ADDERALL XR Extended-release capsule Ref.[50505] Active ingredients: Amfetamine Dexamfetamine
Source: FDA, National Drug Code (US) Revision Year: 2022
12.1. Mechanism of Action
Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The mode of therapeutic action in ADHD is not known.
12.2. Pharmacodynamics
Amphetamines block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space.
12.3. Pharmacokinetics
Pharmacokinetic studies of ADDERALL XR have been conducted in healthy adult and pediatric (children aged 6-12 yrs) subjects, and adolescent (13-17 yrs) and children with ADHD. Both ADDERALL (immediate-release) tablets and ADDERALL XR extended release capsules contain d-amphetamine and l-amphetamine salts in the ratio of 3:1. Following administration of ADDERALL (immediate-release), the peak plasma concentrations occurred in about 3 hours for both d-amphetamine and l-amphetamine.
The time to reach maximum plasma concentration (Tmax) for ADDERALL XR is about 7 hours, which is about 4 hours longer compared to ADDERALL (immediate-release). This is consistent with the extended-release nature of the product.
Figure 1. Mean d-amphetamine and l-amphetamine Plasma Concentrations Following Administration of ADDERALL XR 20 mg (8 am) and ADDERALL (immediate-release) 10 mg Twice Daily (8 am and 12 noon) in the Fed State:
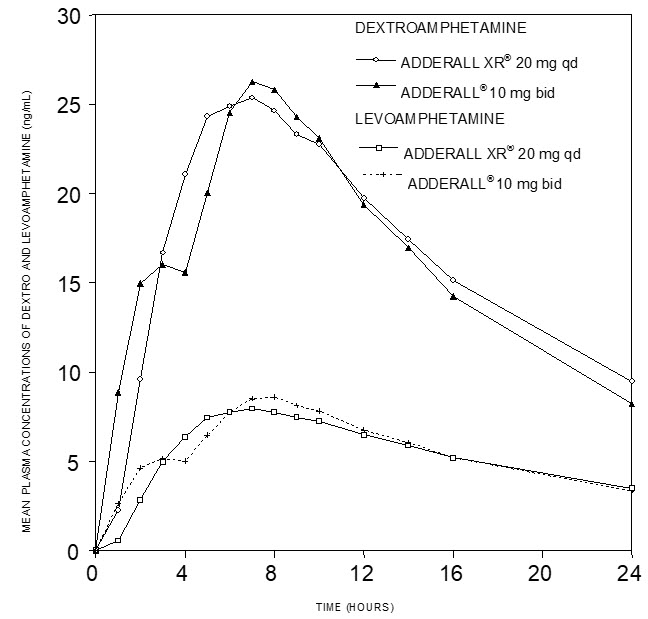
A single dose of ADDERALL XR 20 mg extended release capsules provided comparable plasma concentration profiles of both d-amphetamine and l-amphetamine to ADDERALL (immediate-release) 10 mg twice daily administered 4 hours apart.
The mean elimination half-life for d-amphetamine is 10 hours in adults; 11 hours in adolescents aged 13-17 years and weighing less than or equal to 75 kg/165 lbs; and 9 hours in children aged 6 to 12 years. For the l-amphetamine, the mean elimination half-life in adults is 13 hours; 13 to 14 hours in adolescents; and 11 hours in children aged 6 to 12 years. On a mg/kg body weight basis, children have a higher clearance than adolescents or adults (see Special Populations below).
ADDERALL XR demonstrates linear pharmacokinetics over the dose range of 20 to 60 mg in adults and adolescents weighing greater than 75 kg/165 lbs, over the dose range of 10 to 40 mg in adolescents weighing less than or equal to 75 kg/165 lbs, and 5 to 30 mg in children aged 6 to 12 years. There is no unexpected accumulation at steady state in children.
Food does not affect the extent of absorption of d-amphetamine and l-amphetamine, but prolongs Tmax by 2.5 hours (from 5.2 hrs at fasted state to 7.7 hrs after a high-fat meal) for d-amphetamine and 2.7 hours (from 5.6 hrs at fasted state to 8.3 hrs after a high fat meal) for l-amphetamine after administration of ADDERALL XR 30 mg. Opening the capsule and sprinkling the contents on applesauce results in comparable absorption to the intact capsule taken in the fasted state. Equal doses of ADDERALL XR strengths are bioequivalent.
