XOFIGO Solution for injection Ref.[9648] Active ingredients: Radium-223 dichloride
Source: European Medicines Agency (EU) Revision Year: 2020 Publisher: Bayer AG, 51368, Leverkusen, Germany
Pharmacodynamic properties
Pharmacotherapeutic group: Therapeutic radiopharmaceuticals, other therapeutic radiopharmaceuticals, various therapeutic radiopharmaceuticals
ATC code: V10XX03
Mechanism of action
Xofigo is a therapeutic alpha particle-emitting pharmaceutical.
Its active moiety radium-223 (as radium-223 dichloride) mimics calcium and selectively targets bone, specifically areas of bone metastases, by forming complexes with the bone mineral hydroxyapatite. The high linear energy transfer of alpha emitters (80 keV/µm) leads to a high frequency of double-strand DNA breaks in adjacent tumour cells, resulting in a potent cytotoxic effect. Additional effects on the tumour microenvironment including osteoblasts and osteoclasts also contribute to the in vivo efficacy. The alpha particle range from radium-223 is less than 100 µm (less than 10 cell diameters) which minimises damage to the surrounding normal tissue.
Pharmacodynamic effects
Compared with placebo, there was a significant difference in favour of Xofigo for all five serum biomarkers for bone turnover studied in a phase II randomised study (bone formation markers: bone alkaline phosphatase [ALP], total ALP and procollagen I N propeptide [PINP], bone resorption markers: C-terminal crosslinking telopeptide of type I collagen/serum C-terminal crosslinked telopeptide of type I collagen [S-CTX-I] and type I collagen crosslinked C-telopeptide [ICTP]).
Cardiac electrophysiology/QT prolongation
No significant QTc prolonging effects were observed after intravenous injection of Xofigo in comparison with placebo in a subgroup of 29 patients in the phase III study (ALSYMPCA).
Clinical efficacy and safety
The clinical safety and efficacy of Xofigo have been evaluated in a double-blind, randomised, multiple dose, phase III, multicentre study (ALSYMPCA; EudraCT 2007-006195-1)) in castration-resistant prostate cancer patients with symptomatic bone metastases. Patients with visceral metastases and malignant lymphadenopathy exceeding 3 cm were excluded. The primary efficacy endpoint was overall survival. Main secondary endpoints included time to symptomatic skeletal events (SSE), time to progression of total alkaline phosphatase (ALP), time to progression of prostate specific antigen (PSA), response of total ALP and normalisation of total ALP.
At the cut-off date of the pre-planned interim analysis (confirmatory analysis), a total of 809 patients were randomised 2:1 to receive Xofigo 55 kBq/kg intravenously every 4 weeks for 6 cycles (N=541) plus best standard of care, or matching placebo plus best standard of care (N=268). Best standard of care included e.g. local external beam radiotherapy, bisphosphonates, corticosteroids, antiandrogens, oestrogens, estramustine or ketoconazole.
An updated descriptive analysis of safety and of overall survival was performed in 921 randomised patients prior to implementing crossover (i.e. offering patients in the placebo group to receive Xofigo treatment).
Demographic and baseline disease characteristics (interim analysis population) were similar between the Xofigo and placebo groups and are shown below for Xofigo:
- the mean age of patients was 70 years (range 49 to 90 years).
- 87% of patients enrolled had an ECOG performance status score of 0-1.
- 41% received bisphosphonates.
- 42% of patients did not receive prior docetaxel because they were deemed ineligible or refused to receive docetaxel.
- 46% of patients had no pain or WHO scale 1 (asymptomatic or mildly symptomatic) and 54% had pain WHO scale 2-3.
- 16% of patients had <6 bone metastases, 44% of patients had between 6 and 20 bone metastases, 40% of patients had more than 20 bone metastases or superscan.
During the treatment period, 83% of patients received luteinising hormone-releasing hormone (LHRH) agonists and 21% of patients received anti-androgens concomitantly.
