ZOCOR Film-coated tablet Ref.[10687] Active ingredients: Simvastatin
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
Simvastatin is a prodrug and is hydrolyzed to its active β-hydroxyacid form, simvastatin acid, after administration. Simvastatin is a specific inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, the enzyme that catalyzes the conversion of HMG-CoA to mevalonate, an early and rate limiting step in the biosynthetic pathway for cholesterol. In addition, simvastatin reduces VLDL and TG and increases HDL-C.
12.2. Pharmacodynamics
Epidemiological studies have demonstrated that elevated levels of total-C, LDL-C, as well as decreased levels of HDL-C are associated with the development of atherosclerosis and increased cardiovascular risk. Lowering LDL-C decreases this risk. However, the independent effect of raising HDL-C or lowering TG on the risk of coronary and cardiovascular morbidity and mortality has not been determined.
12.3. Pharmacokinetics
Simvastatin is a lactone that is readily hydrolyzed in vivo to the corresponding β-hydroxyacid, a potent inhibitor of HMG-CoA reductase. Inhibition of HMG-CoA reductase is the basis for an assay in pharmacokinetic studies of the β-hydroxyacid metabolites (active inhibitors) and, following base hydrolysis, active plus latent inhibitors (total inhibitors) in plasma following administration of simvastatin.
Following an oral dose of 14C-labeled simvastatin in man, 13% of the dose was excreted in urine and 60% in feces. Plasma concentrations of total radioactivity (simvastatin plus 14C-metabolites) peaked at 4 hours and declined rapidly to about 10% of peak by 12 hours postdose. Since simvastatin undergoes extensive first-pass extraction in the liver, the availability of the drug to the general circulation is low (<5%).
Both simvastatin and its β-hydroxyacid metabolite are highly bound (approximately 95%) to human plasma proteins. Rat studies indicate that when radiolabeled simvastatin was administered, simvastatin-derived radioactivity crossed the blood-brain barrier.
The major active metabolites of simvastatin present in human plasma are the β-hydroxyacid of simvastatin and its 6'-hydroxy, 6'-hydroxymethyl, and 6'-exomethylene derivatives. Peak plasma concentrations of both active and total inhibitors were attained within 1.3 to 2.4 hours postdose. While the recommended therapeutic dose range is 5 to 40 mg/day, there was no substantial deviation from linearity of AUC of inhibitors in the general circulation with an increase in dose to as high as 120 mg. Relative to the fasting state, the plasma profile of inhibitors was not affected when simvastatin was administered immediately before an American Heart Association recommended low-fat meal.
In a study including 16 elderly patients between 70 and 78 years of age who received ZOCOR 40 mg/day, the mean plasma level of HMG-CoA reductase inhibitory activity was increased approximately 45% compared with 18 patients between 18-30 years of age. Clinical study experience in the elderly (n=1522), suggests that there were no overall differences in safety between elderly and younger patients [see Use in Specific Populations (8.5)].
Kinetic studies with another statin, having a similar principal route of elimination, have suggested that for a given dose level higher systemic exposure may be achieved in patients with severe renal insufficiency (as measured by creatinine clearance).
Simvastatin acid is a substrate of the transport protein OATP1B1. Concomitant administration of medicinal products that are inhibitors of the transport protein OATP1B1 may lead to increased plasma concentrations of simvastatin acid and an increased risk of myopathy. For example, cyclosporine has been shown to increase the AUC of statins; although the mechanism is not fully understood, the increase in AUC for simvastatin acid is presumably due, in part, to inhibition of CYP3A4 and/or OATP1B1.
The risk of myopathy is increased by high levels of HMG-CoA reductase inhibitory activity in plasma. Inhibitors of CYP3A4 can raise the plasma levels of HMG-CoA reductase inhibitory activity and increase the risk of myopathy [see Warnings and Precautions (5.1) and Drug Interactions (7.1)].
