Efgartigimod alfa
Mechanism of action
Efgartigimod alfa is a human IgG1 antibody fragment engineered for increased affinity to the neonatal Fc Receptor (FcRn). Efgartigimod alfa binds to FcRn, resulting in a reduction in the levels of circulating IgG including pathogenic IgG autoantibodies. Efgartigimod alfa does not affect the levels of other immunoglobulins (IgA, IgD, IgE or IgM), and does not reduce those of albumin.
IgG autoantibodies are the underlying cause of the pathogenesis of IgG mediated autoimmune diseases.
In Myasthenia Gravis (MG) these impair neuromuscular transmission by binding to acetylcholine receptors (AChR), musclespecific tyrosine kinase (MuSK) or low density lipoprotein receptor-related protein 4 (LRP4).
In chronic inflammatory demyelinating polyneuropathy (CIDP), several lines of evidence point to the key role of IgG autoantibodies in the pathogenesis of this disease. This includes the demonstration of autoreactive IgG antibodies against components of myelinated nerves, passive transfer of CIDP symptoms to animal models using sera or IgG's from patients with CIDP, and the therapeutic effect of plasma exchange and immunoadsorption for treating patients with CIDP.
Pharmacodynamic properties
Intravenous formulation
In the ARGX-113-1704 double-blind placebo-controlled study in gMG patients, efgartigimod alfa 10 mg/kg administered once weekly for 4 weeks decreased serum IgG levels and AChR autoantibody (AChRAb) levels. Maximum mean percentage decrease in total IgG levels compared to baseline reached 61% one week after the last infusion of the initial treatment cycle and returned to baseline levels 9 weeks after the last infusion. Similar effects were also observed for all subtypes of IgG. Decrease in AChR-Ab levels followed a similar time course with maximum mean percentage decrease of 58% one week after the last infusion and return to baseline levels 7 weeks after the last infusion. Similar changes were observed during the second cycle of the study.
Subcutaneous formulation
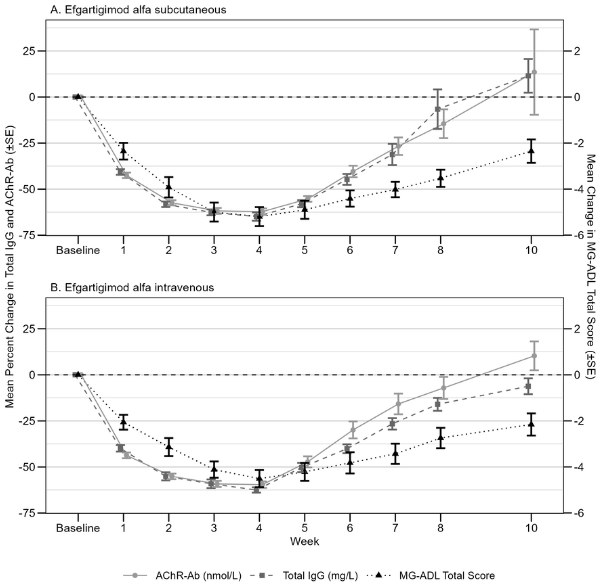
In the ARGX-113-2001 study, decreases in AChR-Ab levels followed a comparable time course as total IgG levels and were similar between the efgartigimod alfa subcutaneous and intravenous groups. Maximum mean percentage decreases in AChR-Ab levels of 62.2% and 59.6% were observed one week after the last administration in the efgartigimod alfa subcutaneous and intravenous groups, respectively. For both the efgartigimod alfa subcutaneous and intravenous groups, decrease in total IgG and AChR-Ab levels were associated with a clinical response, as measured by the change from baseline in MG-ADL total score (see figure 1).
Figure 1. Relationship between total IgG and AChR-Ab and MG-ADL total score in AChR-Ab seropositive population treated with efgartigimod alfa subcutaneous (1A) and efgartigimod alfa intravenous (1B) (study ARGX-113-2001):
In the ARGX-113-1802 study in patients with CIDP receiving continuous once-weekly administration of efgartigimod alfa subcutaneous at 1 000 mg, the mean percent change from baseline in total IgG levels was sustained from Week 4 throughout the treatment period (mean percentage reduction from baseline ranging between 66.8 to 71.6%).
Pharmacokinetic properties
Absorption
Based upon population PK data analysis, the estimated bioavailability with efgartigimod alfa 1 000 mg subcutaneous is 77%.
The mean Ctrough after 4 once weekly administrations with efgartigimod alfa 1 000 mg subcutaneous and efgartigimod alfa 10 mg/kg intravenous were 22.0 μg/mL (37% CV) and 14.9 μg/mL (43% CV), respectively. The AUC0-168h of efgartigimod alfa after administration of one treatment cycle with 1 000 mg subcutaneous and 10 mg/kg intravenous were comparable.
In patients receiving continuous subcutaneous administration of efgartigimod alfa 1 000 mg once weekly, mean Ctrough ranged from 14.9 to 20.1 μg/mL.
Distribution
Based upon population PK data analysis in healthy subjects and patients the volume of distribution is 18 L.
Biotransformation
Efgartigimod alfa is expected to be degraded by proteolytic enzymes into small peptides and amino acids.
Elimination
The terminal half-life is 80 to 120 hours (3 to 5 days). Based upon population PK data analysis, the clearance is 0.128 L/h. The molecular weight of efgartigimod alfa is approximately 54 kDa, which is at the boundary of molecules that are renally filtered.
Linearity/non-linearity
The pharmacokinetics profile of efgartigimod alfa is linear, independent of dose or time, with negligible accumulation. The geometric mean accumulation ratio based on observed peak concentrations was 1.12.
Special populations
Age, gender, race and bodyweight
The pharmacokinetics of efgartigimod alfa were not affected by age (19-78 years), gender and race.
A population pharmacokinetic analysis showed that the effect of bodyweight on efgartigimod alfa exposure was limited at a dose of 10 mg/kg in patients up to 120 kg as well as in patients of 120 kg and above who received a capped dose of 1 200 mg/infusion. There was no effect of bodyweight on the extent of IgG reduction. In the double-blind placebo-controlled study, 5 (3%) patients were over 120 kg. The median bodyweight of patients on efgartigimod alfa in the study was 76.5 kg (min 49; max 229).
Renal impairment
No dedicated pharmacokinetic studies have been performed in patients with renal impairment.
The effect of renal function marker estimated glomerular filtration rate [eGFR] as a covariate in a population pharmacokinetic analysis showed a reduced clearance resulting in a limited increase in exposure in patients with mild renal impairment (eGFR 60-89 mL/min/1.73 m²). No specific dose adjustment is recommended in patients with mild renal impairment.
There is insufficient data on the impact of moderate renal impairment (eGFR 30-59 mL/min/1.73 m²) and severe renal impairment (eGFR <30 mL/min/1.73 m²) on efgartigimod alfa pharmacokinetic parameters.
Hepatic impairment
No dedicated pharmacokinetic study has been performed in patients with hepatic impairment.
The effect of hepatic function markers as covariates in a population pharmacokinetic analysis did not show any impact on the pharmacokinetics of efgartigimod alfa.
Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology and repeated dose toxicity.
In reproduction studies in rats and rabbits, intravenous administration of efgartigimod alfa did not result in adverse effects on fertility and pregnancy nor were teratogenic effects observed up to dose levels corresponding to 11-fold (rats) and 56-fold (rabbits) to the exposure (AUC) at the maximum recommended therapeutic dose.
Carcinogenicity and genotoxicity
No studies have been conducted to assess the carcinogenic and genotoxic potential of efgartigimod alfa.
Related medicines
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.