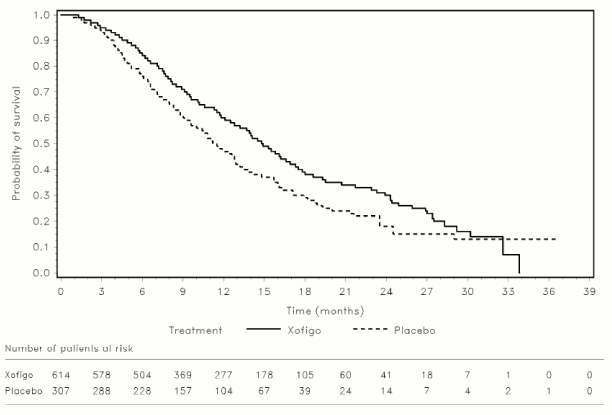
The results of both the interim and updated analysis revealed that overall survival was significantly longer in patients treated with Xofigo plus best standard of care compared to patients treated with placebo plus best standard of care (see Table 2 and Figure 2). A higher rate of non-prostate cancer related deaths was observed in the placebo group (26/541, 4.8% in the Xofigo arm compared to 23/268, 8.6% in the placebo arm).
Table 2. Survival results from the phase III ALSYMPCA study:
| Xofigo | Placebo | |
|---|---|---|
| Interim analysis | N=541 | N=268 |
| Number (%) of deaths | 191 (35.3%) | 123 (45.9%) |
| Median overall survival (months) (95% CI) | 14.0 (12.1–15.8) | 11.2 (9.0–13.2) |
| Hazard ratiob (95% CI) | 0.695 (0.552–0.875) | |
| p-valuea (2-sided) | 0.00185 | |
| Updated analysis | N=614 | N=307 |
| Number (%) of deaths | 333 (54.2%) | 195 (63.5%) |
| Median overall survival (months) (95% CI) | 14.9 (13.9–16.1) | 11.3 (10.4–12.8) |
| Hazard ratiob (95% CI) | 0.695 (0.581–0.832) | |
CI = confidence interval
a The Phase 3 study ALSYMPCA was stopped for efficacy after the interim analysis. As the updated analysis is provided for descriptive purposes only, a p-value is not provided.
b Hazard ratio (Xofigo over placebo) <1 favours Xofigo.
Figure 2. Kaplan-Meier overall survival curves (updated analysis):
The results of the interim analysis and the updated analysis also showed a significant improvement in all main secondary endpoints in the Xofigo arm compared to the placebo arm (see Table 3). Time to event data on ALP progression were supported by statistically significant advantage with respect to ALP normalisation and ALP responses at week 12.
Table 3. Secondary efficacy endpoints from the phase III ALSYMPCA study (interim analysis):
| Incidence | Time-to-event analysis (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|
| [no. (%) of patients] | [median no. of months] | Hazard ratio | p-value | |||||
| Xofigo N=541 | Placebo N=268 | Xofigo N=541 | Placebo N=268 | <1 favours Xofigo | ||||
| Symptomatic skeletal event (SSE) | SSE composite endpoint a | 132 (24.4%) | 82 (30.6%) | 13.5 (12.2–19.6) | 8.4 (7.2–ΝΕ)b | 0.610 (0.461–0.807) | 0.00046 | |
| SSE components | External beam radiation for pain relief | 122 (22.6%) | 72 (26.9%) | 17.0 (12.9–ΝΕ) | 10.8 (7.9–ΝΕ) | 0.649 (0.483–0.871) | 0.00375 | |
| Spinal cord compression | 17 (3.1%) | 16 (6.0%) | ΝΕ | ΝΕ | 0.443 (0.223–0.877) | 0.01647 | ||
| Surgical intervention | 9 (1.7%) | 5 (1.9%) | ΝΕ | ΝΕ | 0.801 (0.267–2.398) | 0.69041 | ||
| Bone fractures | 20 (3.7%) | 18 (6.7%) | ΝΕ | ΝΕ | 0.450 (0.236–0.856) | 0.01255 | ||
| Total ALP progressionc | 79 (14.6%) | 116 (43.3%) | ΝΕ | 3.7 (3.5–4.1) | 0.162 (0.120–0.220) | <0.00001 | ||
| PSA progressiond | 288 (53.2%) | 141 (52.6%) | 3.6 (3.5–3.7) | 3.4 (3.3–3.5) | 0.671 (0.546–0.826) | <0.00015 | ||
ALP = alkaline phosphatase; CI = confidence interval; NE = not estimable; PSA = prostate-specific antigen; SSE = symptomatic skeletal event
a Defined as occurrence of any of the following: external beam radiotherapy to relieve pain, or pathologic fracture, or spinal cord compression, or tumor-related orthopedic surgical intervention.
b not estimable owing to insufficient events after the median
c Defined as ≥25% increase compared to baseline/nadir.
d Defined as a ≥25% increase and an increase in absolute value of ≥2 ng/mL compared to baseline/nadir.