Table 3. Effect of Coadministered Drugs or Grapefruit Juice on Simvastatin Systemic Exposure:
| Coadministered Drug or Grapefruit Juice | Dosing of Coadministered Drug or Grapefruit Juice | Dosing of Simvastatin | Geometric Mean Ratio (Ratio* with / without coadministered drug) No Effect = 1.00 | ||
|---|---|---|---|---|---|
| AUC | Cmax | ||||
| Contraindicated with simvastatin [see Contraindications (4) and Warnings and Precautions (5.1)] | |||||
| Telithromycin† | 200 mg QD for 4 days | 80 mg | simvastatin acid‡ simvastatin | 12 8.9 | 15 5.3 |
| Nelfinavirn† | 1250 mg BID for 14 days | 20 mg QD for 28 days | simvastatin acid‡ simvastatin | 6 | 6.2 |
| Itraconazolen† | 200 mg QD for 4 days | 80 mg | simvastatin acid‡ simvastatin | 13.1 13.1 | |
| Posaconazole | 100 mg (oral suspension) QD for 13 days | 40 mg | simvastatin acid simvastatin | 7.3 10.3 | 9.2 9.4 |
| 200 mg (oral suspension) QD for 13 days | 40 mg | simvastatin acid simvastatin | 8.5 10.6 | 9.5 11.4 | |
| Gemfibrozil | 600 mg BID for 3 days | 40 mg | simvastatin acid simvastatin | 2.85 1.35 | 2.18 0.91 |
| Avoid grapefruit juice with simvastatin [see Warnings and Precautions (5.1)] | |||||
| Grapefruit Juice§ (high dose) | 200 mL of double-strength TID¶ | 60 mg single dose | simvastatin acid simvastatin | 7 16 | |
| Grapefruit Juice§ (low dose) | 8 oz (about 237 mL) of single-strength# | 20 mg single dose | simvastatin acid simvastatin | 1.3 1.9 | |
| Avoid taking with >10 mg simvastatin, based on clinical and/or postmarketing experience [see Warnings and Precautions (5.1)] | |||||
| Verapamil SR | 240 mg QD Days 1-7 then 240 mg BID on Days 8-10 | 80 mg on Day 10 | simvastatin acid simvastatin | 2.3 2.5 | 2.4 2.1 |
| Diltiazem | 120 mg BID for 10 days | 80 mg on Day 10 | simvastatin acid simvastatin | 2.69 3.10 | 2.69 2.88 |
| Diltiazem | 120 mg BID for 14 days | 20 mg on Day 14 | simvastatin | 4.6 | 3.6 |
| Dronedarone | 400 mg BID for 14 days | 40 mg QD for 14 days | simvastatin acid simvastatin | 1.96 3.90 | 2.14 3.75 |
| Avoid taking with >20 mg simvastatin, based on clinical and/or postmarketing experience [see Warnings and Precautions (5.1)] | |||||
| Amiodarone | 400 mg QD for 3 days | 40 mg on Day 3 | simvastatin acid simvastatin | 1.75 1.76 | 1.72 1.79 |
| Amlodipine | 10 mg QD × 10 days | 80 mg on Day 10 | simvastatin acid simvastatin | 1.58 1.77 | 1.56 1.47 |
| Ranolazine SR | 1000 mg BID for 7 days | 80 mg on Day 1 and Days 6-9 | simvastatin acid simvastatin | 2.26 1.86 | 2.28 1.75 |
| Avoid taking with >20 mg simvastatin (or 40 mg for patients who have previously taken 80 mg simvastatin chronically, e.g., for 12 months or more, without evidence of muscle toxicity), based on clinical experience | |||||
| Lomitapide | 60 mg QD for 7 days | 40 mg single dose | simvastatin acid simvastatin | 1.7 2 | 1.6 2 |
| Lomitapide | 10 mg QD for 7 days | 20 mg single dose | simvastatin acid simvastatin | 1.4 1.6 | 1.4 1.7 |
| No dosing adjustments required for the following: | |||||
| Fenofibrate | 160 mg QD × 14 days | 80 mg QD on Days 8-14 | simvastatin acid simvastatin | 0.64 0.89 | 0.89 0.83 |
| Niacin extended-release | 2 g single dose | 20 mg single dose | simvastatin acid simvastatin | 1.6 1.4 | 1.84 1.08 |
| Propranolol | 80 mg single dose | 80 mg single dose | total inhibitor | 0.79 | ↓ from 33.6 to 21.1 ng∙eq/mL |
| active inhibitor | 0.79 | ↓ from 7.0 to 4.7 ng∙eq/mL | |||
* Results based on a chemical assay except results with propranolol as indicated.
