WAYLIVRA Solution for injection Ref.[11028] Active ingredients: Volanesorsen
Source: European Medicines Agency (EU) Revision Year: 2022 Publisher: Akcea Therapeutics Ireland Ltd., St. James House, 72 Adelaide Road, Dublin 2, D02 Y017, Ireland
5.1. Pharmacodynamic properties
Pharmacotherapeutic group: lipid modifying agents, other lipid modifying agents
ATC code: C10AX18
Mechanism of action
Volanesorsen is an antisense oligonucleotide designed to inhibit the formation of apoC-III, a protein that is recognised to regulate both triglyceride metabolism and hepatic clearance of chylomicrons and other triglyceride-rich lipoproteins. The selective binding of volanesorsen to the apoC-III messenger ribonucleic acid (mRNA) within the 3′ untranslated region at base position 489-508 causes the degradation of the mRNA. This binding prevents translation of the protein apoC-III, thus removing an inhibitor of triglyceride clearance and enabling metabolism through an LPL-independent pathway.
Pharmacodynamic effects
Effects of Waylivra on lipid parameters
In APPROACH, the Phase 3 clinical study in patients with FCS, Waylivra reduced fasting triglycerides, total cholesterol, non-HDL cholesterol, apoC-III, apoB-48, and chylomicron triglyceride levels and increased LDL-C, HDL-C, and apoB (see Table 3).
Table 3. Mean baseline and percent change in lipid parameters from baseline to month 3:
| Lipid Parameter (g/L for apoC-III, apoB, apoB-48; mmol/L for cholesterol, triglycerides) | Placebo (N=33) | Volanesorsen 285 mg (N=33) | ||
|---|---|---|---|---|
| Baseline | % Change | Baseline | % Change | |
| Triglycerides | 24,3 | +24% | 25,6 | -72% |
| Total Cholesterol | 7,3 | +13% | 7,6 | -39% |
| LDL-C | 0,72 | +7% | 0,73 | +139% |
| HDL-C | 0,43 | +5% | 0,44 | +45% |
| Non-HDL-C | 6,9 | +14% | 7,1 | -45% |
| ApoC-III | 0,29 | +6% | 0,31 | -84% |
| ApoB | 0,69 | +2% | 0,65 | +20% |
| ApoB-48 | 0,09 | +16% | 0,11 | -75% |
| Chylomicron Triglycerides | 20 | +38% | 22 | -77% |
Cardiac Electrophysiology
At a drug concentration 4.1 times the peak drug plasma concentrations (Cmax) of the maximum recommended dose (285 mg subcutaneous injection), volanesorsen did not prolong the heart-rate corrected QT (QTc) interval.
Clinical efficacy and safety
APPROACH study in patients with FCS
The APPROACH study is a randomised, double-blind placebo-controlled 52-week multicentre clinical study in 66 patients with FCS, evaluating volanesorsen 285 mg administered as a subcutaneous injection (33 treated with volanesorsen, 33 with placebo). Main inclusion criteria were a diagnosis of FCS (Type 1 hyperlipoproteinemia) in combination with a history of chylomicronemia evidenced by documentation of lactescent serum or documentation of fasting TG measurement ≥880 mg/dl.
Diagnosis of FCS required documentation of at least one of the following:
a) Confirmed homozygote, compound heterozygote, or double heterozygote for known loss-offunction mutations in Type 1-causing genes (such as LPL, APOC2, GPIHBP1, or LMF1)
b) Post heparin plasma LPL activity of ≤20% of normal. Patients taking Glybera within 2 years prior to screening were excluded from the study.
Nineteen of the 33 patients in the volanesorsen group completed 12 months of study treatment. Thirteen of these patients had dose adjustment/pause on the study. Out of the 13, 5 had a dose pause, 5 had a dose adjustment and 3 had both a dose pause and dose adjustment.
