Source: European Medicines Agency (EU) Revision Year: 2017 Publisher: Merck Sharp & Dohme Ltd, Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, United Kingdom
Pharmacotherapeutic group: Antithrombotic agents, platelet aggregation inhibitors excluding heparin
ATC code: B01AC26
Vorapaxar is a selective and reversible inhibitor of the PAR-1 receptors on platelets that are activated by thrombin.
Vorapaxar inhibits thrombin-induced platelet aggregation in in vitro studies. In addition, vorapaxar inhibits thrombin receptor agonist peptide (TRAP)-induced platelet aggregation without affecting coagulation parameters. Vorapaxar does not inhibit platelet aggregation induced by other agonists such as adenosine diphosphate (ADP), collagen or a thromboxane mimetic.
At a dose of 2.5 mg of vorapaxar sulfate (equivalent to 2.08 mg vorapaxar) daily, vorapaxar consistently achieves ≥80% inhibition of TRAP-induced platelet aggregation within one week of initiation of treatment. The duration of platelet inhibition is dose and concentration dependent. Inhibition of TRAP-induced platelet aggregation at a level of ≥80% may last for 2 to 4 weeks after discontinuation of daily doses of vorapaxar sulfate 2.5 mg. The duration of these pharmacodynamic effects is consistent with the drug’s elimination half-life.
Consistent with its selective molecular target (PAR-1), vorapaxar has no effect on ADP-induced platelet aggregation in healthy subjects and patient populations.
In healthy volunteer studies, no changes in platelet P-selectin and soluble CD40 ligand (sCD40L) expression or coagulation test parameters (TT, PT, aPTT, ACT, ECT) occurred after single or multiple dose (28 days) administration of vorapaxar. No meaningful changes in P-selectin, sCD40L and hs-CRP concentrations were observed in patients treated with vorapaxar in the Phase ⅔ clinical trials.
The effect of vorapaxar on the QTc interval was evaluated in a thorough QT study and in other studies. Vorapaxar had no effect on the QTc interval at single doses up to 120 mg.
Zontivity has been shown to reduce the rate of a combined endpoint of cardiovascular death, MI, stroke, and urgent coronary revascularization (UCR).
The clinical evidence for the effect of Zontivity in patients with a history of myocardial infarction, defined as a spontaneous MI ≥2 weeks but 12 months prior, is derived from TRA 2°P-TIMI 50 (Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events). TRA 2°P-TIMI 50 was a multicenter, randomized, double-blind, placebo-controlled study conducted in patients who had evidence or a history of atherosclerosis involving the coronary, cerebral, or peripheral vascular systems. Patients were randomized to receive daily treatment with 2.5 mg vorapaxar sulfate (n=13,225) or placebo (n=13,224) in addition to other standard therapy. The study’s primary endpoint was the composite of cardiovascular death, MI, stroke, and UCR. The composite of cardiovascular death, MI, and stroke were assessed as secondary endpoint. The median duration of treatment with vorapaxar was 823 days (interquartile range: 645-1016 days). The findings for the primary efficacy composite endpoint show a 3-year Kaplan-Meier (K-M) event rate of 11.2% in the Zontivity group compared with that of 12.4% in the placebo group (Hazard Ratio [HR]: 0.88; 95% Confidence Interval [CI], 0.82 to 0.95; p=0.001) and demonstrated superiority of Zontivity over placebo in preventing CV death, MI, stroke, or UCR.
The findings for the key secondary efficacy endpoint, a 3-year K-M event rate of 9.3% in the Zontivity group compared with that of 10.5% in placebo group (HR: 0.87; 95% CI, 0.80 to 0.94; p<0.001).
