AMYVID Solution for injection Ref.[10078] Active ingredients: Florbetapir ¹⁸F
Source: FDA, National Drug Code (US) Revision Year: 2020
1. Indications and Usage
Amyvid is indicated for Positron Emission Tomography (PET) imaging of the brain to estimate β-amyloid neuritic plaque density in adult patients with cognitive impairment who are being evaluated for Alzheimer's Disease (AD) and other causes of cognitive decline. A negative Amyvid scan indicates sparse to no neuritic plaques and is inconsistent with a neuropathological diagnosis of AD at the time of image acquisition; a negative scan result reduces the likelihood that a patient's cognitive impairment is due to AD. A positive Amyvid scan indicates moderate to frequent amyloid neuritic plaques; neuropathological examination has shown this amount of amyloid neuritic plaque is present in patients with AD, but may also be present in patients with other types of neurologic conditions as well as older people with normal cognition. Amyvid is an adjunct to other diagnostic evaluations.
Limitations of Use:
- A positive Amyvid scan does not establish a diagnosis of AD or other cognitive disorder.
- Safety and effectiveness of Amyvid have not been established for:
- Predicting development of dementia or other neurologic condition;
- Monitoring responses to therapies.
2. Dosage and Administration
2.1 Radiation Safety-Drug Handling
Amyvid is a radioactive drug and should be handled with appropriate safety measures to minimize radiation exposure during administration [see Warnings and Precautions (5.1)]. Use waterproof gloves and effective shielding, including syringe shields when handling Amyvid. Radiopharmaceuticals, including Amyvid, should only be used by or under the control of physicians who are qualified by specific training and experience in the safe use and handling of radioactive materials, and whose experience and training have been approved by the appropriate governmental agency authorized to license the use of radiopharmaceuticals.
2.2 Recommended Dosing and Administration Instructions
The recommended dose for Amyvid is 370 MBq (10 mCi), maximum 50 μg mass dose, administered as a single intravenous bolus in a total volume of 10 mL or less. Follow the injection with an intravenous flush of 0.9% sterile sodium chloride.
- Inspect the radiopharmaceutical dose solution prior to administration and do not use it if it contains particulate matter or is discolored.
- Use aseptic technique and radiation shielding to withdraw Amyvid solution.
- Assay the dose in a suitable dose calibrator prior to administration.
- Inject Amyvid through a short intravenous catheter (approximately 1.5 inches or less) to minimize the potential for adsorption of the drug to the catheter. Portions of the Amyvid dose may adhere to longer catheters.
2.3 Image Acquisition Guidelines
A 10-minute PET image should be acquired starting 30 to 50 minutes after Amyvid intravenous injection. The patient should be supine and the head positioned to center the brain, including the cerebellum, in the PET scanner field of view. Reducing head movement with tape or other flexible head restraints may be employed. Image reconstruction should include attenuation correction with resulting transaxial pixel sizes between 2 and 3 mm.
2.4 Image Display and Interpretation
Amyvid images should be interpreted only by readers who successfully complete a special training program [see Warnings and Precautions (5.1)]. Training is provided by the manufacturer using either an in-person tutorial or an electronic process.
The objective of Amyvid image interpretation is to provide an estimate of the brain β-amyloid neuritic plaque density, not to make a clinical diagnosis. Image interpretation is performed independently of a patient's clinical features and relies upon the recognition of unique image features.
Image Display
Images should be displayed in the transaxial orientation with access as needed to the sagittal and coronal planes. In reviewing the images, include all transaxial slices of the brain using a black-white scale with the maximum intensity of the scale set to the maximum intensity of all the brain pixels. Initially locate the brain slice with the highest levels of image contrast (highest radioactivity signals for Amyvid uptake) and adjust the contrast appropriately. Start image interpretation by displaying slices sequentially from the bottom of the brain to the top. Periodically refer to the sagittal and coronal plane image display, as needed to better define the radioactivity uptake and to ensure that the entire brain is displayed.
Image Interpretation
Image interpretation is based upon the distribution of radioactive signal within the brain; clinical information is not a component of the image assessment [see Warnings and Precautions (5.1)]. Images are designated as positive or negative by comparing the radioactivity in cortical gray matter with activity in the adjacent white matter. This determination is made only in the cerebral cortex; the signal uptake in the cerebellum does not contribute to the scan interpretation (for example, a positive scan may show retained cerebellar gray-white contrast even when the cortical gray-white contrast is lost).
- Negative scans show more radioactivity in white matter than in gray matter, creating clear gray-white contrast.
