Uridine triacetate
Chemical formula: C₁₅H₁₈N₂O₉ Molecular mass: 370.314 g/mol PubChem compound: 20058
Mechanism of action
Uridine triacetate is an acetylated form of uridine. Following oral administration, uridine triacetate is deacetylated by nonspecific esterases present throughout the body, yielding uridine in the circulation (Figure 1).
Figure 1. Uridine Triacetate Conversion to Uridine:
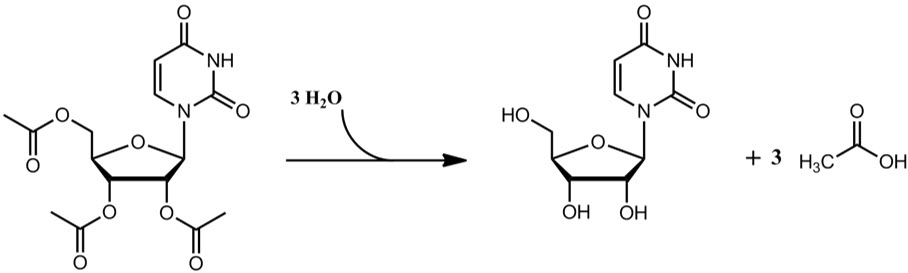
Uridine triacetate is provided in the systemic circulation of patients with hereditary orotic aciduria who cannot synthesize adequate quantities of uridine due to a genetic defect in uridine nucleotide synthesis.
Pharmacodynamic properties
Hereditary orotic aciduria (uridine monophosphate synthase deficiency) is a rare congenital autosomal recessive disorder of pyrimidine metabolism caused by a defect in uridine monophosphate synthase (UMPS). The UMPS gene encodes uridine 5′monophosphate synthase, a bifunctional enzyme that catalyzes the final two steps of the de novo pyrimidine biosynthetic pathway in mammalian cells.
The defect in UMP synthase in hereditary orotic aciduria has two primary biochemical consequences. First, the blockade of de novo UMP synthesis results in a systemic deficiency of pyrimidine nucleotides, accounting for most clinical consequences of the disease. Second, orotic acid from the de novo pyrimidine pathway that cannot be converted to UMP is excreted in the urine, accounting for the common name of the disorder, orotic aciduria. Orotic acid crystals in the urine can cause episodes of obstructive uropathy.
Uridine triacetate delivered into the circulation, it can be used by essentially all cells to make uridine nucleotides, compensating for the genetic deficiency in synthesis in patients with hereditary orotic aciduria. When intracellular uridine nucleotides are restored into the normal range, overproduction of orotic acid is reduced by feedback inhibition, so that urinary excretion of orotic acid is also reduced.
Pharmacokinetic properties
Absorption
Uridine triacetate delivers 4- to 6-fold more uridine into the systemic circulation compared to equimolar doses of uridine itself. Maximum concentrations of uridine in plasma following oral uridine triacetate are generally achieved within 2 to 3 hours, and the half-life ranges from approximately 2 to 2.5 hours.
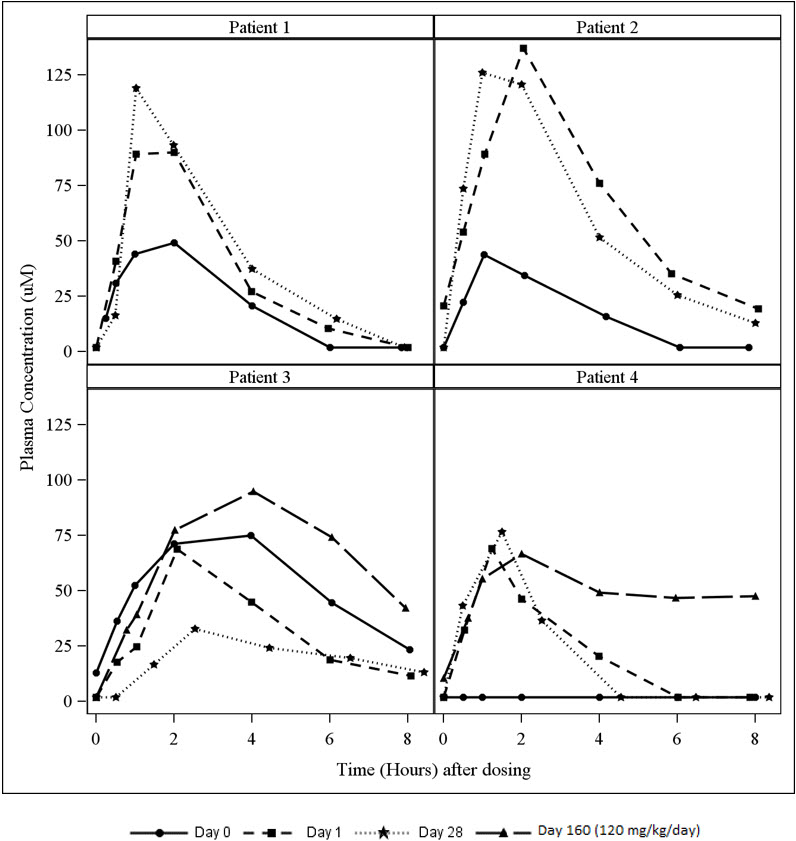
A study in patients with hereditary orotic aciduria included an assessment of plasma uridine pharmacokinetics in 4 patients. Three of the patients were previously treated with oral uridine. On Day 0 (baseline), these three patients received their usual daily dose of oral uridine as a single dose (150 to 200 mg/kg once daily) and on Day 1, initiated oral uridine triacetate treatment (60 mg/kg once daily). A fourth patient was enrolled who was naïve to uridine replacement therapy. The dose of uridine triacetate was increased on Day 116 to 120 mg/kg once daily in two patients (Patients 3 and 4) and plasma uridine concentrations were assessed on Day 160 (44 days after the dose increase).