† Results could be representative of the following CYP3A4 inhibitors: ketoconazole, erythromycin, clarithromycin, HIV protease inhibitors, and nefazodone.
‡ Simvastatin acid refers to the β-hydroxyacid of simvastatin.
§ The effect of amounts of grapefruit juice between those used in these two studies on simvastatin pharmacokinetics has not been studied.
¶ Double-strength: one can of frozen concentrate diluted with one can of water. Grapefruit juice was administered TID for 2 days, and 200 mL together with single dose simvastatin and 30 and 90 minutes following single dose simvastatin on Day 3.
# Single-strength: one can of frozen concentrate diluted with 3 cans of water. Grapefruit juice was administered with breakfast for 3 days, and simvastatin was administered in the evening on Day 3.
In a study of 12 healthy volunteers, simvastatin at the 80-mg dose had no effect on the metabolism of the probe cytochrome P450 isoform 3A4 (CYP3A4) substrates midazolam and erythromycin. This indicates that simvastatin is not an inhibitor of CYP3A4, and, therefore, is not expected to affect the plasma levels of other drugs metabolized by CYP3A4.
Coadministration of simvastatin (40 mg QD for 10 days) resulted in an increase in the maximum mean levels of cardioactive digoxin (given as a single 0.4 mg dose on day 10) by approximately 0.3 ng/mL.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 72-week carcinogenicity study, mice were administered daily doses of simvastatin of 25, 100, and 400 mg/kg body weight, which resulted in mean plasma drug levels approximately 1, 4, and 8 times higher than the mean human plasma drug level, respectively (as total inhibitory activity based on AUC) after an 80-mg oral dose. Liver carcinomas were significantly increased in high-dose females and mid- and high-dose males with a maximum incidence of 90% in males. The incidence of adenomas of the liver was significantly increased in mid- and high-dose females. Drug treatment also significantly increased the incidence of lung adenomas in mid- and high-dose males and females. Adenomas of the Harderian gland (a gland of the eye of rodents) were significantly higher in high-dose mice than in controls. No evidence of a tumorigenic effect was observed at 25 mg/kg/day.
In a separate 92-week carcinogenicity study in mice at doses up to 25 mg/kg/day, no evidence of a tumorigenic effect was observed (mean plasma drug levels were 1 times higher than humans given 80 mg simvastatin as measured by AUC).
In a two-year study in rats at 25 mg/kg/day, there was a statistically significant increase in the incidence of thyroid follicular adenomas in female rats exposed to approximately 11 times higher levels of simvastatin than in humans given 80 mg simvastatin (as measured by AUC).
A second two-year rat carcinogenicity study with doses of 50 and 100 mg/kg/day produced hepatocellular adenomas and carcinomas (in female rats at both doses and in males at 100 mg/kg/day). Thyroid follicular cell adenomas were increased in males and females at both doses; thyroid follicular cell carcinomas were increased in females at 100 mg/kg/day. The increased incidence of thyroid neoplasms appears to be consistent with findings from other statins. These treatment levels represented plasma drug levels (AUC) of approximately 7 and 15 times (males) and 22 and 25 times (females) the mean human plasma drug exposure after an 80 milligram daily dose.
No evidence of mutagenicity was observed in a microbial mutagenicity (Ames) test with or without rat or mouse liver metabolic activation. In addition, no evidence of damage to genetic material was noted in an in vitro alkaline elution assay using rat hepatocytes, a V-79 mammalian cell forward mutation study, an in vitro chromosome aberration study in CHO cells, or an in vivo chromosomal aberration assay in mouse bone marrow.
There was decreased fertility in male rats treated with simvastatin for 34 weeks at 25 mg/kg body weight (4 times the maximum human exposure level, based on AUC, in patients receiving 80 mg/day); however, this effect was not observed during a subsequent fertility study in which simvastatin was administered at this same dose level to male rats for 11 weeks (the entire cycle of spermatogenesis including epididymal maturation). No microscopic changes were observed in the testes of rats from either study. At 180 mg/kg/day, (which produces exposure levels 22 times higher than those in humans taking 80 mg/day based on surface area, mg/m 2), seminiferous tubule degeneration (necrosis and loss of spermatogenic epithelium) was observed. In dogs, there was drug-related testicular atrophy, decreased spermatogenesis, spermatocytic degeneration and giant cell formation at 10 mg/kg/day, (approximately 2 times the human exposure, based on AUC, at 80 mg/day). The clinical significance of these findings is unclear.