- Positive scans show cortical areas with reduction or loss of the normally distinct gray-white contrast. These scans have one or more areas with increased cortical gray matter signal which results in reduced (or absent) gray-white contrast. Specifically, a positive scan will have either:
- Two or more brain areas (each larger than a single cortical gyrus) in which there is reduced or absent gray-white contrast. This is the most common appearance of a positive scan.
or
** One or more areas in which gray matter radioactivity is intense and clearly exceeds radioactivity in adjacent white matter.
Some scans may be difficult to interpret due to image noise, atrophy with a thinned cortical ribbon, or image blur. For cases in which there is uncertainty as to the location or edge of gray matter on the PET scan and a co-registered computerized tomography (CT) image is available (as when the study is done on a PET/CT scanner) the interpreter should examine the CT image to clarify the relationship of the PET radioactivity and the gray matter anatomy.
Figures 1, 2, and 3 provide examples of negative and positive scans. Figure 1 demonstrates varying degrees of normal gray-white contrast (negative) and examples where gray-white contrast has been lost (positive). Figure 2 illustrates typical features of a negative scan, while Figure 3 shows the loss of gray-white contrast in different brain regions of a positive scan.
Figure 1. Examples of Amyvid negative scans (top two rows) and positive scans (bottom two rows). Left to right panels show sagittal, coronal, and transverse PET image slices. Final panel to right shows enlarged picture of the brain area under the box. The top two arrows are pointing to normal preserved gray-white contrast with the cortical radioactivity less than the adjacent white matter. The bottom two arrows indicate areas of decreased gray-white contrast with increased cortical radioactivity that is comparable to the radioactivity in the adjacent white matter.
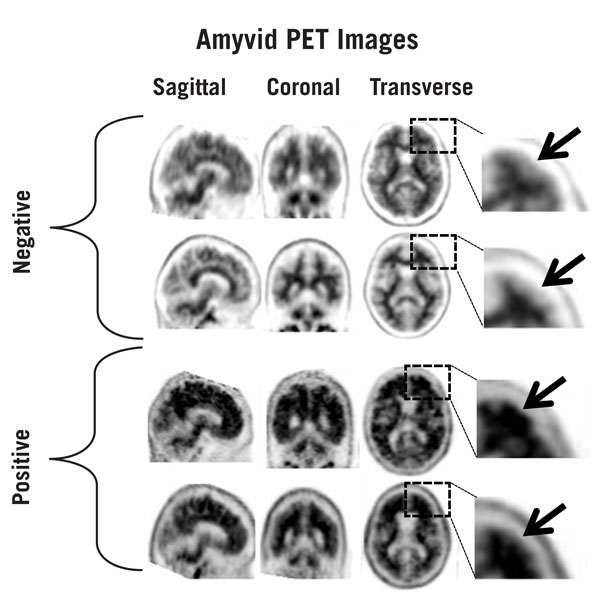
Figure 2. Typical Negative Scan. Images are displayed from a negative scan with upper (top) and lower (bottom) transverse slices both showing good gray-white matter contrast. On the right side of each slice, dotted lines have been used to illustrate the edge of the cortical gray matter (outer line) and the gray-white border (inner line). These dotted lines highlight contrast in uptake between the less intense uptake in the gray matter and the more intense uptake in the white matter. In addition, arrows illustrate the following points:
A) White matter tracts can be delineated from the frontal lobe to parietal lobe.
B) White matter tracts are clearly identified throughout the occipital / temporal area.
C) Scalloped appearance is seen with "fingers" of white matter in the frontal cortex.
D) Low levels of tracer in scalp or skull that should be distinguished from gray matter uptake by its shape and position.
