Source: European Medicines Agency (EU) Revision Year: 2022 Publisher: H. Lundbeck A/S, Ottiliavej 9, 2500 Valby, Denmark
Pharmacotherapeutic group: analgesics, calcitonin gene-related peptide (CGRP) antagonists
ATC code: N02CD05
Eptinezumab is a recombinant humanized immunoglobulin G1 (IgG1) antibody that binds to α- and β-forms of human calcitonin gene-related peptide (CGRP) ligand with low picomolar affinity (4 and 3 pM Kd, respectively). Eptinezumab prevents the activation of the CGRP receptors and hence the downstream cascade of physiological events linked to initiation of migraine attacks.
Eptinezumab inhibits α- and β-CGRP-mediated neurogenic inflammation and vasodilation.
Eptinezumab is highly selective (>100,000-fold vs related neuropeptides amylin, calcitonin, adrenomedullin and intermedin).
VYEPTI (eptinezumab) was evaluated for the preventive treatment of migraine in two pivotal placebo-controlled studies: PROMISE 1 was conducted in patients with episodic migraine (n=888) and PROMISE 2 in patients with chronic migraine (n=1072). Enrolled patients had a history of migraine (with or without aura) of at least 12 months, according to the International Classification of Headache Disorders (ICHD-II or III) diagnostic criteria.
PROMISE 1 was a parallel group, double-blind, placebo-controlled study to evaluate the efficacy and safety of VYEPTI for the preventive treatment of episodic migraine in adults. 665 patients were randomized to receive placebo (N=222), 100 mg eptinezumab (N=221), or 300 mg eptinezumab (N=222) every 12 weeks for 48 weeks (4 infusions). Episodic migraine was defined as ≥4 and ≤14 headache days of which at least 4 had to be migraine days in each 28-day period in the 3 months prior to screening and confirmed during baseline period. Patients were allowed concurrent acute migraine or headache medications, including migraine-specific medications (i.e., triptans, ergotamine derivatives), during the study. Regular use (greater than 7 days per month) of other treatments for the prevention of migraine was not allowed.
The primary efficacy endpoint was the change from baseline in mean monthly migraine days (MMD) over weeks 1-12. The key secondary endpoints included ≥50% and ≥75% migraine responder rates defined as the proportion of patients achieving at least the specified percent reduction in migraine days over weeks 1-12, ≥75% migraine responder rate over weeks 1-4, and the percentage of patients with a migraine on the day after the first dosing (day 1).
Patients had a mean age of 40 years (range: 18 to 71 years), 84% were women, and 84% were white. At baseline the mean number of migraine days per month at baseline was 8.6 and the rate of patients with a migraine on a given day was 31%; both were similar across treatment groups.
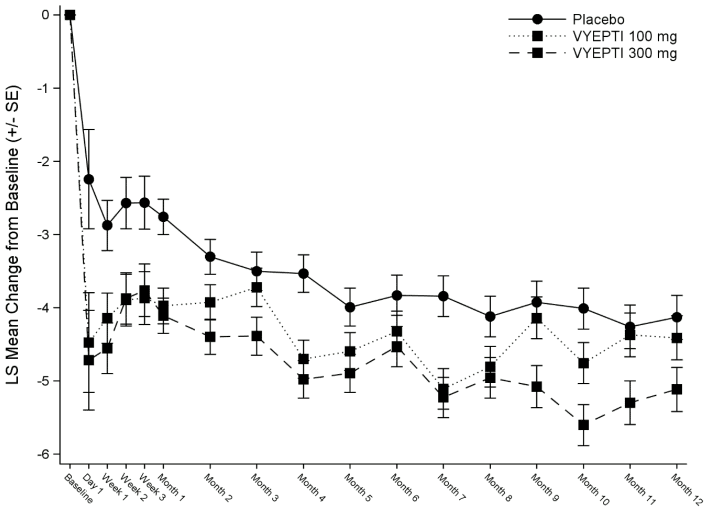
Reduction in mean monthly migraine days from placebo for both doses was observed from the first day after administration.
Figure 1. Mean changes from baseline of monthly migraine days in PROMISE 1:
LS = least square; VYEPTI = eptinezumab
At each timepoint, an ANCOVA including treatment and prophylactic medication use as factors and baseline migraine days as a continuous covariate was used to estimate the mean change from baseline.