13.2. Animal Toxicology and/or Pharmacology
CNS Toxicity
Optic nerve degeneration was seen in clinically normal dogs treated with simvastatin for 14 weeks at 180 mg/kg/day, a dose that produced mean plasma drug levels about 12 times higher than the mean plasma drug level in humans taking 80 mg/day.
A chemically similar drug in this class also produced optic nerve degeneration (Wallerian degeneration of retinogeniculate fibers) in clinically normal dogs in a dose-dependent fashion starting at 60 mg/kg/day, a dose that produced mean plasma drug levels about 30 times higher than the mean plasma drug level in humans taking the highest recommended dose (as measured by total enzyme inhibitory activity). This same drug also produced vestibulocochlear Wallerian-like degeneration and retinal ganglion cell chromatolysis in dogs treated for 14 weeks at 180 mg/kg/day, a dose that resulted in a mean plasma drug level similar to that seen with the 60 mg/kg/day dose.
CNS vascular lesions, characterized by perivascular hemorrhage and edema, mononuclear cell infiltration of perivascular spaces, perivascular fibrin deposits and necrosis of small vessels were seen in dogs treated with simvastatin at a dose of 360 mg/kg/day, a dose that produced mean plasma drug levels that were about 14 times higher than the mean plasma drug levels in humans taking 80 mg/day. Similar CNS vascular lesions have been observed with several other drugs of this class.
There were cataracts in female rats after two years of treatment with 50 and 100 mg/kg/day (22 and 25 times the human AUC at 80 mg/day, respectively) and in dogs after three months at 90 mg/kg/day (19 times) and at two years at 50 mg/kg/day (5 times).
14. Clinical Studies
14.1 Clinical Studies in Adults
Reductions in Risk of CHD Mortality and Cardiovascular Events
In 4S, the effect of therapy with ZOCOR on total mortality was assessed in 4,444 patients with CHD and baseline total cholesterol 212-309 mg/dL (5.5-8.0 mmol/L). In this multicenter, randomized, double-blind, placebo-controlled study, patients were treated with standard care, including diet, and either ZOCOR 20-40 mg/day (n=2,221) or placebo (n=2,223) for a median duration of 5.4 years. Over the course of the study, treatment with ZOCOR led to mean reductions in total-C, LDL-C and TG of 25%, 35%, and 10%, respectively, and a mean increase in HDL-C of 8%. ZOCOR significantly reduced the risk of mortality by 30% (p=0.0003, 182 deaths in the ZOCOR group vs 256 deaths in the placebo group). The risk of CHD mortality was significantly reduced by 42% (p=0.00001, 111 vs 189 deaths). There was no statistically significant difference between groups in non-cardiovascular mortality. ZOCOR significantly decreased the risk of having major coronary events (CHD mortality plus hospital-verified and silent non-fatal myocardial infarction [MI]) by 34% (p<0.00001, 431 vs 622 patients with one or more events). The risk of having a hospital-verified non-fatal MI was reduced by 37%. ZOCOR significantly reduced the risk for undergoing myocardial revascularization procedures (coronary artery bypass grafting or percutaneous transluminal coronary angioplasty) by 37% (p<0.00001, 252 vs 383 patients). ZOCOR significantly reduced the risk of fatal plus non-fatal cerebrovascular events (combined stroke and transient ischemic attacks) by 28% (p=0.033, 75 vs 102 patients). ZOCOR reduced the risk of major coronary events to a similar extent across the range of baseline total and LDL cholesterol levels. Because there were only 53 female deaths, the effect of ZOCOR on mortality in women could not be adequately assessed. However, ZOCOR significantly lessened the risk of having major coronary events by 34% (60 vs 91 women with one or more event). The randomization was stratified by angina alone (21% of each treatment group) or a previous MI. Because there were only 57 deaths among the patients with angina alone at baseline, the effect of ZOCOR on mortality in this subgroup could not be adequately assessed. However, trends in reduced coronary mortality, major coronary events and revascularization procedures were consistent between this group and the total study cohort. Additionally, ZOCOR resulted in similar decreases in relative risk for total mortality, CHD mortality, and major coronary events in elderly patients (≥65 years), compared with younger patients.
