COZAAR Film-coated tablet Ref.[10551] Active ingredients: Losartan
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
Angiotensin II [formed from angiotensin I in a reaction catalyzed by angiotensin converting enzyme (ACE, kininase II)] is a potent vasoconstrictor, the primary vasoactive hormone of the renin-angiotensin system, and an important component in the pathophysiology of hypertension. It also stimulates aldosterone secretion by the adrenal cortex. Losartan and its principal active metabolite block the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor found in many tissues, (e.g., vascular smooth muscle, adrenal gland). There is also an AT2 receptor found in many tissues but it is not known to be associated with cardiovascular homeostasis. Neither losartan nor its principal active metabolite exhibits any partial agonist activity at the AT1 receptor, and both have much greater affinity (about 1000-fold) for the AT1 receptor than for the AT2 receptor. In vitro binding studies indicate that losartan is a reversible, competitive inhibitor of the AT1 receptor. The active metabolite is 10 to 40 times more potent by weight than losartan and appears to be a reversible, non-competitive inhibitor of the AT1 receptor.
Neither losartan nor its active metabolite inhibits ACE (kininase II, the enzyme that converts angiotensin I to angiotensin II and degrades bradykinin), nor do they bind to or block other hormone receptors or ion channels known to be important in cardiovascular regulation.
12.2. Pharmacodynamics
Losartan inhibits the pressor effect of angiotensin II (as well as angiotensin I) infusions. A dose of 100 mg inhibits the pressor effect by about 85% at peak with 25-40% inhibition persisting for 24 hours. Removal of the negative feedback of angiotensin II causes a doubling to tripling in plasma renin activity and consequent rise in angiotensin II plasma concentration in hypertensive patients. Losartan does not affect the response to bradykinin, whereas ACE inhibitors increase the response to bradykinin. Aldosterone plasma concentrations fall following losartan administration. In spite of the effect of losartan on aldosterone secretion, very little effect on serum potassium was observed.
The effect of losartan is substantially present within one week but in some studies the maximal effect occurred in 3-6 weeks. In long-term follow-up studies (without placebo control) the effect of losartan appeared to be maintained for up to a year. There is no apparent rebound effect after abrupt withdrawal of losartan. There was essentially no change in average heart rate in losartan-treated patients in controlled trials.
12.3. Pharmacokinetics
Absorption
Following oral administration, losartan is well absorbed and undergoes substantial first-pass metabolism. The systemic bioavailability of losartan is approximately 33%. Mean peak concentrations of losartan and its active metabolite are reached in 1 hour and in 3-4 hours, respectively. While maximum plasma concentrations of losartan and its active metabolite are approximately equal, the AUC (area under the curve) of the metabolite is about 4 times as great as that of losartan. A meal slows absorption of losartan and decreases its Cmax but has only minor effects on losartan AUC or on the AUC of the metabolite (~10% decrease). The pharmacokinetics of losartan and its active metabolite are linear with oral losartan doses up to 200 mg and do not change over time.
Distribution
The volume of distribution of losartan and the active metabolite is about 34 liters and 12 liters, respectively. Both losartan and its active metabolite are highly bound to plasma proteins, primarily albumin, with plasma free fractions of 1.3% and 0.2%, respectively. Plasma protein binding is constant over the concentration range achieved with recommended doses. Studies in rats indicate that losartan crosses the blood-brain barrier poorly, if at all.
Metabolism
Losartan is an orally active agent that undergoes substantial first-pass metabolism by cytochrome P450 enzymes. It is converted, in part, to an active carboxylic acid metabolite that is responsible for most of the angiotensin II receptor antagonism that follows losartan treatment. About 14% of an orally-administered dose of losartan is converted to the active metabolite. In addition to the active carboxylic acid metabolite, several inactive metabolites are formed. In vitro studies indicate that cytochrome P450 2C9 and 3A4 are involved in the biotransformation of losartan to its metabolites.
Elimination
Total plasma clearance of losartan and the active metabolite is about 600 mL/min and 50 mL/min, respectively, with renal clearance of about 75 mL/min and 25 mL/min, respectively. The terminal half-life of losartan is about 2 hours and of the metabolite is about 6-9 hours. After single doses of losartan administered orally, about 4% of the dose is excreted unchanged in the urine and about 6% is excreted in urine as active metabolite. Biliary excretion contributes to the elimination of losartan and its metabolites. Following oral 14C-labeled losartan, about 35% of radioactivity is recovered in the urine and about 60% in the feces. Following an intravenous dose of 14C-labeled losartan, about 45% of radioactivity is recovered in the urine and 50% in the feces. Neither losartan nor its metabolite accumulates in plasma upon repeated once-daily dosing.