Subgroup survival analysis
Subgroup survival analysis showed a consistent survival benefit for treatment with Xofigo, independent of use of bisphosphonates at baseline and prior use of docetaxel.
A statistically significant overall survival benefit of treatment could not be demonstrated in the subgroups of patients with fewer than 6 metastases (HR for radium-223 to placebo 0.901; 95% CI [0.553-1.466], p=0.674) or a baseline total alkaline phosphatase (ALP) <220 U/L (HR 0.823; 95% CI [0.633-1.068], p=0.142) in the phase III ALSYMPCA study. Therefore, efficacy may be diminished in patients with a low level of osteoblastic activity from their bone metastases.
Quality of life
Health Related Quality of Life (HRQOL) was assessed in the phase III ALSYMPCA study using specific questionnaires: the EQ-5D (generic instrument) and the FACT-P (prostate cancer specific instrument). Both groups experience a loss of quality of life. Relative to placebo, the decline in quality of life was slower for Xofigo during the on-treatment period as measured by EQ-5D utility index score (-0.040 versus –0.109; p=0.001), EQ-5D self-reported Visual Analogue health status scores (VAS) (-2.661 versus -5.860; p=0.018) and the FACT P total score (-3.880 versus -7.651, p=0.006) but did not reach published minimally important differences. There is limited evidence that the delay in loss of HRQOL extends beyond the treatment period.
Pain relief
The results from the phase III ALSYPMCA study regarding time to external beam radiation therapy (EBRT) for pain relief and fewer patients reporting bone pain as an adverse event in the Xofigo group indicate a positive effect on bone pain.
Subsequent treatment with cytotoxic substances
In the course of the 2:1 randomised ALSYMPCA study, 93 (15.5%) patients in the Xofigo group and 54 (17.9%) patients in the placebo group received cytotoxic chemotherapy at varying times after the last treatment. No differences in haematological laboratory values were apparent between the two groups.
Combination with abiraterone and prednisone/prednisolone
The clinical efficacy and safety of concurrent initiation of Xofigo, abiraterone acetate and prednisone/prednisolone treatment was assessed in a randomized, placebo-controlled multicenter phase III study (ERA-223 trial) in 806 chemotherapy-naïve patients with asymptomatic or mildly symptomatic castration resistant prostate cancer with bone metastases. The study was unblinded early based on an Independent Data Monitoring Committee Recommendation. At an interim analysis, an increased incidence of fractures (28.6% vs 11.4%) and reduced median overall survival (30.7 months versus 33.3 months, HR 1.195, 95% CI [0.950-1.505], p=0.13) was observed among patients receiving Xofigo in combination with abiraterone acetate and prednisone/prednisolone compared to patients receiving placebo in combination with abiraterone acetate and prednisone/prednisolone.
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with Xofigo in all subsets of the paediatric population in the treatment of all conditions included in the category of malignant neoplasms (except central nervous system tumours, haematopoietic and lymphoid tissue neoplasms) and in the treatment of multiple myeloma (see section 4.2 for information on paediatric use).
Pharmacokinetic properties
General introduction
Pharmacokinetic, biodistribution and dosimetry data have been obtained from 3 phase I studies. Pharmacokinetic data were obtained in 25 patients at activities ranging from 51 to 276 kBq/kg. Pharmacokinetic, biodistribution and dosimetry data were obtained in 6 patients at an activity of 110 kBq/kg given twice, 6 weeks apart, and in 10 patients at an activity of 55, 110 or 221 kBq/kg.
Absorption
Xofigo is administered as an intravenous injection and is thus 100% bioavailable.
Distribution and organ uptake
After intravenous injection, radium-223 is rapidly cleared from the blood and is incorporated primarily into bone and bone metastases, or is excreted into the intestine.
Fifteen minutes post injection, about 20% of the injected activity remained in the blood. At 4 hours, about 4% of the injected activity remained in the blood, decreasing to less than 1% at 24 hours after the injection. The volume of distribution was higher than the blood volume indicating distribution to peripheral compartments.
At 10 minutes post injection, activity was observed in the bone and in the intestine. At 4 hours post injection, the mean percentage of the radioactive dose present in bone and intestine was approximately 61% and 49%, respectively.
No significant uptake was seen in other organs such as heart, liver, kidneys, urinary bladder and spleen at 4 hours post injection.