The Heart Protection Study (HPS) was a large, multi-center, placebo-controlled, double-blind study with a mean duration of 5 years conducted in 20,536 patients (10,269 on ZOCOR 40 mg and 10,267 on placebo). Patients were allocated to treatment using a covariate adaptive method3 which took into account the distribution of 10 important baseline characteristics of patients already enrolled and minimized the imbalance of those characteristics across the groups. Patients had a mean age of 64 years (range 40-80 years), were 97% Caucasian and were at high risk of developing a major coronary event because of existing CHD (65%), diabetes (Type 2, 26%; Type 1, 3%), history of stroke or other cerebrovascular disease (16%), peripheral vessel disease (33%), or hypertension in males ≥65 years (6%). At baseline, 3,421 patients (17%) had LDL-C levels below 100 mg/dL, of whom 953 (5%) had LDL-C levels below 80 mg/dL; 7,068 patients (34%) had levels between 100 and 130 mg/dL; and 10,047 patients (49%) had levels greater than 130 mg/dL.
The HPS results showed that ZOCOR 40 mg/day significantly reduced: total and CHD mortality; non-fatal MI, stroke, and revascularization procedures (coronary and non-coronary) (see Table 4).
Table 4. Summary of Heart Protection Study Results:
| Endpoint | ZOCOR (N=10,269) n (%)* | Placebo (N=10,267) n (%)* | Risk Reduction (%) (95% CI) | p-Value |
|---|---|---|---|---|
| Primary | ||||
| Mortality | 1,328 (12.9) | 1,507 (14.7) | 13 (6-19) | p=0.0003 |
| CHD mortality | 587 (5.7) | 707 (6.9) | 18 (8-26) | p=0.0005 |
| Secondary | ||||
| Non-fatal MI | 357 (3.5) | 574 (5.6) | 38 (30-46) | p<0.0001 |
| Stroke | 444 (4.3) | 585 (5.7) | 25 (15-34) | p<0.0001 |
| Tertiary | ||||
| Coronary revascularization | 513 (5) | 725 (7.1) | 30 (22-38) | p<0.0001 |
| Peripheral and other non-coronary revascularization | 450 (4.4) | 532 (5.2) | 16 (5-26) | p=0.006 |
* n = number of patients with indicated event
Two composite endpoints were defined in order to have sufficient events to assess relative risk reductions across a range of baseline characteristics (see Figure 1). A composite of major coronary events (MCE) was comprised of CHD mortality and non-fatal MI (analyzed by time-to-first event; 898 patients treated with ZOCOR had events and 1,212 patients on placebo had events). A composite of major vascular events (MVE) was comprised of MCE, stroke and revascularization procedures including coronary, peripheral and other non-coronary procedures (analyzed by time-to-first event; 2,033 patients treated with ZOCOR had events and 2,585 patients on placebo had events). Significant relative risk reductions were observed for both composite endpoints (27% for MCE and 24% for MVE, p<0.0001). Treatment with ZOCOR produced significant relative risk reductions for all components of the composite endpoints. The risk reductions produced by ZOCOR in both MCE and MVE were evident and consistent regardless of cardiovascular disease related medical history at study entry (i.e., CHD alone; or peripheral vascular disease, cerebrovascular disease, diabetes or treated hypertension, with or without CHD), gender, age, creatinine levels up to the entry limit of 2.3 mg/dL, baseline levels of LDL-C, HDL-C, apolipoprotein B and A-1, baseline concomitant cardiovascular medications (i.e., aspirin, beta blockers, or calcium channel blockers), smoking status, alcohol intake, or obesity. Diabetics showed risk reductions for MCE and MVE due to ZOCOR treatment regardless of baseline HbA1c levels or obesity with the greatest effects seen for diabetics without CHD.