Specific Populations
Pediatric
Pharmacokinetic parameters after multiple doses of losartan (average dose 0.7 mg/kg, range 0.36 to 0.97 mg/kg) as a tablet to 25 hypertensive patients aged 6 to 16 years are shown in Table 4 below. Pharmacokinetics of losartan and its active metabolite were generally similar across the studied age groups and similar to historical pharmacokinetic data in adults. The principal pharmacokinetic parameters in adults and children are shown in the table below.
Table 2. Pharmacokinetic Parameters in Hypertensive Adults and Children Age 6-16 Following Multiple Dosing:
| Adults given 50 mg once daily for 7 days N=12 | Age 6-16 given 0.7 mg/kg once daily for 7 days N=25 | |||
|---|---|---|---|---|
| Parent | Active Metabolite | Parent | Active Metabolite | |
| AUC0-24 (ng∙hr/mL)* | 442 ± 173 | 1685 ± 452 | 368 ± 169 | 1866 ± 1076 |
| CMAX (ng/mL)* | 224 ± 82 | 212 ± 73 | 141 ± 88 | 222 ± 127 |
| T1/2 (h)† | 2.1 ± 0.70 | 7.4 ± 2.4 | 2.3 ± 0.8 | 5.6 ± 1.2 |
| TPEAK (h)‡ | 0.9 | 3.5 | 2.0 | 4.1 |
| CLREN (mL/min)* | 56 ± 23 | 20 ± 3 | 53 ± 33 | 17 ± 8 |
* Mean ± standard deviation
† Harmonic mean and standard deviation
‡ Median
The bioavailability of the suspension formulation was compared with losartan tablets in healthy adults. The suspension and tablet are similar in their bioavailability with respect to both losartan and the active metabolite [see Dosage and Administration (2.5)].
Geriatric and Gender
Losartan pharmacokinetics have been investigated in the elderly (65-75 years) and in both genders. Plasma concentrations of losartan and its active metabolite are similar in elderly and young hypertensives. Plasma concentrations of losartan were about twice as high in female hypertensives as male hypertensives, but concentrations of the active metabolite were similar in males and females. No dosage adjustment is necessary [see Dosage and Administration (2.1)].
Race
Pharmacokinetic differences due to race have not been studied [see Use in Specific Populations (8.6)].
Renal Insufficiency
Following oral administration, plasma concentrations and AUCs of losartan and its active metabolite are increased by 50-90% in patients with mild (creatinine clearance of 50 to 74 mL/min) or moderate (creatinine clearance 30 to 49 mL/min) renal insufficiency. In this study, renal clearance was reduced by 55-85% for both losartan and its active metabolite in patients with mild or moderate renal insufficiency. Neither losartan nor its active metabolite can be removed by hemodialysis [see Warnings and Precautions (5.3) and Use in Specific Populations (8.7)].
Hepatic Insufficiency
Following oral administration in patients with mild to moderate alcoholic cirrhosis of the liver, plasma concentrations of losartan and its active metabolite were, respectively, 5-times and about 1.7-times those in young male volunteers. Compared to normal subjects the total plasma clearance of losartan in patients with hepatic insufficiency was about 50% lower and the oral bioavailability was about doubled. Use a starting dose of 25 mg for patients with mild to moderate hepatic impairment. COZAAR has not been studied in patients with severe hepatic impairment [see Dosage and Administration (2.4) and Use in Specific Populations (8.8)].
Drug Interactions
No clinically significant drug interactions have been found in studies of losartan potassium with hydrochlorothiazide, digoxin, warfarin, cimetidine and phenobarbital. However, rifampin has been shown to decrease the AUC of losartan and its active metabolite by 30% and 40%, respectively. Fluconazole, an inhibitor of cytochrome P450 2C9, decreased the AUC of the active metabolite by approximately 40%, but increased the AUC of losartan by approximately 70% following multiple doses. Conversion of losartan to its active metabolite after intravenous administration is not affected by ketoconazole, an inhibitor of P450 3A4. The AUC of active metabolite following oral losartan was not affected by erythromycin, an inhibitor of P450 3A4, but the AUC of losartan was increased by 30%.