Metabolism and Excretion
Amphetamine is reported to be oxidized at the 4 position of the benzene ring to form 4-hydroxyamphetamine, or on the side chain α or β carbons to form alpha-hydroxy-amphetamine or norephedrine, respectively. Norephedrine and 4-hydroxy-amphetamine are both active and each is subsequently oxidized to form 4-hydroxy-norephedrine. Alpha-hydroxy-amphetamine undergoes deamination to form phenylacetone, which ultimately forms benzoic acid and its glucuronide and the glycine conjugate hippuric acid. Although the enzymes involved in amphetamine metabolism have not been clearly defined, CYP2D6 is known to be involved with formation of 4-hydroxy-amphetamine. Since CYP2D6 is genetically polymorphic, population variations in amphetamine metabolism are a possibility.
Amphetamine is known to inhibit monoamine oxidase, whereas the ability of amphetamine and its metabolites to inhibit various P450 isozymes and other enzymes has not been adequately elucidated. In vitro experiments with human microsomes indicate minor inhibition of CYP2D6 by amphetamine and minor inhibition of CYP1A2, 2D6, and 3A4 by one or more metabolites. However, due to the probability of auto-inhibition and the lack of information on the concentration of these metabolites relative to in vivo concentrations, no predications regarding the potential for amphetamine or its metabolites to inhibit the metabolism of other drugs by CYP isozymes in vivo can be made.
With normal urine pHs, approximately half of an administered dose of amphetamine is recoverable in urine as derivatives of alpha-hydroxy-amphetamine and approximately another 30-40% of the dose is recoverable in urine as amphetamine itself. Since amphetamine has a pKa of 9.9, urinary recovery of amphetamine is highly dependent on pH and urine flow rates. Alkaline urine pHs result in less ionization and reduced renal elimination, and acidic pHs and high flow rates result in increased renal elimination with clearances greater than glomerular filtration rates, indicating the involvement of active secretion. Urinary recovery of amphetamine has been reported to range from 1% to 75%, depending on urinary pH, with the remaining fraction of the dose hepatically metabolized. Consequently, both hepatic and renal dysfunction have the potential to inhibit the elimination of amphetamine and result in prolonged exposures. In addition, drugs that effect urinary pH are known to alter the elimination of amphetamine, and any decrease in amphetamine's metabolism that might occur due to drug interactions or genetic polymorphisms is more likely to be clinically significant when renal elimination is decreased [see Drug Interactions (7)].
Special Populations
Comparison of the pharmacokinetics of d- and l-amphetamine after oral administration of ADDERALL XR in children (6-12 years) and adolescent (13-17 years) ADHD patients and healthy adult volunteers indicates that body weight is the primary determinant of apparent differences in the pharmacokinetics of d- and l-amphetamine across the age range. Systemic exposure measured by area under the curve to infinity (AUC∞) and maximum plasma concentration (Cmax) decreased with increases in body weight, while oral volume of distribution (VZ/F), oral clearance (CL/F), and elimination half-life (t1/2) increased with increases in body weight.
Pediatric Patients
On a mg/kg weight basis, children eliminated amphetamine faster than adults. The elimination half-life (t1/2) is approximately 1 hour shorter for d-amphetamine and 2 hours shorter for l-amphetamine in children than in adults. However, children had higher systemic exposure to amphetamine (Cmax and AUC) than adults for a given dose of ADDERALL XR, which was attributed to the higher dose administered to children on a mg/kg body weight basis compared to adults. Upon dose normalization on a mg/kg basis, children showed 30% less systemic exposure compared to adults.
Gender
Systemic exposure to amphetamine was 20-30% higher in women (N=20) than in men (N=20) due to the higher dose administered to women on a mg/kg body weight basis. When the exposure parameters (Cmax and AUC) were normalized by dose (mg/kg), these differences diminished. Age and gender had no direct effect on the pharmacokinetics of d- and l-amphetamine.
Race
Formal pharmacokinetic studies for race have not been conducted. However, amphetamine pharmacokinetics appeared to be comparable among Caucasians (N=33), Blacks (N=8) and Hispanics (N=10).
Patients with Renal Impairment
The effect of renal impairment on d- and l-amphetamine after administration of ADDERALL XR has not been studied. The impact of renal impairment on the disposition of amphetamine is expected to be similar between oral administration of lisdexamfetamine and Adderall XR.
In a pharmacokinetic study of lisdexamfetamine in adult subjects with normal and impaired renal function, mean d-amphetamine clearance was reduced from 0.7 L/hr/kg in normal subjects to 0.4 L/hr/kg in subjects with severe renal impairment (GFR 15 to <30mL/min/1.73m²). Dialysis did not significantly affect the clearance of d-amphetamine [see Use in Specific Populations (8.6)].
