ZYFLO Film-coated tablet Ref.[9902] Active ingredients:
Source: FDA, National Drug Code (US) Revision Year: 2020
2. Clinical Pharmacology
Mechanism of Action
Zileuton is a specific inhibitor of 5-lipoxygenase and thus inhibits leukotriene (LTB4, LTC4, LTD4, and LTE4) formation. Both the R(+) and S(-) enantiomers are pharmacologically active as 5-lipoxygenase inhibitors in in vitro systems. Leukotrienes are substances that induce numerous biological effects including augmentation of neutrophil and eosinophil migration, neutrophil and monocyte aggregation, leukocyte adhesion, increased capillary permeability, and smooth muscle contraction. These effects contribute to inflammation, edema, mucus secretion, and bronchoconstriction in the airways of asthmatic patients. Sulfido-peptide leukotrienes (LTC4, LTD4, LTE4, also known as the slow-releasing substances of anaphylaxis) and LTB4, a chemoattractant for neutrophils and eosinophils, can be measured in a number of biological fluids including bronchoalveolar lavage fluid (BALF) from asthmatic patients.
Zileuton is an orally active inhibitor of ex vivo LTB4 formation in several species, including dogs, monkeys, rats, sheep, and rabbits. Zileuton inhibits arachidonic acid-induced ear edema in mice, neutrophil migration in mice in response to polyacrylamide gel, and eosinophil migration into the lungs of antigen-challenged sheep.
Zileuton inhibits leukotriene-dependent smooth muscle contractions in vitro in guinea pig and human airways. The compound inhibits leukotriene-dependent bronchospasm in antigen and arachidonic acid-challenged guinea pigs. In antigen-challenged sheep, zileuton inhibits late-phase bronchoconstriction and airway hyperreactivity. In humans, pretreatment with zileuton attenuated bronchoconstriction caused by cold air challenge in patients with asthma.
Pharmacokinetics
Zileuton is rapidly absorbed upon oral administration with a mean time to peak plasma concentration (Tmax) of 1.7 hours and a mean peak level (Cmax) of 4.98 μg/mL. The absolute bioavailability of ZYFLO is unknown. Systemic exposure (mean AUC) following 600 mg ZYFLO administration is 19.2 μg.hr/mL. Plasma concentrations of zileuton are proportional to dose, and steady-state levels are predictable from single-dose pharmacokinetic data. Administration of ZYFLO with food resulted in a small but statistically significant increase (27%) in zileuton Cmax without significant changes in the extent of absorption (AUC) or Tmax. Therefore, ZYFLO can be administered with or without food (see DOSAGE AND ADMINISTRATION).
The apparent volume of distribution (V/F) of zileuton is approximately 1.2 L/kg. Zileuton is 93% bound to plasma proteins, primarily to albumin, with minor binding to αl-acid glycoprotein.
Elimination of zileuton is predominantly via metabolism with a mean terminal half-life of 2.5 hours. Apparent oral clearance of zileuton is 7.0 mL/min/kg. ZYFLO activity is primarily due to the parent drug. Studies with radiolabeled drug demonstrated that orally administered zileuton is well absorbed into the systemic circulation with 94.5% and 2.2% of the radiolabeled dose recovered in urine and feces, respectively. Several zileuton metabolites have been identified in human plasma and urine. These include two diastereomeric O-glucuronide conjugates (major metabolites) and an N-dehydroxylated metabolite of zileuton. The urinary excretion of the inactive N-dehydroxylated metabolite and unchanged zileuton each accounted for less than 0.5% of the dose. In vitro studies utilizing human liver microsomes have shown that zileuton and its N-dehydroxylated metabolite can be oxidatively metabolized by the cytochrome P450 isoenzymes 1A2, 2C9 and 3A4 (CYP1A2, CYP2C9 and CYP3A4).
Special populations
Effect of age
The pharmacokinetics of zileuton were investigated in healthy elderly volunteers (ages 65 to 81 years, 9 males, 9 females) and healthy young volunteers (ages 20 to 40 years, 5 males and 4 females) after single and multiple oral doses of 600 mg every 6 hours of zileuton. Zileuton pharmacokinetics were similar in healthy elderly subjects (≥65 years) compared to healthy younger adults (18 to 40 years).
Effect of gender
Across several studies, no significant gender effects were observed on the pharmacokinetics of zileuton.
Renal insufficiency
The pharmacokinetics of zileuton were similar in healthy subjects and in subjects with mild, moderate, and severe renal insufficiency. In subjects with renal failure requiring hemodialysis, zileuton pharmacokinetics were not altered by hemodialysis and a very small percentage of the administered zileuton dose (<0.5%) was removed by hemodialysis. Hence, dosing adjustment in patients with renal dysfunction or undergoing hemodialysis is not necessary.
Hepatic insufficiency
ZYFLO is contraindicated in patients with active liver disease (see CONTRAINDICATIONS and PRECAUTIONS, Hepatic).