Mean age was 46 years (range 20-75 years; 5 patients ≥65 years old); 45% were men; 80% were White, 17% were Asian, and 3% were of other races. Mean body mass index was 25 kg/m². A history of documented acute pancreatitis was reported for 76% of patients and a history of diabetes was reported for 15% of patients; 21% of patients had a recorded history of lipaemia retinalis and 23% of patients had a recorded history of eruptive xanthomas. The median age at diagnosis was 27 years, with 23% shown to lack a known FCS genetic mutation.
At study entry, 55% of patients were on lipid lowering therapies (48% on fibrates, 29% on fish oils, 20% HMG-CoA reductase inhibitors), 27% were on pain medications, 20% were on platelet aggregation inhibitors, and 14% were on nutritional supplements. Background lipid-lowering therapies remained consistent throughout the study. Patients were prohibited from receiving plasma apheresis within 4 weeks prior to screening or during the study; 11% of patients had previously received gene therapy for lipoprotein lipase deficiency (i.e., alipogene tiparvovec), on average 8 years prior to starting this study. After a 6-week diet run-in period, the mean fasting triglyceride level at baseline was 2,209 mg/dL (25.0 mmol/L). Compliance with diet and alcohol restriction was reinforced through periodic counselling sessions during the study.
Waylivra led to a statistically significant reduction in triglyceride levels as compared to placebo at the primary efficacy endpoint, defined as percent change from baseline to Month 3 in fasting triglycerides, in addition to a lower incidence of pancreatitis over the 52-week treatment period in a post-hoc analysis (Table 4).
At the primary efficacy endpoint, the treatment difference between volanesorsen and placebo in mean fasting triglyceride percent change was -94% (95% CI: -122% -67%; p˂0.0001, with a decrease of - 77% from baseline (95% CI: -97, -56) in patients receiving volanesorsen and an increase of 18% from baseline (95% CI: -4, 39) in patients receiving placebo (Table 4).
Table 4. Mean change from baseline in fasting triglycerides in the phase 3 placebo-controlled study in patients with FCS at month 3 (APPROACH):
| Placebo (N=33) | Volanesorsen 285 mg (N=33) | Relative Difference in Change vs Placebo | |
|---|---|---|---|
| LS mean percent change (95% CI) | +18% (-4, 39) | -77% (-97, -56) | -94%* (-122, -67) |
| LS mean absolute change (95% CI) mg/dL or mmol/L | +92 (-301, +486) mg/dl +1 (-3, +5) mmol/l | -1.712 (-2.094, -1.330) mg/dl -19 (-24, -15) mmol/l | -1.804 (-2.306, -1.302) mg/dl -20 (-26, -15) mmol/l |
* p-value <0.0001 (primary efficacy endpoint)
Difference= LS Mean of [volanesorsen % Change – Placebo % Change] (ANCOVA model)
Onset of the reduction was rapid with separation from placebo seen as early as 4 weeks and maximum response seen at 12 weeks, with clinically and statistically significant triglyceride reduction maintained over 52 weeks (Figure 1). The mean fasting triglyceride percent change was significantly different between volanesorsen and placebo arms at 3, 6, and 12 months; the volanesorsen arm included patients who did not complete dosing but who returned for assessments over the 52-week study. There were no significant differences in treatment effect across the stratification factors of presence or absence of concurrent omega-3 fatty acids or fibrates.
Figure 1. LS mean percent change in fasting triglycerides in phase 3 study in patients with FCS (APPROACH):
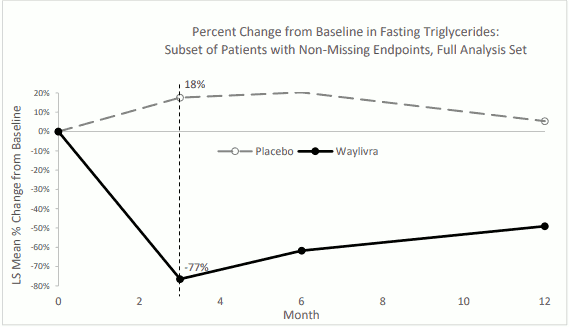
LS mean percent change from baseline in fasting triglycerides based on the observed data are displayed.