Figure 1. The Effects of Treatment with ZOCOR on Major Vascular Events and Major Coronary Events in HPS:
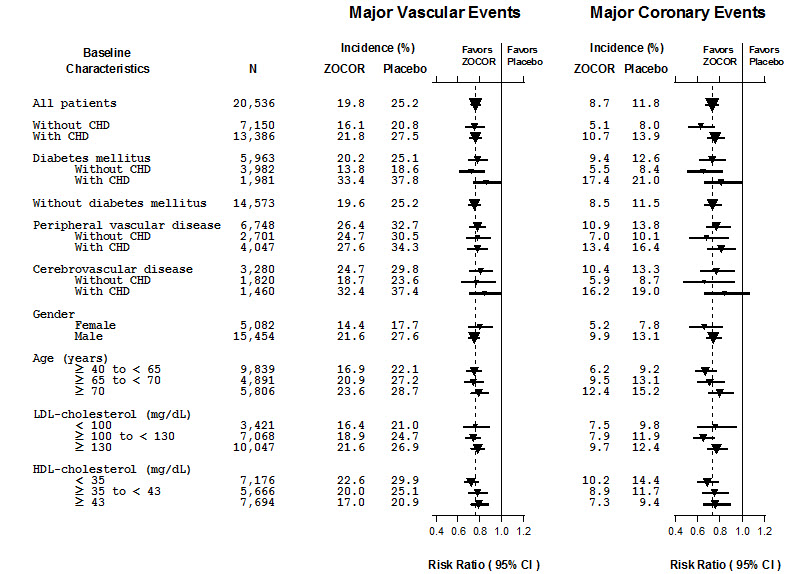
N = number of patients in each subgroup. The inverted triangles are point estimates of the relative risk, with their 95% confidence intervals represented as a line. The area of a triangle is proportional to the number of patients with MVE or MCE in the subgroup relative to the number with MVE or MCE, respectively, in the entire study population. The vertical solid line represents a relative risk of one. The vertical dashed line represents the point estimate of relative risk in the entire study population.
3 D.R. Taves, Minimization: a new method of assigning patients to treatment and control groups. Clin. Pharmacol. Ther. 15 (1974 ), pp. 443-453
Angiographic Studies
In the Multicenter Anti-Atheroma Study, the effect of simvastatin on atherosclerosis was assessed by quantitative coronary angiography in hypercholesterolemic patients with CHD. In this randomized, double-blind, controlled study, patients were treated with simvastatin 20 mg/day or placebo. Angiograms were evaluated at baseline, two and four years. The co-primary study endpoints were mean change per-patient in minimum and mean lumen diameters, indicating focal and diffuse disease, respectively. ZOCOR significantly slowed the progression of lesions as measured in the Year 4 angiogram by both parameters, as well as by change in percent diameter stenosis. In addition, simvastatin significantly decreased the proportion of patients with new lesions and with new total occlusions.
Modifications of Lipid Profiles
Primary Hyperlipidemia (Fredrickson type lla and llb)
ZOCOR has been shown to be effective in reducing total-C and LDL-C in heterozygous familial and non-familial forms of hyperlipidemia and in mixed hyperlipidemia. Maximal to near maximal response is generally achieved within 4-6 weeks and maintained during chronic therapy. ZOCOR significantly decreased total-C, LDL-C, total-C/HDL-C ratio, and LDL-C/HDL-C ratio; ZOCOR also decreased TG and increased HDL-C (see Table 5).