Table 2. Primary and key secondary efficacy endpoint results in PROMISE 1 (episodic migraine):
| VYEPTI 100 mg N=221 | VYEPTI 300 mg N=222 | Placebo N=222 | |
|---|---|---|---|
| Monthly migraine days (MMD) – Weeks 1-12 | |||
| Baseline | 8.7 | 8.6 | 8.4 |
| Mean change | -3.9 | -4.3 | -3.2 |
| Difference from placebo | -0.7 | -1.1 | |
| CI95% | (-1.3, -0.1) | (-1.7, -0.5) | |
| p-value vs placebo | 0.0182 | 0.0001 | |
| ≥75% MMD responders – Weeks 1-12 | |||
| Responders | 30.8% | 31.5% | 20.3% |
| Difference from placebo | 10.5% | 11.3% | |
| p-value vs placebo | 0.0112 | 0.0066 | |
| ≥75% MMD responders – Weeks 1-12 | |||
| Responders | 22.2% | 29.7% | 16.2% |
| Difference from placebo | 6.0% | 13.5% | |
| p-value vs placebo | 0.1126 | 0.0007 | |
| ≥50% MMD responders – Weeks 1-12 | |||
| Responders | 49.8% | 56.3% | 37.4% |
| Difference from placebo | 12.4% | 18.9% | |
| p-value vs placebo | 0.0085 | 0.0001 | |
PROMISE 2 was a parallel group, double-blind, placebo-controlled global study to evaluate the efficacy and safety of VYEPTI for the preventive treatment of chronic migraine in adults. A total of 1,072 patients were randomized and received placebo (N=366), 100 mg eptinezumab (N=356), or 300 mg eptinezumab (N=350) every 12 weeks for 24 weeks (2 infusions). Chronic migraine was defined as ≥15 to ≤26 headache days, of which ≥8 were assessed as migraine days in the 3 months prior to screening and confirmed during the 28-day screening period. During the study, patients were allowed acute or preventive medication for migraine or headache on an established stable regimen (except for onabotulinumtoxinA).
A total of 431 patients (40%) with a dual diagnosis of chronic migraine and medication overuse headache (associated with the overuse of triptans, ergotamine, or combination analgesics >10 days/month, or acetaminophen, acetylsalicylic acid, or non-steroidal anti-inflammatory drugs ≥15 days/month) confirmed during screening period were included in the study population.
The primary efficacy endpoint was the change from baseline in mean MMD over weeks 1-12. The key secondary endpoints included ≥50% and ≥75% migraine responder rates defined as the proportion of patients achieving the specified percent reduction in migraine days over weeks 1-12, ≥75% migraine responder rate over weeks 1-4, the percentage of patients with a migraine on the day after dosing, the reduction in migraine prevalence from baseline to week 4, the change from baseline in the total score on the Headache Impact Test (HIT-6) at week 12 (300 mg dose only), and the change from baseline in acute monthly migraine medication days, mean over weeks 1-12 (300 mg dose only). Patients had a mean age of 41 years (range: 18 to 65 years), 88% were women, and 91% were white. Forty-one percent of patients were taking concomitant preventive medication for migraine. At baseline the mean number of migraine days per month at baseline was 16.1 and the rate of patients with a migraine on a given day was 57.6%; both were similar across treatment groups.
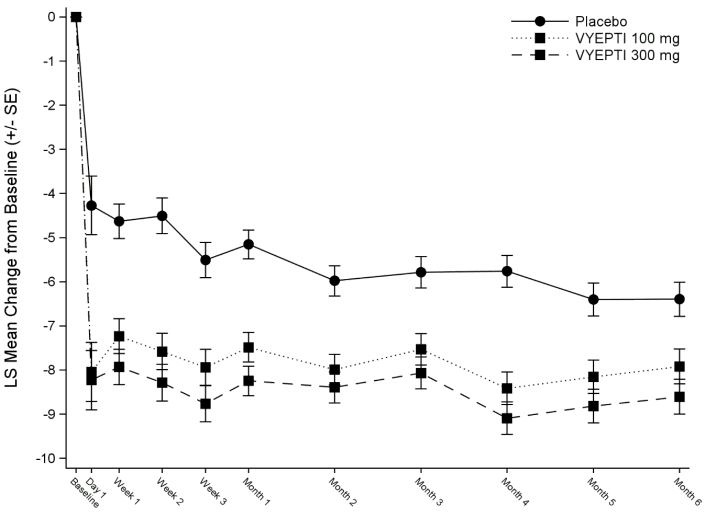
Reduction in mean monthly migraine days from placebo for both doses was observed from the first day after administration.
<bFigure 2. Mean changes from baseline of monthly migraine days in PROMISE 2:
LS = least square; VYEPTI = eptinezumab
At each timepoint, an ANCOVA including treatment as a factor and baseline migraine days as a continuous covariate was used to estimate the mean change from baseline.