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
No evidence of carcinogenicity was found in studies in which d,l-amphetamine (enantiomer ratio of 1:1) was administered to mice and rats in the diet for 2 years at doses of up to 30 mg/kg/day in male mice, 19 mg/kg/day in female mice, and 5 mg/kg/day in male and female rats. These doses are approximately 2.4, 1.5, and 0.8 times, respectively, the maximum recommended human dose of 30 mg/day given to children, on a mg/m² basis.
Mutagenesis
Amphetamine, in the enantiomer ratio d- to l- ratio of 3:1, was not clastogenic in the mouse bone marrow micronucleus test in vivo and was negative when tested in the E. coli component of the Ames test in vitro. d,l-Amphetamine (1:1 enantiomer ratio) has been reported to produce a positive response in the mouse bone marrow micronucleus test, an equivocal response in the Ames test, and negative responses in the in vitro sister chromatid exchange and chromosomal aberration assays.
Impairment of Fertility
Amphetamine, in the enantiomer ratio d- to l- ratio of 3:1, did not adversely affect fertility or early embryonic development in the rat at doses of up to 20 mg/kg/day (approximately 8 times the maximum recommended human dose of 20 mg/day given to adolescents, on a mg/m² basis).
13.2. Animal Toxicology and/or Pharmacology
Acute administration of high doses of amphetamine (d- or d,l-) has been shown to produce long-lasting neurotoxic effects, including irreversible nerve fiber damage, in rodents. The significance of these findings to humans is unknown.
14. Clinical Studies
Pediatric Patients
A double-blind, randomized, placebo-controlled, parallel-group study was conducted in children aged 6-12 (N=584) who met DSM-IV criteria for ADHD (either the combined type or the hyperactive-impulsive type). Patients were randomized to fixed-dose treatment groups receiving final doses of 10, 20, or 30 mg of ADDERALL XR or placebo once daily in the morning for three weeks. Significant improvements in patient behavior, based upon teacher ratings of attention and hyperactivity, were observed for all ADDERALL XR doses compared to patients who received placebo, for all three weeks, including the first week of treatment, when all ADDERALL XR subjects were receiving a dose of 10 mg/day. Patients who received ADDERALL XR showed behavioral improvements in both morning and afternoon assessments compared to patients on placebo.
In a classroom analogue study, patients (N=51) receiving fixed doses of 10 mg, 20 mg or 30 mg ADDERALL XR demonstrated statistically significant improvements in teacher-rated behavior and performance measures, compared to patients treated with placebo.
A double-blind, randomized, multi-center, parallel-group, placebo-controlled study was conducted in adolescents aged 13-17 (N=327) who met DSM-IV criteria for ADHD. The primary cohort of patients (n=287, weighing ≤75kg/165lbs) was randomized to fixed-dose treatment groups and received four weeks of treatment. Patients were randomized to receive final doses of 10 mg, 20 mg, 30 mg, and 40 mg ADDERALL XR or placebo once daily in the morning. Patients randomized to doses greater than 10 mg were titrated to their final doses by 10 mg each week. The secondary cohort consisted of 40 subjects weighing >75kg/165lbs who were randomized to fixed-dose treatment groups receiving final doses of 50 mg and 60 mg ADDERALL XR or placebo once daily in the morning for 4 weeks. The primary efficacy variable was the Attention Deficit Hyperactivity Disorder-Rating Scale IV (ADHD-RS-IV) total score for the primary cohort. The ADHD-RS-IV is an 18-item scale that measures the core symptoms of ADHD. Improvements in the primary cohort were statistically significantly greater in all four primary cohort active treatment groups (ADDERALL XR 10 mg, 20 mg, 30 mg, and 40 mg) compared with the placebo group. There was not adequate evidence that doses greater than 20 mg/day conferred additional benefit.
Adult Patients
A double-blind, randomized, placebo-controlled, parallel-group study was conducted in adults (N=255) who met DSM-IV criteria for ADHD. Patients were randomized to fixed-dose treatment groups receiving final doses of 20, 40, or 60 mg of ADDERALL XR or placebo once daily in the morning for four weeks. Significant improvements, measured with the Attention Deficit Hyperactivity Disorder-Rating Scale (ADHD-RS), an 18- item scale that measures the core symptoms of ADHD, were observed at endpoint for all ADDERALL XR doses compared to patients who received placebo for all four weeks. There was not adequate evidence that doses greater than 20 mg/day conferred additional benefit.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.