Table 5. Mean Response in Patients with Primary Hyperlipidemia and Combined (mixed) Hyperlipidemia (Mean Percent Change from Baseline After 6 to 24 Weeks):
| TREATMENT | N | TOTAL-C | LDL-C | HDL-C | TG* |
|---|---|---|---|---|---|
| Lower Dose Comparative Study† (Mean % Change at Week 6) | |||||
| ZOCOR 5 mg q.p.m. | 109 | -19 | -26 | 10 | -12 |
| ZOCOR 10 mg q.p.m. | 110 | -23 | -30 | 12 | -15 |
| Scandinavian Simvastatin Survival Study‡ (Mean % Change at Week 6) | |||||
| Placebo | 2223 | -1 | -1 | 0 | -2 |
| ZOCOR 20 mg q.p.m. | 2221 | -28 | -38 | 8 | -19 |
| Upper Dose Comparative Study§ (Mean % Change Averaged at Weeks 18 and 24) | |||||
| ZOCOR 40 mg q.p.m. | 433 | -31 | -41 | 9 | -18 |
| ZOCOR 80 mg q.p.m.¶ | 664 | -36 | -47 | 8 | -24 |
| Multi-Center Combined Hyperlipidemia Study# (Mean % Change at Week 6) | |||||
| Placebo | 125 | 1 | 2 | 3 | -4 |
| ZOCOR 40 mg q.p.m. | 123 | -25 | -29 | 13 | -28 |
| ZOCOR 80 mg q.p.m. | 124 | -31 | -36 | 16 | -33 |
* median percent change
† mean baseline LDL-C 24 4 mg/dL and median baseline TG 168 mg/dL
‡ mean baseline LDL-C 188 mg/dL and median baseline TG 128 mg/dL
§ mean baseline LDL-C 226 mg/dL and median baseline TG 156 mg/dL
¶ 21% and 36% median reduction in TG in patients with TG ≤200 mg/dL and TG >200 mg/dL, respectively. Patients with TG >350 mg/dL were excluded
# mean baseline LDL-C 156 mg/dL and median baseline TG 391 mg/dL.
Hypertriglyceridemia (Fredrickson type lV)
The results of a subgroup analysis in 74 patients with type lV hyperlipidemia from a 130-patient, double-blind, placebo-controlled, 3-period crossover study are presented in Table 6.
Table 6. Six-week, Lipid-lowering Effects of Simvastatin in Type lV Hyperlipidemia Median Percent Change (25th and 75th percentile) from Baseline*:
| TREATMENT | N | Total-C | LDL-C | HDL-C | TG | VLDL-C | Non-HDL-C |
|---|---|---|---|---|---|---|---|
| Placebo | 74 | +2 (-7, +7) | +1 (-8, +14) | +3 (-3, +10) | -9 (-25, +13) | -7 (-25, +11) | +1 (-9, +8) |
| ZOCOR 40 mg/day | 74 | -25 (-34, -19) | -28 (-40, -17) | +11 (+5, +23) | -29 (-43, -16) | -37 (-54, -23) | -32 (-42, -23) |
| ZOCOR 80 mg/day | 74 | -32 (-38, -24) | -37 (-46, -26) | +15 (+5, +23) | -34 (-45, -18) | -41 (-57, -28) | -38 (-49, -32) |
* The median baseline values (mg/dL) for the patients in this study were: total-C = 254, LDL-C = 135, HDL-C = 36, TG = 404, VLDL-C = 83, and non-HDL-C = 215.
Dysbetalipoproteinemia (Fredrickson type lll)
The results of a subgroup analysis in 7 patients with type lll hyperlipidemia (dysbetalipoproteinemia) (apo E2/2) (VLDL-C/TG>0.25) from a 130-patient, double-blind, placebo-controlled, 3-period crossover study are presented in Table 7.
Table 7. Six-week, Lipid-lowering Effects of Simvastatin in Type lll Hyperlipidemia Median Percent Change (min, max) from Baseline*:
| TREATMENT | N | Total-C | LDL-C + IDL | HDL-C | TG | VLDL-C + IDL | Non-HDL-C |
|---|---|---|---|---|---|---|---|
| Placebo | 7 | -8 (-24, +34) | -8 (-27, +23) | -2 (-21, +16) | +4 (-22, +90) | -4 (-28, +78) | -8 (-26, -39) |
| ZOCOR 40 mg/day | 7 | -50 (-66, -39) | -50 (-60, -31) | +7 (-8, +23) | -41 (-74, -16) | -58 (-90, -37) | -57 (-72, -44) |
| ZOCOR 80 mg/day | 7 | -52 (-55, -41) | -51 (-57, -28) | +7 (-5, +29) | -38 (-58, +2) | -60 (-72, -39) | -59 (-61, -46) |
* The median baseline values (mg/dL) were: total-C = 324 , LDL-C = 121, HDL-C = 31, TG = 4 11, VLDL-C = 170, and non-HDL-C = 291.