Difference = LS Mean of [volanesorsen % Change – Placebo % Change] (ANCOVA model)
p-value from ANCOVA model <0.0001 at Month 3 (primary efficacy endpoint), Month 6 and Month 12
Additional efficacy results for changes in triglyceride are presented in Table 5. Most patients receiving volanesorsen experienced a clinically significant reduction in triglycerides.
Table 5. Additional results for changes in triglycerides in the APPROACH study (primary endpoint at month 3):
| Parameter at month 3a | Placebo (N=31) | Volanesorsen 285 mg (N=30) |
|---|---|---|
| Percent of patientsb with fasting plasma triglyceride <750 mg/dL (8.5 mmol/L)* | 10% | 77% |
| Percent of patientsc with ≥40% reduction in fasting triglycerides** | 9% | 88% |
a The month 3 endpoint was defined as the average of week 12 (Day 78) and Week 13 (Day 85) fasting assessments. If 1 visit was missing, then the other visit was used as the endpoint.
b The denominator for percentage calculation was the total number of patients in FAS with baseline fasting triglyceride ≥750 mg/dL (or 8.5 mmol/L) in each treatment group.
c The denominator for percentage calculation was the total number of patients in each treatment group.
* p-value =0.0001
** p-value <0.0001
P-values from logistic regression model with treatment, presence of pancreatitis and presence of concurrent omega-3 fatty acids and/or fibrates as factors, and logarithm-transformed baseline fasting triglycerides as a covariate.
In the APPROACH study, the numerical incidence of pancreatitis in patients treated with volanesorsen was lower compared with placebo (3 patients 4 events in 33 placebo patients vs 1 patient 1 event in 33 volanesorsen patients).
An analysis of patients with a history of recurrent pancreatitis events (≥2 events in the 5 years prior to Study Day 1) showed a significant reduction in pancreatitis attacks in volanesorsen-treated patients compared to placebo treated patients (p=0.0242). In the volanesorsen group, of the 7 patients who had 24 adjudicated pancreatitis attacks in the prior 5 years, none of the patients experienced a pancreatitis attack during the 52 week treatment period. In the placebo group, of the 4 patients who had 17 adjudicated pancreatitis attacks in the prior 5 years, 3 patients experienced 4 pancreatitis attacks during the 52-week treatment period.
Open-label extension study in patients with FCS
CS7 is a multicentre, open-label extension Phase 3 study designed to evaluate the safety and efficacy of dosing and extended dosing with volanesorsen in patients with FCS. All patients enrolled either had participated in the APPROACH Study, in the CS16 Study, or were new FCS patients and had completed qualification assessments prior to receiving volanesorsen 285 mg once per week or a reduced frequency for safety or tolerability reasons determined in their index study. A total of 68 patients have been treated in this study including 51 treatment-naïve patients, 14 patients who had received volanesorsen in Study CS6, and 3 patients who had received volanesorsen in Study CS16. Fifty patients had a dose pause, 45 had a dose adjustment and 41 had both a dose pause and a dose adjustment.
Data from Study CS7 is provided in Table 6. The percent change in fasting TG from Index Study Baseline to Open-label Month 3 for the APPROACH- and CS16-volanesorsen patients was -49.2% and -64.9%, respectively. The percent change in fasting TG from index study baseline to open-label month 6, month 12 and month 24 for the APPROACH-volanesorsen patients was -54.8%, -35.1% and -50.2%, respectively.