Although the TRA 2°P-TIMI 50 trial was not designed to evaluate the relative benefit of Zontivity in individual patient subgroups, the benefit was most apparent in patients who were enrolled on the basis of a recent MI as indicated by a history of spontaneous MI ≥2 weeks but ≤12 months prior (post-MI or PAD patient population) with no history of stroke or TIA. Of these patients, 10,080 received Zontivity (8,458 post-MI and 1,622 PAD) and 10,090 received placebo (8,439 post-MI and 1,651 PAD) in addition to standard of care, including antiplatelet therapy with acetylsalicylic acid and thienopyridine. Of the patients with MI without a history of stroke or TIA, 21% were receiving acetylsalicylic acid without thienopyridine, 1% was receiving a thienopyridine without acetylsalicylic acid, and 77% were receiving both acetylsalicylic acid and a thienopyridine when they enrolled in the trial. Of the patients with PAD without a history of stroke or TIA, 61% were receiving acetylsalicylic acid without thienopyridine, 8% were receiving a thienopyridine without acetylsalicylic acid, and 27% were receiving both acetylsalicylic acid and a thienopyridine when they enrolled. In post-MI and PAD patients, the median duration of treatment with Zontivity in these patients was 2.5 years (up to 4 years). This background therapy was to be continued during the trial at the treating physician’s discretion, per standard of care.
The post-MI patient population with no history of stroke or TIA was 88% Caucasian, 20% female, and 29% ≥65 years of age, with a median age of 58 years, and included patients with diabetes (21%) and patients with hypertension (62%). The median Body Mass Index was 28.
The PAD patient population with no history of stroke or TIA was 90% Caucasian, 29% female, and 57% ≥65 years of age, with a median age of 66 years, and included patients with diabetes (35%) and patients with hypertension (82%). The median Body Mass Index was 27.
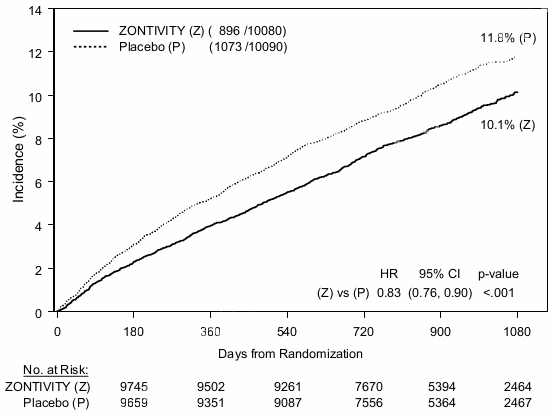
In the cohort of post-MI or PAD patients with no history of stroke or TIA, the findings for the primary and key secondary composite endpoints are consistent with the overall population (see Figure 1 and Table 4).
Among patients with a qualifying MI, Zontivity was initiated at least 2 weeks after the MI and within the first 12 months from the acute event. Within that period the effect was similar regardless of the time from qualifying MI to the start of therapy with Zontivity.
The treatment effect of vorapaxar on the primary and key secondary endpoints was shown to be durable and persistent over the length of the TRA 2°P – TIMI 50 study.
Figure 1. Time to First Occurrence of CV death, MI, Stroke or UCR in Post-MI or PAD Patients with No History of Stroke or TIA:
Table 4. Primary and Key Secondary Efficacy Endpoints in Post-MI or PAD Patients with No History of Stroke or TIA:
| Placebo (n=10.090) | Zontivity (n=10.080) | Hazard Ratio‡,§ (95% CI) | p-value§ | |||
|---|---|---|---|---|---|---|
| Endpoints | Patients with events* (%) | K-M %† | Patients with events* (%) | K-M%† | ||
| Primary Efficacy Endpoint (CV death/MI/stroke/UCR) | 1,073 (10.6%) | 11.8% | 896 (8.9%) | 10.1% | 0.83 (0.76-0.90) | <0.001 |
| CV Death | 154 (1.5%) | 129 (1.3%) | ||||
| ΕΜ | 531 (5.3%) | 450 (4.5%) | ||||
| Stroke | 123 (1.2%) | 91 (0.9%) | ||||
| UCR | 265 (2.6%) | 226 (2.2%) | ||||
| Key Secondary Efficacy Endpoint (CV death/MI/stroke)§ | 851 (8.4%) | 9.5% | 688 (6.8%) | 7.9% | 0.80 (0.73–0.89) | <0.001 |
| CV Death | 160 (1.6%) | 132 (1.3%) | ||||
| ΕΜ | 562 (5.6%) | 464 (4.6%) | ||||
| Stroke | 129 (1.3%) | 92 (0.9%) | ||||
* Each patient was counted only once (first component event) in the component summary that contributed to the primary efficacy endpoint
† K-M estimate at 1,080 days
‡ Hazard ratio is Zontivity group versus placebo group
§ Cox proportional hazard model with covariates treatment and stratification factors (qualifying atherosclerotic disease and planned thienopyridine use)
In the cohort of post-MI or PAD patients with no history of stroke or TIA, the net clinical outcome analysis based on multiple occurrences of endpoints (CV Death/MI/Stroke/GUSTO Severe) is constant over time at each of the censoring times examined (12, 18, 24, 30, and 36 months) at cumulative 6-month intervals. (See Table 5.)