Homozygous Familial Hypercholesterolemia
In a controlled clinical study, 12 patients 15-39 years of age with homozygous familial hypercholesterolemia received simvastatin 40 mg/day in a single dose or in 3 divided doses, or 80 mg/day in 3 divided doses. In 11 patients with reductions in LDL-C, the mean LDL-C changes for the 40- and 80-mg doses were 14% (range 8% to 23%, median 12%) and 30% (range 14% to 46%, median 29%), respectively. One patient had an increase of 15% in LDL-C. Another patient with absent LDL-C receptor function had an LDL-C reduction of 41% with the 80-mg dose.
Endocrine Function
In clinical studies, simvastatin did not impair adrenal reserve or significantly reduce basal plasma cortisol concentration. Small reductions from baseline in basal plasma testosterone in men were observed in clinical studies with simvastatin, an effect also observed with other statins and the bile acid sequestrant cholestyramine. There was no effect on plasma gonadotropin levels. In a placebo-controlled, 12-week study there was no significant effect of simvastatin 80 mg on the plasma testosterone response to human chorionic gonadotropin. In another 24-week study, simvastatin 20-40 mg had no detectable effect on spermatogenesis. In 4S, in which 4,444 patients were randomized to simvastatin 20-40 mg/day or placebo for a median duration of 5.4 years, the incidence of male sexual adverse events in the two treatment groups was not significantly different. Because of these factors, the small changes in plasma testosterone are unlikely to be clinically significant. The effects, if any, on the pituitary-gonadal axis in pre-menopausal women are unknown.
14.2 Clinical Studies in Adolescents
In a double-blind, placebo-controlled study, 175 patients (99 adolescent boys and 76 post-menarchal girls) 10-17 years of age (mean age 14.1 years) with heterozygous familial hypercholesterolemia (HeFH) were randomized to simvastatin (n=106) or placebo (n=67) for 24 weeks (base study). Inclusion in the study required a baseline LDL-C level between 160 and 400 mg/dL and at least one parent with an LDL-C level >189 mg/dL. The dosage of simvastatin (once daily in the evening) was 10 mg for the first 8 weeks, 20 mg for the second 8 weeks, and 40 mg thereafter. In a 24-week extension, 144 patients elected to continue therapy with simvastatin 40 mg or placebo.
ZOCOR significantly decreased plasma levels of total-C, LDL-C, and Apo B (see Table 8). Results from the extension at 48 weeks were comparable to those observed in the base study.
Table 8. Lipid-Lowering Effects of Simvastatin in Adolescent Patients with Heterozygous Familial Hypercholesterolemia (Mean Percent Change from Baseline):
| Dosage | Duration | N | Total-C | LDL-C | HDL-C | TG* | Apo B | |
|---|---|---|---|---|---|---|---|---|
| Placebo | 24 Weeks | 67 | % Change from Baseline (95% CI) | 1.6 (-2.2, 5.3) | 1.1 (-3.4, 5.5) | 3.6 (-0.7, 8.0) | -3.2 (-11.8, 5.4) | -0.5 (-4.7, 3.6) |
| Mean baseline, mg/dL (SD) | 278.6 (51.8) | 211.9 (49.0) | 46.9 (11.9) | 90.0 (50.7) | 186.3 (38.1) | |||
| ZOCOR | 24 Weeks | 106 | % Change from Baseline (95% CI) | -26.5 (-29.6, -23.3) | -36.8 (-40.5, -33.0) | 8.3 (4.6, 11.9) | -7.9 (-15.8, 0.0) | -32.4 (-35.9, -29.0) |
| Mean baseline, mg/dL (SD) | 270.2 (44.0) | 203.8 (41.5) | 47.7 (9.0) | 78.3 (46.0) | 179.9 (33.8) |
* median percent change
After 24 weeks of treatment, the mean achieved LDL-C value was 124.9 mg/dL (range: 64.0-289.0 mg/dL) in the ZOCOR 40 mg group compared to 207.8 mg/dL (range: 128.0-334.0 mg/dL) in the placebo group.
The safety and efficacy of doses above 40 mg daily have not been studied in children with HeFH. The long-term efficacy of simvastatin therapy in childhood to reduce morbidity and mortality in adulthood has not been established.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.