Table 6. Summary of fasting triglycerides (mean (SD, SEM), mg/dL) over time in study CS7 (N=68):
| Time point | Treatment-naïve group (open-label study baselinea, N=51) | APPROACH-volanesorsen (index study baselinea, N=14) | CS16-volanesorsen (index study baselinea, N=3) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Observed value | % change from baseline | n | Observed value | % change from baseline | n | Observed value | % change from baseline | |
| Baselinea | 51 | 2341 (1193, 167) | - | 14 | 2641 (1228, 328) | - | 3 | 2288 (1524, 880) | - |
| Month 3 | 47 | 804 (564, 82) | -59.8 (37.0, 5.4) | 14 | 1266 (812, 217) | -49.2 (34.8, 9.3) | 3 | 855 (651, 376) | -64.9 (9.1, 5.3) |
| Month 6 | 49 | 1032 (695, 99) | -45.5 (42.9, 6.1) | 13 | 1248 (927, 257) | -54.8 (23.8, 6.6) | 3 | 1215 (610, 352) | -43.0 (19.7, 11.4) |
| Month 12 | 45 | 1332 (962, 143) | -36.3 (44.2, 6.6) | 12 | 1670 (1198, 346) | -35.1 (45.6, 13.2) | 3 | 1351 (929, 536) | -41.6 (36.3, 21.0) |
| Month 15 | 34 | 1328 (976, 167) | -35.6 (48.1, 8.2) | 10 | 1886 (1219, 386) | -26.5 (57.4, 18.1) | 2 | 1422 (190, 135) | 3.4 (23.3, 16.5) |
| Month 18 | 27 | 1367 (938, 181) | -37.5 (45.6, 8.8) | 7 | 1713 (1122, 424) | -38.4 (32.2, 12.2) | 2 | 1170 (843, 596) | -24.0 (31.9, 22.6) |
| Month 24 | 21 | 1331 (873, 190) | -40.5 (47.4, 10.3) | 5 | 1826 (1743, 780) | -50.2 (32.2, 14.4) | 2 | 1198 (1177, 832) | -26.3 (56.0, 39.6) |
a Baseline values for treatment-naïve group were taken from the open-label study CS7 and baseline for APPROACH-volanesorsen and CS16-volanesorsen groups were taken from the respective index study.
Elderly population
Clinical studies included 4 patients with FCS aged 65 treated with volanesorsen in randomised control studies (phase II study CS2, 1 patient; APPROACH 3 patients), and 6 patients aged 65 and over in the open-label extension study (CS7). No overall differences in safety or effectiveness were observed between these patients and younger patients, however data are limited in this subpopulation.
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies with volanesorsen in one or more subsets of the paediatric population in the treatment of familial chylomicronemia syndrome (see section 4.2 for information on paediatric use).
This medicinal product has been authorised under a so-called 'conditional approval' scheme. This means that further evidence on this medicinal product is awaited. The European Medicines Agency will review new information on this medicinal product at least every year and this SmPC will be updated as necessary.
5.2. Pharmacokinetic properties
Absorption
Following subcutaneous injection, peak plasma concentrations of volanesorsen are typically reached in 2 to 4 hours. The absolute bioavailability of volanesorsen following a single subcutaneous administration is approximately 80% (most likely higher because an AUC of 0 to 24 hours was used and volanesorsen has a half-life of >2 weeks).
Following a dose of 285 mg once weekly in patients with FCS, the estimated geometric mean (coefficient of variation % of geometric mean) steady-state Cmax is 8.92 µg/ml (35%), AUC0-168h is 136 µg*h/ml (38%), and Ctrough is 127 ng/ml (58%) in patients who remain negative for anti-drug antibody. An alternative dosing regimen of 285 mg volanesorsen every two weeks results in a Ctrough,ss of approximately 58.0 ng/ml with Cmax and AUC similar compared to the once weekly dosing regimen.
Distribution
Volanesorsen was rapidly and widely distributed to tissues following subcutaneous or intravenous administration in all species evaluated. The estimated steady-state volume of distribution (Vss) in patients with FCS is 330 L. Volanesorsen is highly bound to human plasma proteins (>98%) and the binding is concentration independent.