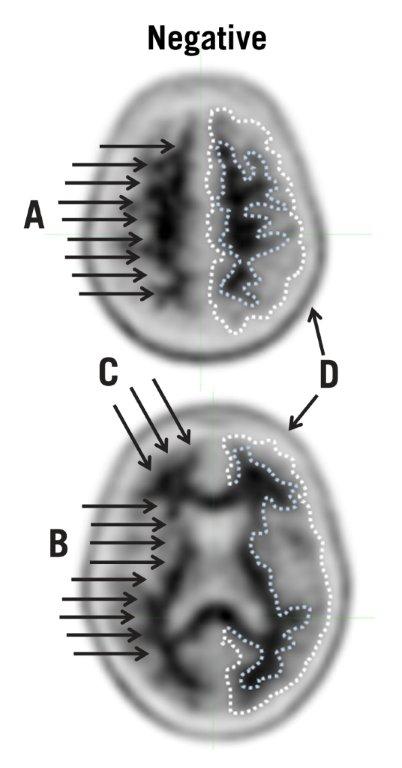
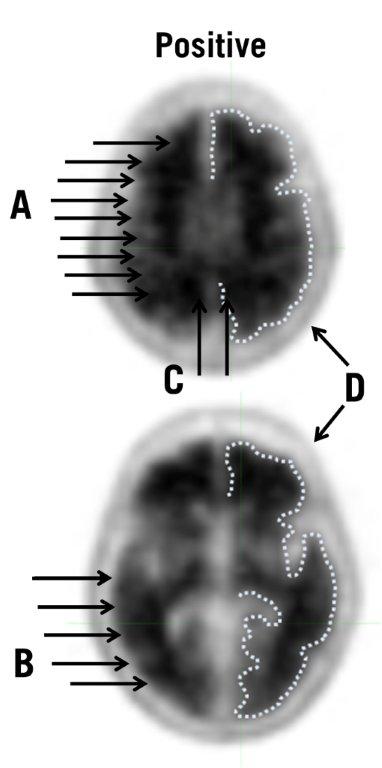
Figure 3. Typical Positive Scan: Images from a positive scan showing upper (top) and lower (bottom) transverse slices with loss of gray-white matter contrast in multiple brain regions. On the right side of each slice the edge of the cortical gray matter has been illustrated with a dotted line. Compared to the images from the negative case in Figure 2, the gray matter uptake is more similar to the white matter uptake and the gray-white matter border is more difficult to discern. In addition, arrows show the following points:
A) White matter tracts are difficult to fully identify as they travel from frontal to parietal lobe.
B) Borders of white matter tracts in occipital/temporal area are lost in places.
C) Gray matter in medial parietal cortex (precuneus) has increased uptake.
D) Low levels of tracer in scalp or skull that should be distinguished from gray matter uptake by its shape and position.
2.5 Radiation Dosimetry
The estimated radiation absorbed doses for adults from intravenous injection of Amyvid are shown in Table 1.
Table 1. Estimated Radiation Absorbed Dose, Amyvid (Florbetapir F 18 Injection):
| ORGAN/TISSUE | MEAN ABSORBED DOSE PER UNIT ADMINISTERED ACTIVITY(μGy/MBq) |
|---|---|
| Adrenal | 14 |
| Bone - Osteogenic Cells | 28 |
| Bone - Red Marrow | 14 |
| Brain | 10 |
| Breasts | 6 |
| Gallbladder Wall | 143 |
| GIa - Lower Large Intestine Wall | 28 |
| GI - Small Intestine | 66 |
| GI - Stomach Wall | 12 |
| GI - Upper Large Intestine Wall | 74 |
| Heart Wall | 13 |
| Kidneys | 14 |
| Liver | 64 |
| Lungs | 9 |
| Muscle | 9 |
| Ovaries | 18 |
| Pancreas | 14 |
| Skin | 6 |
| Spleen | 9 |
| Testes | 7 |
| Thymus | 7 |
| Thyroid | 7 |
| Urinary Bladder Wall | 27 |
| Uterus | 16 |
| Total Body | 12 |
| Effective Dose (μSv/MBq)b | 19 |
a Gastrointestinal
b Assumed radiation weighting factor, wr, (formerly defined as quality factor, Q) of 1 for conversion of absorbed dose (Gray or rads) to dose equivalent (Sieverts or rem) for F 18. To obtain radiation absorbed dose in rad/mCi from above table, multiply the dose in μGy/MBq by 0.0037, (e.g., 14 μGy/MBq x 0.0037 = 0.0518 rad/mCi)
The effective dose resulting from a 370 MBq (10 mCi) dose of Amyvid is 7.0 mSv in an adult, (19 x 370 = 7030 μSv = 7.030 mSv). The use of a CT scan to calculate attenuation correction for reconstruction of Amyvid images (as done in PET/CT imaging) will add radiation exposure. Diagnostic head CT scans using helical scanners administer an average of 2.2 ± 1.3 mSv effective dose (CRCPD Publication E-07-2, 2007). The actual radiation dose is operator and scanner dependent. The total radiation exposure from Amyvid administration and subsequent scan on a PET/CT scanner is estimated to be 9 mSv.
16.2. Storage and Handling
Store Amyvid at 25ºC (77°F); excursions permitted to 15ºC to 30ºC (59°F to 86°F) [see USP Controlled Room Temperature]. The product does not contain a preservative. Store Amyvid within the original container or equivalent radiation shielding. Amyvid must not be diluted.
This preparation is approved for use by persons under license by the Nuclear Regulatory Commission or the relevant regulatory authority of an Agreement State.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.