Table 5. Multiple Occurrences of Net Clinical Outcome (CV Death/MI/Stroke/GUSTO Severe*) in Post-MI or PAD Patients with No History of Stroke or TIA:
| Placebo n=10.049 | Zontivity n=10.059 | Hazard Ratio†,‡ (95% CI) | p-value‡ | |
|---|---|---|---|---|
| Randomization to 12 months | ||||
| Total Events | 474 | 401 | 0.83 (0.73-0.95) | 0.008 |
| Patients with only one Event | 337 | 269 | ||
| Patients with two Events | 49 | 47 | ||
| Patients with ≥3 Events | 11 | 12 | ||
| Randomization to 18 months | ||||
| Total Events | 703 | 564 | 0.79 (0.71-0.89) | <0.001 |
| Patients with only one Event | 463 | 361 | ||
| Patients with two Events | 82 | 67 | ||
| Patients with ≥3 Events | 21 | 21 | ||
| Randomization to 24 months | ||||
| Total Events | 903 | 741 | 0.81 (0.73-0.89) | <0.001 |
| Patients with only one Event | 554 | 456 | ||
| Patients with two Events | 114 | 80 | ||
| Patients with ≥3 Events | 34 | 38 | ||
| Randomization to 30 months | ||||
| Total Events | 1.070 | 893 | 0.82 (0.75-0.90) | <0.001 |
| Patients with only one Event | 658 | 524 | ||
| Patients with two Events | 121 | 102 | ||
| Patients with ≥3 Events | 46 | 48 | ||
| Randomization to 36 months | ||||
| Total Events | 1.166 | 987 | 0.83 (0.76-0.91) | <0.001 |
| Patients with only one Event | 700 | 569 | ||
| Patients with two Events | 138 | 112 | ||
| Patients with ≥3 Events | 52 | 55 | ||
* Includes all CV Death, MI, Stroke and GUSTO severe events up to each timepoint as indicated in the table.
† Hazard Ratio is vorapaxar group versus placebo group.
‡ Hazard Ratio and p-value were calculated based on Andersen-Gill model with covariates treatment and stratification factor (planned thienopyridine use).
In post-MI or PAD patients with no history of stroke or TIA, an analysis of multiple occurrences of adjudicated endpoints indicates that Zontivity was associated with a reduction in the incidence of recurrent events.
Among post-MI or PAD patients without a history of stroke or TIA, Zontivity appeared to reduce the rate of definite stent thrombosis (HR 0.71 (0.51-0.99 for adjudicated “definite”) vs. placebo in subjects receiving any stent before or during the study.
Patients with a history of PAD but without a history of stroke or TIA randomized to vorapaxar had fewer peripheral revascularization procedures (15.4% v 19.3%, 3-year KM rates; HR 0.82 [0.71-0.94, 95% CI]; P=0.005) and fewer hospitalizations for acute limb ischemia (2.0% v 3.3%; HR 0.59 [0.40–0.86]; P=0.007) than patients randomized to placebo.
The treatment effect of Zontivity was consistent with the overall results across many subgroups, including sex; age; renal insufficiency; medical history of diabetes mellitus; tobacco use; concomitant therapies at baseline including thienopyridine, acetylsalicylic acid, and statins.
