MabCampath 30mg/ml concentrate for solution for infusion Ref.[2469] Active ingredients: Alemtuzumab
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2012 Publisher: Genzyme Europe BV Gooimeer 10 1411 DD Naarden Netherlands
Pharmacodynamic properties
Pharmacotherapeutic group: Antineoplastic agents, monoclonal antibodies
ATC code: L01XC04
Alemtuzumab is a genetically engineered humanised IgG1 kappa monoclonal antibody specific for a 21-28 kD lymphocyte cell surface glycoprotein (CD52) expressed primarily on the surface of normal and malignant peripheral blood B and T cell lymphocytes. Alemtuzumab was generated by the insertion of six complementarity-determining regions from an IgG2a rat monoclonal antibody into a human IgG1 immunoglobulin molecule.
Alemtuzumab causes the lysis of lymphocytes by binding to CD52, a highly expressed, non-modulating antigen which is present on the surface of essentially all B and T cell lymphocytes as well as monocytes, thymocytes and macrophages. The antibody mediates the lysis of lymphocytes via complement fixation and antibody-dependent cell mediated cytotoxicity. The antigen has been found on a small percentage (< 5%) of granulocytes, but not on erythrocytes or platelets. Alemtuzumab does not appear to damage haematopoietic stem cells or progenitor cells.
First line B-CLL patients
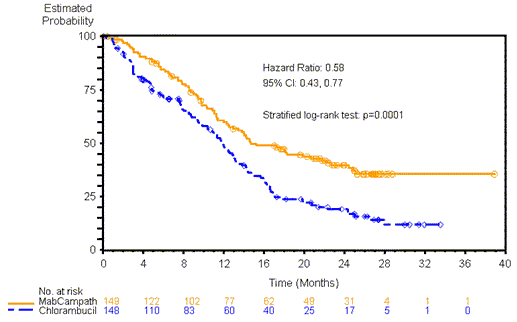
The safety and efficacy of MabCampath were evaluated in a Phase 3, open-label, randomized comparative trial of first line (previously untreated) Rai stage I-IV B-CLL patients requiring therapy (Study 4). MabCampath was shown to be superior to chlorambucil as measured by the primary endpoint progression free survival (PFS) (see Figure 1).
Figure 1: Progression free survival in first line study (by treatment group)
The secondary objectives included complete response (CR) and overall response (CR or partial response) rates using the 1996 NCIWG criteria, the duration of response, time to alternative treatment and safety of the two treatment arms.
Summary of first-line patient population and outcomes
| Independent review of response rate and duration | |||
|---|---|---|---|
| MabCampath n=149 | Chlorambucil n=148 | P value | |
| Median Age (Years) | 59 | 60 | Not Applicable |
| Rai Stage III/IV Disease | 33.6% | 33.1% | Not Applicable |
| Overall Response Rate | 83.2% | 55.4% | <0.0001* |
| Complete Response | 24.2% | 2.0% | <0.0001* |
| MRD negative**** | 7.4% | 0.0% | 0.0008* |
| Partial Response | 59.1% | 53.4% | Not Applicable |
| Duration of Response**, CR or PR (Months) | N=124 16.2 | N=82 12.7 | Not Applicable |
| K-M median (95% Confidence Interval) | (11.5, 23.0) | (10.2, 14.3) | |
| Time to Alternative Treatment (Months) | 23.3 | 14.7 | 0.0001*** |
| K-M median (95% Confidence Interval) | (20.7, 31.0) | (12.6, 16.8) | |
* Pearson chi-square test or Exact test
** Duration of best response
*** log-rank test stratified by Rai group (Stage I-II vs III-IV)
**** by 4-colour flow
Cytogenetic Analyses in first line B-CLL patients
The cytogenetic profile of B-CLL has been increasingly recognized as providing important prognostic information and may predict response to certain therapies. Of the first-line patients (n=282) in whom baseline cytogenetic (FISH) data were available in Study 4, chromosomal aberrations were detected in 82%, while normal karyotype was detected in 18%. Chromosomal aberrations were categorized according to Döhner's hierarchical model. In first line patients, treated with either MabCampath or chlorambucil, there were 21 patients with the 17p deletion, 54 patients with 11q deletion, 34 patients with trisomy 12, 51 patients with normal karyotype and 67 patients with sole 13q deletion.
ORR was superior in patients with any 11q deletion (87% v 29%; p<0.0001) or sole deletion 13q (91% v 62%; p=0.0087) treated with MabCampath compared to chlorambucil. A trend toward improved ORR was observed in patients with 17p deletion treated with MabCampath (64% v 20%; p=0.0805). Complete remissions were also superior in patients with sole 13q deletion treated with MabCampath (27% v 0%; p=0.0009). Median PFS was superior in patients with sole 13q deletion treated with MabCampath (24.4 v 13.0 months; p=0.0170 stratified by Rai Stage). A trend towards improved PFS was observed in patients with 17p deletion, trisomy 12 and normal karyotype, which did not reach significance due to small sample size.