In vitro studies show that volanesorsen is not a substrate or inhibitor of P-glycoprotein (P-gp), breast cancer resistance protein (BCRP), organic anion transporting polypeptides (OATP1B1, OATP1B3), bile salt export pump (BSEP), organic cation transporters (OCT1, OCT2), or organic anion transporters (OAT1, OAT3).
Biotransformation
Volanesorsen is not a substrate for CYP metabolism, and is metabolised in tissues by endonucleases to form shorter oligonucleotides that are then substrates for additional metabolism by exonucleases. Unchanged volanesorsen is the predominant circulating component.
In vitro studies indicate that volanesorsen is not an inhibitor of CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, or CYP3A4 or inducer of CYP1A2, CYP2B6, or CYP3A4.
Elimination
Elimination involves both metabolism in tissues and excretion in urine. Urinary recovery of the parent drug was limited in humans with <3% of administered subcutaneous dose recovered within 24 hours post dose. The parent drug and 5- to 7-mer chain-shortened metabolites accounted for approximately 26% and 55% of oligonucleotides recovered in urine, respectively. Following subcutaneous administration, terminal elimination half-life is approximately 2 to 5 weeks.
In animals, elimination of volanesorsen was slow and occurred mainly via urinary excretion, reflecting rapid plasma clearance principally to tissues. Both volanesorsen and shorter oligonucleotide metabolites (predominantly 7-mer metabolites (generated either from 3′-deletions or 5′-deletions)) were identified in human urine.
Linearity / non-linearity
Single- and multiple-dose pharmacokinetics of volanesorsen in healthy volunteers and patients with hypertriglyceridemia have shown that the Cmax of volanesorsen is dose-proportional over a dose range of 100 to 400 mg and the AUC is slightly more than dose-proportional over the same dose range. Steady-state was reached approximately 3 months after starting volanesorsen. Accumulation in Ctrough was observed (7- to 14-fold) and little or no increase in Cmax or AUC was observed following weekly SC administration over a dose of 200 to 400 mg. Some accumulation in AUC and Cmax was observed for the 50 to 100 mg dose. Since the administered dose will be 285 mg every two weeks, or 142.5 mg weekly, little increase in Cmax or AUC is expected upon multiple dosing in the clinical setting.
Special Populations
Renal impairment
A population pharmacokinetic analysis suggests that mild and moderate renal impairment has no clinically relevant effect on the systemic exposure of volanesorsen. No data are available in patients with severe renal impairment.
Hepatic impairment
The pharmacokinetics of volanesorsen in patients with hepatic impairment is unknown.
Age, sex, weight, and race
Based on the population pharmacokinetic analysis, age, body weight, sex, or race has no clinically relevant effect on volanesorsen exposure. There are limited data available in subjects >75 years of age.
Anti-volanesorsen antibody formation affecting pharmacokinetics
The formation of binding antibodies to volanesorsen appeared to increase total Ctrough by 2- to 19-fold.
5.3. Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity, carcinogenicity or toxicity to reproduction and development.
Dose and time-dependent reductions in platelet counts were observed in Cynomolgus monkey repeated dose studies. The decrease was gradual, self-sustaining and did not decrease to adverse levels. In individual monkeys, severe thrombocytopenia was noted in the 9 month study of drug treated groups at clinically relevant exposures and has also been observed in clinical studies. The decrease in platelet counts was not acute and decreased to below 50,000 cells/μl. Platelet counts recovered after cessation of treatment, but decreased again below 50,000 cells/μl after treatment was resumed in some monkeys. Decreased platelet counts were also observed in rodent repeated dose studies. A mode of action for the observed thrombocytopenia is currently not known.
In nonclinical studies, levels of volanesorsen in milk were very low in lactating mice. The concentrations in breast milk of mice were >800 fold lower than effective tissue concentrations in maternal liver. Due to the poor oral bioavailability of volanesorsen, it is considered unlikely that these low milk concentrations would result in systemic exposure from nursing (see section 4.6).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.