Biotransformation
Radium-223 is an isotope which decays and is not metabolised.
Elimination
Faecal excretion is the major route of elimination from the body. About 5% is excreted in the urine and there is no evidence of hepatobiliary excretion.
The whole body measurements at 7 days after injection (after correcting for decay) indicate that a median of 76% of administered activity was excreted from the body. The rate of elimination of radium-223 dichloride from the gastrointestinal tract is influenced by the high variability in intestinal transit rates across the population, with the normal range from once daily to once weekly bowel evacuation.
Linearity/non-linearity
The pharmacokinetics of radium-223 dichloride were linear in the activity range investigated (51 to 276 kBq/kg).
Paediatric population
Safety and effectiveness of Xofigo have not been studied in children and adolescents below 18 years of age.
Preclinical safety data
Systemic toxicity
In single and repeated dose toxicity studies in rats, the main findings were reduced body weight gain, haematological changes, reduced serum alkaline phosphatase and microscopic findings in the bone marrow (depletion of haematopoietic cells, fibrosis), spleen (secondary extra-medullary haematopoiesis) and bone (depletion of osteocytes, osteoblasts, osteoclasts, fibro-osseous lesions, disruption/disorganisation of the physis/growth line). These findings were related to radiation-induced impairment of haematopoiesis and a reduction of osteogenesis and started at the lowest activity of 22 kBq per kg body weight (0.4 times the clinically recommended dose).
In dogs, haematological changes were observed starting at the lowest activity of 55 kBq/kg, the clinically recommended dose. Dose-limiting myelotoxicity was seen in dogs after single administration of 497 kBq radium-223 dichloride per kg body weight (9 times the clinically recommended activity).
After repeated administration of the clinically recommended activity of 55 kBq per kg body weight once every 4 weeks for 6 months, two dogs developed non-displaced pelvic fractures. Due to the presence of osteolysis of trabecular bone in other bone locations of treated animals in varying degree, a spontaneous fracture in the context of osteolysis cannot be excluded. The clinical relevance of these findings is unknown.
Retinal detachment was seen in dogs after a single injection of activities of 166 and 497 kBq per kg body weight (3 and 9 times the clinically recommended dose), but not after repeated administration of the clinically recommended activity of 55 kBq per kg body weight once every 4 weeks for 6 months. The exact mechanism for induction of retinal detachment is unknown, but literature data suggests that radium is specifically taken up in the tapetum lucidum of the canine eye. Since humans do not have a tapetum lucidum, the clinical relevance of these findings for humans is uncertain. No case of retinal detachment has been reported in clinical trials.
No histological changes were observed in organs involved in the excretion of radium-223 dichloride.
Osteosarcomas, a known effect of bone-seeking radionuclides, were observed at clinically relevant doses in rats 7–12 months after start of treatment. Osteosarcomas were not observed in dog studies. No case of osteosarcoma has been reported in clinical studies with Xofigo. The risk for patients to develop osteosarcomas with exposure to radium-223 is unknown at present. The presence of neoplastic changes, other than osteosarcomas, was also reported in the longer term (12 to 15 months) rat toxicity studies (see section 4.8).
Embryotoxicity/Reproduction toxicity
Studies on reproductive and developmental toxicity have not been performed. In general, radionuclides induce reproductive and developmental effects.
A minimal number of abnormal spermatocytes were seen in a few seminiferous tubules in the testes of male rats after a single administration of ≥2270 kBq/kg body weight radium-223 dichloride (≥41 times the clinically recommended activity). The testes seemed to otherwise be functioning normally and the epididymides revealed a normal content of spermatocytes. Uterine polyps (endometrial stroma) were observed in female rats after single or repeated administration of ≥359 kBq/kg body weight radium-223 dichloride (≥6.5 times the clinically recommended activity).
Since radium-223 distributes mainly to bone, the potential risk for adverse effects in the male gonads in cancer patients with castration-resistant prostate cancer is very low, but cannot be excluded (see section 4.6).
Genotoxicity/Carcinogenicity
Studies on the mutagenic and carcinogenic potential of Xofigo have not been performed. In general, radionuclides are considered to be genotoxic and carcinogenic.
Safety pharmacology
No significant effects were seen on vital organ systems, i.e. cardiovascular (dog), respiratory or central nervous systems (rat), after single dose administration of activities from 497 to 1100 kBq per kg body weight (9 [dog] to 20 [rat] times the clinically recommended activity).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.