6.6. Carcinogenesis, Mutagenesis, Impairment of Fertility
In 2-year carcinogenicity studies, increases in the incidence of liver, kidney, and vascular tumors in female mice and a trend towards an increase in the incidence of liver tumors in male mice were observed at 450 mg/kg/day (providing approximately 4 times [females] or 7 times [males] the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose). No increase in the incidence of tumors was observed at 150 mg/kg/day (providing approximately 2 times the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose). In rats, an increase in the incidence of kidney tumors was observed in both sexes at 170 mg/kg/day (providing approximately 6 times [males] or 14 times [females] the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose). No increased incidence of kidney tumors was seen at 80 mg/kg/day (providing approximately 4 times [males] or 6 times [females] the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose). Although a dose-related increased incidence of benign Leydig cell tumors was observed, Leydig cell tumorigenesis was prevented by supplementing male rats with testosterone.
Zileuton was negative in genotoxicity studies including bacterial reverse mutation (Ames) using S. typhimurium and E. coli, chromosome aberration in human lymphocytes, in vitro unscheduled DNA synthesis (UDS), in rat hepatocytes with or without zileuton pretreatment and in mouse and rat kidney cells with zileuton pretreatment, and mouse micronucleus assays. However, a dose-related increase in DNA adduct formation was reported in kidneys and livers of female mice treated with zileuton. Although some evidence of DNA damage was observed in a UDS assay in hepatocytes isolated from Aroclor-1254 treated rats, no such finding was noticed in hepatocytes isolated from monkeys, where the metabolic profile of zileuton is more similar to that of humans.
In reproductive performance/fertility studies, zileuton produced no effects on fertility in rats at oral doses up to 300 mg/kg/day (providing approximately 8 times [male rats] and 18 times [female rats] the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose). Comparative systemic exposure (AUC) is based on measurements in male rats or nonpregnant female rats at similar dosages. However, reduction in fetal implants was observed at oral doses of 150 mg/kg/day and higher (providing approximately 9 times the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose). Increases in gestation length, prolongation of estrous cycle, and increases in stillbirths were observed at oral doses of 70 mg/kg/day and higher (providing approximately 4 times the systemic exposure (AUC) achieved at the maximum recommended human daily oral dose). In a perinatal/postnatal study in rats, reduced pup survival and growth were noted at an oral dose of 300 mg/kg/day (providing approximately 18 times the systemic exposure [AUC] achieved at the maximum recommended human daily oral dose).
13. Clinical Studies
Two double-blind, parallel, placebo-controlled, multi-center studies have established the efficacy of ZYFLO in the treatment of asthma. Three hundred seventy-three (373) patients were enrolled in the 6-month, double-blind phase of Study 1, and 401 patients were enrolled in the 3-month double-blind phase of Study 2. In these studies, the patients were mild-to-moderate asthmatics who had a mean baseline FEV1 of approximately 2.3 liters and who used inhaled beta-agonists as needed, the mean being approximately 6 puffs of albuterol per day from a metered-dose inhaler. In each study, patients were randomized to receive either ZYFLO 400 mg four times daily, ZYFLO 600 mg four times daily, or placebo. Only the ZYFLO 600 mg four times daily dosage regimen was shown to be efficacious by demonstrating statistically significant improvement across several parameters.
Efficacy endpoints measured in Study 1 are shown in Table 1 below as mean change from baseline to the end of the study (six months). Statistically significant differences from placebo at the p<0.05 level are indicated by an asterisk (*). Similar results were observed after three months in Study 2.
Table 1. Mean Change From Baseline To End Of Study (Six-month study):
| Efficacy Endpoint | ZYFLO 600 mg 4 times/day | Placebo |
|---|---|---|
| Through FEV1 (L) | 0.27 | 0.14 |
| AM PEFR (L/min) | 30.60* | 5.04 |
| PM PEFR (L/min) | 24.59* | 7.98 |
| β-Agonist Use (puffs/day) | -1.77* | -0.22 |
| Daily Symptom Score (0-3 Scale) | -0.49* | -0.28 |
| Nocturnal Symptom Score (0-3 Scale) | -0.29* | -0.04 |
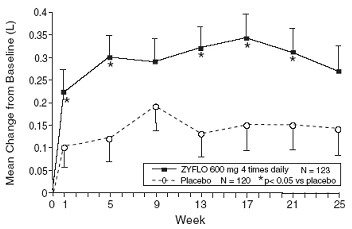
Figure 1 shows the mean effect of ZYFLO versus placebo for the primary efficacy variable, trough FEV 1, over the course of Study 1.
Figure 1. Mean Change From Baseline To Through FEV1 (L):
Of all the patients in Study 1 and Study 2, 7.0% of those administered ZYFLO 600 mg four times daily required systemic corticosteroid therapy for exacerbation of asthma, whereas 18.7% of the placebo group required corticosteroid treatment. This difference was statistically significant.
In these trials, there was a statistically significant improvement from baseline in FEV1, which occurred 2 hours after initial administration of ZYFLO. This mean increase was approximately 0.10 L greater than that in placebo-treated patients.
These studies evaluated patients receiving as-needed inhaled beta-agonist as their only asthma therapy. In this patient population, post-hoc analyses suggested that individuals with lower FEV1 values at baseline showed a greater improvement.
The role of ZYFLO in the management of patients with more severe asthma, patients receiving anti-asthma therapy other than as-needed, inhaled beta-agonists, or patients receiving it as an oral or inhaled corticosteroid-sparing agent remains to be fully characterized.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.