Assessment of CMV by PCR
In the randomized controlled trial in first line patients (Study 4), patients in the MabCampath arm were tested weekly for CMV using a PCR (polymerase chain reaction) assay from initiation through completion of therapy, and every 2 weeks for the first 2 months following therapy. In this study, asymptomatic positive PCR only for CMV was reported in 77/147 (52.4%) of MabCampath-treated patients; symptomatic CMV infection was reported less commonly in 23/147 MabCampath treated patients (16%). In the MabCampath arm 36/77 (46.8%) of patients with asymptomatic PCR positive CMV received antiviral therapy and 47/77 (61%) of these patients had MabCampath therapy interrupted. The presence of asymptomatic positive PCR for CMV or symptomatic PCR positive CMV infection during treatment with MabCampath had no measurable impact on progression free survival (PFS).
Previously treated B-CLL patients
Determination of the efficacy of MabCampath is based on overall response and survival rates. Data available from three uncontrolled B-CLL studies are summarised in the following table:
| Efficacy parameters | Study 1 | Study 2 | Study 3 |
|---|---|---|---|
| Number of Patients | 93 | 32 | 24 |
| Diagnostic Group | B-CLL pts who had received an alkylating agent and had failed fludarabine | B-CLL pts who had failed to respond or relapsed following treatment with conventional chemotherapy | B-CLL (plus a PLL) pts who had failed to respond or relapsed following treatment with fludarabine |
| Median Age (years) | 66 | 57 | 62 |
| Disease Characteristics (%) | |||
| Rai Stage III/IV | 76 | 72 | 71 |
| B Symptoms 42 | 31 | 21 | |
| Prior Therapies (%) | |||
| Alkylating Agents | 100 | 100 | 92 |
| Fludarabine | 100 | 34 | 100 |
| Number of Prior Regimens (range) | 3 (2-7) | 3 (1-10) | 3 (1-8) |
| Initial Dosing Regimen | Gradual escalation from 3 to 10 to 30 mg | Gradual escalation from 10 to 30 mg | Gradual escalation from 10 to 30 mg |
| Final Dosing Regimen | 30 mg iv 3 x weekly | 30 mg iv 3 x weekly | 30 mg iv 3 x weekly |
| Overall Response Rate (%) | 33 | 21 | 29 |
| (95% Confidence Interval) | (23-43) | (8-33) | (11-47) |
| Complete Response | 2 | 0 | 0 |
| Partial Response | 31 | 21 | 29 |
| Median Duration of Response (months) | 7 | 7 | 11 |
| (95% Confidence Interval) | (5-8) | (5-23) | (6-19) |
| Median time to Response (months) | 2 | 4 | 4 |
| (95% Confidence Interval) | (1-2) | (1-5) | (2-4) |
| Progression-Free Survival (months) | 4 | 5 | 7 |
| (95% Confidence Interval) | (3-5) | (3-7) | (3-9) |
| Survival (months): | |||
| (95% Confidence Interval) | |||
| All patients | 16 (12-22) | 26 (12-44) | 28 (7-33) |
| Responders | 33 (26-NR) | 44 (28-NR) | 36 (19-NR) |
NR = not reached
Pharmacokinetic properties
Pharmacokinetics were characterised in MabCampath-naive patients with B-cell chronic lymphocytic leukaemia (B-CLL) who had failed previous therapy with purine analogues. MabCampath was administered as a 2 hour intravenous infusion, at the recommended dosing schedule, starting at 3 mg and increasing to 30 mg, 3 times weekly, for up to 12 weeks. MabCampath pharmacokinetics followed a 2-compartment model and displayed non-linear elimination kinetics. After the last 30 mg dose, the median volume of distribution at steady-state was 0.15 l/kg (range: 0.1-0.4 l/kg), indicating that distribution was primarily to the extracellular fluid and plasma compartments. Systemic clearance decreased with repeated administration due to decreased receptor-mediated clearance (i.e. loss of CD52 receptors in the periphery). With repeated administration and consequent plasma concentration accumulation, the rate of elimination approached zero-order kinetics. As such, half-life was 8 hours (range: 2-32 hours) after the first 30 mg dose and was 6 days (range: 1-14 days) after the last 30 mg dose. Steady-state concentrations were reached after about 6 weeks of dosing. No apparent difference in pharmacokinetics between males and females was observed nor was any apparent age effect observed.
Preclinical safety data
Preclinical evaluation of alemtuzumab in animals has been limited to the cynomolgus monkey because of the lack of expression of the CD52 antigen on non-primate species.
Lymphocytopenia was the most common treatment-related effect in this species. A slight cumulative effect on the degree of lymphocyte depletion was seen in repeated dose studies compared to single dose studies. Lymphocyte depletion was rapidly reversible after cessation of dosing. Reversible neutropenia was seen following daily intravenous or subcutaneous dosing for 30 days, but not following single doses or daily dosing for 14 days. Histopathology results from bone marrow samples revealed no remarkable changes attributable to treatment. Single intravenous doses of 10 and 30 mg/kg produced moderate to severe dose related hypotension accompanied by a slight tachycardia.
MabCampath Fab binding was observed in lymphoid tissues and the mononuclear phagocyte system. Significant Fab binding was also observed in the male reproductive tract (epididymis, sperm, seminal vesicle) and the skin.
No other findings, in the above toxicity studies, provide information of significant relevance to clinical use.
No short or long term animal studies have been conducted with MabCampath to assess carcinogenic and mutagenic potential.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.