Plasma uridine levels in all four patients are depicted in Figure 2. Pharmacokinetic parameters are summarized in Table 1. Mean exposure to plasma uridine as assessed by Cmax and AUC was greater after oral uridine triacetate than after oral uridine (approximately 4-fold on an equiweight basis, and 6-fold on an equimolar basis), although individual differences in relative bioavailability were noted. Plasma concentrations of the uridine catabolite uracil were generally below the limit of quantitation in all patients.
Table 1. Pharmacokinetic Parameters for Plasma Uridine*:
| Pharmacokinetic Parameters (Plasma Uridine) | Day 0 (Baseline) (Oral Uridine, 150 to 200 mg/kg once daily) N=3* | Day 1 (Oral Uridine triacetate, 60 mg/kg once daily) N=4 | Day 28 (Oral Uridine triacetate, 60 mg/kg once daily) N=4 | Day 160 (Oral Uridine triacetate, 120 mg/kg once daily) N=2† |
|---|---|---|---|---|
| Cmax (µM) mean ± SD | 56.0 ± 16.6 | 91.3 ± 32.2 | 88.7 ± 43.2 | 80.9 ± 20.0 |
| Tmax (hours) median (range‡) | 2.0 (1.0, 4.0) | 2.0 (1.2, 2.1) | 1.3 (1.0, 2.5) | 3.0 (2.0, 4.0) |
| t½ (hours) mean ± SD | 1.6 ± 0.7 | 1.6 ± 0.6 | 2.3 ± 1.6 | 8.2 ± 6.8 |
| AUC(0-8) (µM∙hr) mean ± SD | 238.0 ± 163.2 | 311.2 ± 153.3 | 278.7 ± 148.5 | 465.6 ± 95.3 |
* Data shown are from patients previously treated with oral uridine
† The dose of uridine triacetate was increased on Day 116 to 120 mg/kg per day. Serial plasma samples were taken on Day 160 (4 4 days after the dose increase) for plasma uridine levels.
‡ Tmax range is expressed as the minimum and maximum values obtained
Figure 2. Plasma Uridine Following Oral Administration of Uridine (Day 0) or Uridine triacetate (Days 1, 28 and 160) in Patients with Hereditary Orotic Aciduria:
Food Effect on Uridine PK
A study in healthy adult subjects receiving a slightly different formulation of uridine triacetate granules (6 gram dose) under fed and fasted conditions showed no difference in the overall rate and extent of uridine exposure.
Distribution
Circulating uridine is taken up into mammalian cells via specific nucleoside transporters, and also crosses the blood brain barrier.
Excretion
Uridine can be excreted via the kidneys, but is also metabolized by normal pyrimidine catabolic pathways present in most tissues.
Drug Interaction Studies
In vitro enzyme inhibition data did not reveal meaningful inhibitory effects of uridine triacetate or uridine on CYP3A4, CYP1A2, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and CYP2E1. In vitro enzyme induction data did not reveal an inducing effect of uridine triacetate or uridine on CYP1A2, CYP2B6, or CYP3A4.
In vitro data showed that uridine triacetate was a weak substrate for P-glycoprotein. Uridine triacetate inhibited the transport of a known P-glycoprotein substrate, digoxin, with an IC50 of 344 µM. Due to the potential for high local (gut) concentrations of the drug after dosing, the interaction of uridine triacetate with orally administered P-gp substrate drugs cannot be ruled out.
In vivo data in humans are not available.
Related medicines
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.