Table 3. Primary and key secondary efficacy endpoint results in PROMISE 2 (chronic migraine):
| VYEPTI 100 mg N=356 | VYEPTI 300 mg N=350 | Placebo N=366 | |
|---|---|---|---|
| Monthly migraine days (MMD) – Weeks 1-12 | |||
| Baseline | 16.1 | 16.1 | 16.2 |
| Mean change | -7.7 | -8.2 | -5.6 |
| Difference from placebo | -2.0 | -2.6 | |
| CI95% | (-2.9, -1.2) | (-3.5, -1.7) | |
| p-value vs placebo | <0.0001 | <0.0001 | |
| ≥75% MMD responders – Weeks 1-4 | |||
| Responders | 30.9% | 36.9% | 15.6% |
| Difference from placebo | 15.3% | 21.3% | |
| p-value vs placebo | <0.0001 | <0.0001 | |
| ≥75% MMD responders – Weeks 1-12 | |||
| Responders | 26.7% | 33.1% | 15.0% |
| Difference from placebo | 11.7% | 18.1% | |
| p-value vs placebo | 0.0001 | <0.0001 | |
| ≥50% MMD responders – Weeks 1-12 | |||
| Responders | 57.6% | 61.4% | 39.3% |
| Difference from placebo | 18.2% | 22.1% | |
| p-value vs placebo | <0.0001 | <0.0001 | |
| HIT-6 score – Week 12a | |||
| Baseline | 65.0 | 65.1 | 64.8 |
| Mean change | -6.2 | -7.3 | -4.5 |
| Difference from placebo | -1.7 | -2.9 | |
| CI95% | (-2.8, -0.7) | (-3.9, -1.8) | |
| p-value vs placebo | 0.0010 | <0.0001 | |
| Days per month with acute medication use – Weeks 1-12a,b | |||
| Baseline | 6.6 | 6.7 | 6.2 |
| Mean change | -3.3 | -3.5 | -1.9 |
| Difference from placebo | -1.2 | -1.4 | |
| CI95% | (-1.7., -0.7) | (-1.9., -0.9) | |
| p-value vs placebo | <0.0001 | <0.0001 | |
In the 431 (40%) patients diagnosed with medication-overuse headache (MOH) in PROMISE-2, the mean change from baseline in MMD (weeks 1-12) was for VYEPTI 100 mg -8.4 days, VYEPTI 300 mg -8.6 days, and placebo -5.4 days (mean difference to placebo of -3.0 days and -3.2 days for 100 mg and 300 mg, respectively).
VYEPTI 300 mg was administered every 12 weeks by IV infusion for up to 96 weeks in 128 patients with chronic migraine. The primary objective was to evaluate the long-term safety following repeated doses of VYEPTI. Secondary objectives included characterization of the PK and immunogenicity profiles for VYEPTI (section 4.8) and evaluation of the therapeutic effect of VYEPTI on several patient reported outcomes relating to migraine and quality of life including the Headache Impact Test (HIT-6). Patients had a mean age of 41.5 years (range: 18 to 65 years), 85% were women, 95% were white, and 36% took concomitant preventive medication for migraine. The mean number of migraine days per 28-day period in the 3 months preceding screening was 14.1 days. In total, 100 patients (78.1%) completed the study (week 104). Patients were severely impacted at baseline with a mean total HIT-6 of 65. The mean change from baseline through week 104 was -9.7 (p<0.0001). The safety profile was consistent with the safety profiles observed in the randomized, placebo-controlled studies, and a sustained effect on patient-relevant outcomes was observed for up to 96 weeks.
The European Medicines Agency has deferred the obligation to submit the results of studies with VYEPTI in one or more subset of the paediatric population in the preventive treatment of migraine (see section 4.2 for information on paediatric use).
As VYEPTI is administered intravenously, it is 100% bioavailable. Eptinezumab exhibits linear pharmacokinetics and exposure increases proportionally with doses from 10 to 1000 mg. Steady-state is attained after the first-dose during a once every 12 weeks dosing schedule. Median time to maximum concentration (Cmax) is 30 minutes (end-of-infusion), and the average terminal elimination half-life is 27 days. The mean accumulation ratios based on Cmax and AUC0-tau are 1.08 and 1.15, respectively.
VYEPTI is administered by intravenous infusion which bypasses extravascular absorption and is 100% bioavailable. Median time to peak concentration was attained at the end of infusion (30 minutes).
The central volume of distribution (Vc) for eptinezumab was approximately 3.7 litres.
Eptinezumab is expected to be degraded by proteolytic enzymes into small peptides and amino acids.
Eptinezumab apparent clearance was 0.15 L/day, and the terminal elimination half-life was approximately 27 days.
A population pharmacokinetic analysis including 2 123 subjects explored the effect of age, gender, ethnicity and body weight on the pharmacokinetics of eptinezumab. Relative to a 70 kg subject, steady state exposure of eptinezumab in a 190 kg subject was up to 52% lower, whereas is would be up to 50% higher in a 39 kg subject. However, from the exposure-response evaluation, there was no effect of body weight on the clinical efficacy. No dose adjustment is required based on body weight. The pharmacokinetics of eptinezumab were not affected by age (18-71), gender or race based on population pharmacokinetics. Therefore, no dose adjustment is needed.
No dedicated hepatic or renal impairment studies were conducted to assess the effects of hepatic and renal impairment upon the pharmacokinetics of eptinezumab. Population pharmacokinetic analysis of integrated data from the VYEPTI clinical studies did not reveal any differences in patients with renal or hepatic impairment that would require dose adjustment. No data for patients with severe renal impairment are available.
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated-dose toxicity, juvenile toxicity, or toxicity to reproduction and development.
As eptinezumab is unlikely to interact directly with DNA or other chromosomal material, evaluations for potential genotoxicity were considered unnecessary and not performed.
As no carcinogenicity risk has been identified by extensive evaluation of the literature related to inhibition of CGRP and as no eptinezumab-related proliferative findings were observed in long term studies in monkeys, carcinogenicity testing was considered unnecessary and not performed.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.