In TRA 2°P-TIMI 50, among patients who entered the trial, those with a history of ischaemic stroke had a higher 3 year K-M event rate for ICH on Zontivity plus standard care (2.7%) than on standard care alone (0.9%). In post-MI or PAD patients with no history of stroke or TIA, the 3 year K-M event rates for ICH were 0.6% and 0.5% for Zontivity plus standard care and standard care alone, respectively.
In the TRACER (Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome) trial, comprising patients with a NSTEACS (non-ST segment elevation acute coronary syndrome) who were largely antiplatelet naive, vorapaxar, with a loading dose of 40 mg and then maintained at 2.5 mg/day in addition to standard of care, initiated within 24 hours of NSTEACS, did not achieve its primary efficacy endpoint (cardiovascular death, MI, stroke, urgent coronary revascularization, and recurrent ischemia with rehospitalisation) and there was an increased risk of GUSTO moderate or severe bleeding.
The European Medicines Agency has deferred the obligation to submit the results of studies with Zontivity in one or more subsets of the paediatric population in prevention of arterial thromboembolism (see section 4.2 for information on paediatric use)
After oral administration of a single vorapaxar sulfate 2.5 mg dose, vorapaxar is rapidly absorbed and peak concentrations occur at a median tmax of 1 hour (range: 1 to 2) under fasted conditions. The mean absolute bioavailability of vorapaxar from the 2.5 mg dose of vorapaxar sulfate is 100%.
Ingestion of vorapaxar with a high-fat meal resulted in no meaningful change in AUC with a small (21%) decrease in Cmax and delayed tmax (45 minutes). Zontivity may be taken with or without food. Co-administration of an aluminium hydroxide/magnesium carbonate antacid or proton pump inhibitor (pantoprazole) did not affect vorapaxar AUC with only small decreases in Cmax. Therefore, Zontivity may be administered without regard to co-administration of agents that increase gastric pH (antacid or proton pump inhibitor).
The mean volume of distribution of vorapaxar is approximately 424 litres. Vorapaxar and the major circulating active metabolite, M20, are extensively bound (≥99%) to human plasma proteins. Vorapaxar is highly bound to human serum albumin and does not preferentially distribute into red blood cells.
Vorapaxar is eliminated by metabolism, with CYP3A4 and CYP2J2 responsible for formation of M20, its major active circulating metabolite, and M19, the predominant metabolite identified in excreta. The systemic exposure of M20 is ~20% of the exposure to vorapaxar.
The primary route of elimination is through the faeces, with approximately 91.5% of radiolabeled dose predicted to be recovered in the faeces compared to 8.5% in the urine. Vorapaxar is eliminated primarily in the form of metabolites, with no vorapaxar detected in urine. The apparent terminal half-life for vorapaxar is 187 hours (range 115-317 hours) and is similar for the active metabolite.
Vorapaxar exposure increases in an approximately dose-proportional manner following single doses of 1 to 40 mg and multiple doses of 0.5 to 2.5 mg of vorapaxar sulfate. The systemic pharmacokinetics of vorapaxar are linear with accumulation (6-fold) predictable from single- to multiple-dose data. Steady-state is achieved by 21 days following once-daily dosing.
The effects of renal (end-stage renal disease undergoing haemodialysis) and hepatic impairment on the pharmacokinetics of vorapaxar were evaluated in specific pharmacokinetic studies and are summarized below.
Pharmacokinetics of vorapaxar are similar between patients with end-stage renal disease (ESRD) undergoing haemodialysis and healthy subjects. Based on population pharmacokinetic analysis using data from healthy subjects and patients with atherosclerotic disease, vorapaxar mean AUC is estimated to be higher in patients with mild (17%) and moderate (34%) renal impairment compared to those with normal renal function; these differences are not considered to be clinically relevant. No dose adjustment is necessary for patients with renal impairment, including subjects with ESRD. There is limited therapeutic experience in patients with severe renal impairment or end stage renal disease. Therefore, Zontivity should be used with caution in such patients.
