolism indicate that viltolarsen is metabolically stable. No metabolites were detected in plasma or urine.
Excretion
VILTEPSO is excreted mainly as an unchanged drug in the urine. Viltolarsen elimination half-life was 2.5 (%CV=8) hours, and plasma clearance was 217 mL/hr/kg (%CV=22).
Specific Populations
Age, Sex & Race
The pharmacokinetics of viltolarsen have been evaluated only in male pediatric DMD patients.There is no experience with VILTEPSO in patients 65 years of age or older. No marked differences in any PK parameters were observed between White and Asian patients.
Patients with Renal or Hepatic Impairment
VILTEPSO has not been studied in patients with renal or hepatic impairment. Viltolarsen was found to be metabolically stable, and hepatic metabolism does not contribute to the elimination of viltolarsen. In addition, viltolarsen was mainly excreted unchanged in the urine. Viltolarsen is eliminated renally, and renal impairment is expected to result in increasing exposure of viltolarsen. However, because of the effect of reduced skeletal muscle mass on creatinine measurements in DMD patients, no specific dosage adjustment can be recommended for DMD patients with renal impairment based on glomerular filtration rate estimated by serum creatinine [see Use in Specific Populations (8.6)].
In Vitro Drug Interaction Studies
Viltolarsen did not inhibit CYP3A4/5, CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, UGT1A1, or UGT2B7. Viltolarsen did not induce CYP1A2, CYP2B6, or CYP3A4.
Viltolarsen is not metabolized by CYP enzymes and is not a substrate of transporters BCRP, BSEP, MDR1, OAT1, OAT3, OCT1, OCT2, MATE1, or MATE2-K. Viltolarsen did not inhibit the transporters tested (OATP1B1, OATP1B3, OAT3, BCRP, MDR1, BSEP, OAT1, OCT1, OCT2, MATE1, and MATE2-K).
Based on in vitro data, viltolarsen has a low potential for drug-drug interactions with major CYP enzymes and drug transporters in humans.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies of viltolarsen have not been conducted.
Mutagenesis
Viltolarsen was negative for genotoxicity in in vitro (bacterial reverse mutation, chromosomal aberration in Chinese hamster lung cells) and in vivo (mouse bone marrow micronucleus) assays.
Impairment of Fertility
Intravenous administration of viltolarsen (0, 60, 240, or 1000 mg/kg) to male mice weekly prior to and during mating to untreated females did not have adverse effects on fertility. Plasma exposure (AUC) at the highest dose was approximately 18 times that in humans at the recommended human dose of 80 mg/kg/week.
14. Clinical Studies
The effect of VILTEPSO on dystrophin production was evaluated in one study in DMD patients with a confirmed mutation of the DMD gene that is amenable to exon 53 skipping (Study 1; NCT02740972).
Study 1 was a multicenter, 2-period, dose-finding study conducted in the United States and Canada.
During the initial period (first 4 weeks) of Study 1, patients were randomized (double blind) to VILTEPSO or placebo. All patients then received 20 weeks of open-label VILTEPSO 40 mg/kg once weekly (0.5 times the recommended dosage) (N=8) or 80 mg/kg once weekly (N=8). Study 1 enrolled ambulatory male patients 4 years to less than 10 years of age (median age 7 years) on a stable corticosteroid regimen for at least 3 months.
Efficacy was assessed based on change from baseline in dystrophin protein level (measured as % of the dystrophin level in healthy subjects, i.e., % of normal) at Week 25. Muscle biopsies (left or right biceps brachii) were collected from patients at baseline and following 24 weeks of VILTEPSO treatment, and analyzed for dystrophin protein level by Western blot normalized to myosin heavy chain (primary endpoint) and mass spectrometry (secondary endpoint).
In patients who received VILTEPSO 80 mg/kg once weekly, mean dystrophin levels increased from 0.6% (SD 0.8) of normal at baseline to 5.9% (SD 4.5) of normal by Week 25, with a mean change in dystrophin of 5.3% (SD 4.5) of normal levels (p=0.01) as assessed by validated Western blot (normalized to myosin heavy chain); the median change from baseline was 3.8%. All patients demonstrated an increase in dystrophin levels over their baseline values. As assessed by mass spectrometry (normalized to filamin C), mean dystrophin levels increased from 0.6% (SD 0.2) of normal at baseline to 4.2% (SD 3.7) of normal by Week 25, with a mean change in dystrophin of 3.7% (SD 3.8) of normal levels (nominal p=0.03, not adjusted for multiple comparisons); the median change from baseline was 1.9%.
Individual patient dystrophin levels in patients evaluated in Study 1 are shown in Figure 2 and Table 2.
Figure 2. Dystrophin Expression in Individual Patients (Study 1):
Patients Treated With VILTEPSO 80 mg/kg/week (n=8)
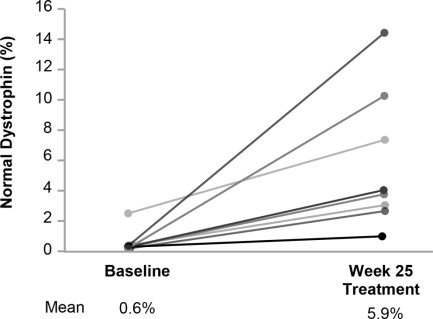
Note: Solid lines represent individual patient data. Dystrophin was measured using Western blot and normalized to myosin heavy chain.
Table 2. Dystrophin Expression in Individual Patients (Study 1):/b>
| Patient Number | Western Blot % Normal Dystrophina | ||
|---|---|---|---|
| Baseline | Week 25 | Change from Baseline | |
| 1 | 0.46 | 1.14 | 0.69 |
| 2 | 0.40 | 3.97 | 3.57 |
| 3 | 0.46 | 2.97 | 2.51 |
| 4 | 0.09 | 10.40 | 10.31 |
| 5 | 0.51 | 14.42 | 13.91 |
| 6 | 2.61 | 7.40 | 4.79 |
| 7 | 0.43 | 3.06 | 2.63 |
| 8 | 0.09 | 4.07 | 3.98 |
a Data were normalized by myosin heavy chain
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.