Pharmacokinetics of vorapaxar are similar between patients with mild (Child Pugh, 5 to 6 points) to moderate (Child Pugh, 7 to 9 points) hepatic impairment and healthy patients. Reduced hepatic function is a risk factor for bleeding and should be considered before initiating Zontivity. No dose adjustment is required for patients with mild hepatic impairment. Zontivity should be used with caution in patients with moderate hepatic impairment. Zontivity is contraindicated in patients with severe hepatic impairment (Child Pugh, 10 to 15 points) (see sections 4.3 and 4.4). Age, gender, weight and race were included as factors assessed in the population pharmacokinetic model to evaluate vorapaxar pharmacokinetics in healthy subjects and patients:
Pharmacokinetics of vorapaxar are similar between elderly, including those ≥75 years of age, and younger patients. No dose adjustment is necessary (see section 4.4).
The mean estimated vorapaxar Cmax and AUC were 30% and 32% higher, respectively, in females compared to males. These differences are not considered to be clinically relevant and no dose adjustment is necessary.
The mean estimated vorapaxar Cmax and AUC were 35% and 33% higher, respectively, in patients with a body weight of <60 kg compared to those weighing 60-100 kg. By comparison, vorapaxar exposure (AUC and Cmax) is estimated to be 19-21% lower in patients with a body weight of >100 kg compared to those weighing 60-100 kg. In general, a body weight <60 kg is a risk factor for bleeding. Zontivity should be used with caution in patients with a body weight <60 kg.
The mean estimated vorapaxar Cmax and AUC were 24% and 22% higher in Asian patients compared to that of Caucasians. Vorapaxar exposure (AUC and Cmax) in patients of African descent is estimated to be 17-19% lower compared to that of Caucasians. These differences are not considered to be clinically relevant and no dose adjustment is necessary.
In vitro metabolism studies demonstrate that vorapaxar is unlikely to cause clinically significant inhibition of human CYP1A2, CYP2B6, CYP3A, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. No clinically meaningful inhibition of CYP2B6, CYP3A, CYP2C19, or CYP2D6 by M20 is expected. In addition, no clinically meaningful inhibition of OATP1B1, OATP1B3, BCRP, OAT1, OAT3, and OCT2 by vorapaxar or M20 is anticipated. Based upon in vitro data, chronic administration of vorapaxar is unlikely to induce the metabolism of drugs metabolized by major CYP isoforms.
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity, carcinogenic potential, and fertility.
In repeat dose oral toxicity studies in rodents and monkeys, the principal treatment-related findings were urinary bladder and ureter hyperplasia in mice, hepatic vascular thrombi, lymphoid necrosis and retinal vacuolation in rats and phospholipidosis in all species. Phospholipidosis occurs at acceptable human to animal safety margins and was reversible. The clinical significance of this finding is currently unknown.
No defects were observed in embryo-foetal developmental studies in rats and rabbits at exposures sufficiently in excess of human exposure at the recommended human dose (RHD). Pre and postnatal studies in rats only showed some inconsistent developmental effects at exposures sufficiently in excess of human exposure at the RHD of 2.08 mg vorapaxar. The overall no effect level for the pre- and postnatal development effects was 5 mg/kg/day (6.8-times [female animals] the human steady-state exposure at 2.5 mg/day).
Vorapaxar had no effects on fertility of male and female rats at exposures sufficiently in excess of human exposure at the RHD.
Vorapaxar was not mutagenic or genotoxic in a battery of in vitro and in vivo studies.
Vorapaxar did not increase bleeding time in non-human primates when administered alone at 1 mg/kg. Bleeding time was prolonged slightly with administration of acetylsalicylic acid alone or in combination with vorapaxar. Acetylsalicylic acid, vorapaxar, and clopidogrel in combination produced significant prolongation of bleeding time. Transfusion of human platelet rich plasma normalised bleeding times with partial recovery of ex vivo platelet aggregation induced with arachidonic acid, but not induced with ADP or TRAP. Platelet poor plasma had no effect on bleeding times or platelet aggregation. (See section 4.4.)
No vorapaxar-related tumours were observed in 2-year rat and mouse studies at oral doses up to 30 mg/kg/day in rats and 15 mg/kg/day in mice (8.9 and 30 times the recommended therapeutic exposures in humans based on plasma exposure to vorapaxar for rats and mice, respectively).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.