The pharmacodynamic consequences of concomitant use of losartan and inhibitors of P450 2C9 have not been examined. Subjects who do not metabolize losartan to active metabolite have been shown to have a specific, rare defect in cytochrome P450 2C9. These data suggest that the conversion of losartan to its active metabolite is mediated primarily by P450 2C9 and not P450 3A4.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Losartan potassium was not carcinogenic when administered at maximally tolerated dosages to rats and mice for 105 and 92 weeks, respectively. Female rats given the highest dose (270 mg/kg/day) had a slightly higher incidence of pancreatic acinar adenoma. The maximally tolerated dosages (270 mg/kg/day in rats, 200 mg/kg/day in mice) provided systemic exposures for losartan and its pharmacologically active metabolite that were approximately 160 and 90 times (rats) and 30 and 15 times (mice) the exposure of a 50 kg human given 100 mg per day.
Losartan potassium was negative in the microbial mutagenesis and V-79 mammalian cell mutagenesis assays and in the in vitro alkaline elution and in vitro and in vivo chromosomal aberration assays. In addition, the active metabolite showed no evidence of genotoxicity in the microbial mutagenesis, in vitro alkaline elution, and in vitro chromosomal aberration assays.
Fertility and reproductive performance were not affected in studies with male rats given oral doses of losartan potassium up to approximately 150 mg/kg/day. The administration of toxic dosage levels in females (300/200 mg/kg/day) was associated with a significant (p<0.05) decrease in the number of corpora lutea/female, implants/female, and live fetuses/female at C-section. At 100 mg/kg/day only a decrease in the number of corpora lutea/female was observed. The relationship of these findings to drug-treatment is uncertain since there was no effect at these dosage levels on implants/pregnant female, percent post-implantation loss, or live animals/litter at parturition. In nonpregnant rats dosed at 135 mg/kg/day for 7 days, systemic exposure (AUCs) for losartan and its active metabolite were approximately 66 and 26 times the exposure achieved in man at the maximum recommended human daily dosage (100 mg).
14. Clinical Studies
14.1 Hypertension
Adult Hypertension
The antihypertensive effects of COZAAR were demonstrated principally in 4 placebo-controlled, 6- to 12-week trials of dosages from 10 to 150 mg per day in patients with baseline diastolic blood pressures of 95-115. The studies allowed comparisons of two doses (50-100 mg/day) as once-daily or twice-daily regimens, comparisons of peak and trough effects, and comparisons of response by gender, age, and race. Three additional studies examined the antihypertensive effects of losartan and hydrochlorothiazide in combination.
The 4 studies of losartan monotherapy included a total of 1075 patients randomized to several doses of losartan and 334 to placebo. The 10- and 25-mg doses produced some effect at peak (6 hours after dosing) but small and inconsistent trough (24 hour) responses. Doses of 50, 100 and 150 mg once daily gave statistically significant systolic/diastolic mean decreases in blood pressure, compared to placebo in the range of 5.5-10.5/3.5-7.5 mmHg, with the 150-mg dose giving no greater effect than 50-100 mg. Twice-daily dosing at 50-100 mg/day gave consistently larger trough responses than once-daily dosing at the same total dose. Peak (6 hour) effects were uniformly, but moderately, larger than trough effects, with the trough-to-peak ratio for systolic and diastolic responses 50-95% and 60-90%, respectively.
Addition of a low dose of hydrochlorothiazide (12.5 mg) to losartan 50 mg once daily resulted in placebo-adjusted blood pressure reductions of 15.5/9.2 mmHg.
Analysis of age, gender, and race subgroups of patients showed that men and women, and patients over and under 65, had generally similar responses. COZAAR was effective in reducing blood pressure regardless of race, although the effect was somewhat less in Black patients (usually a low-renin population).
Pediatric Hypertension
The antihypertensive effect of losartan was studied in one trial enrolling 177 hypertensive pediatric patients aged 6 to 16 years old. Children who weighed <50 kg received 2.5, 25 or 50 mg of losartan daily and patients who weighed ≥50 kg received 5, 50 or 100 mg of losartan daily. Children in the lowest dose group were given losartan in a suspension formulation [see Dosage and Administration (2.1)]. The majority of the children had hypertension associated with renal and urogenital disease. The sitting diastolic blood pressure (SiDBP) on entry into the study was higher than the 95 th percentile level for the patient’s age, gender, and height. At the end of three weeks, losartan reduced systolic and diastolic blood pressure, measured at trough, in a dose-dependent manner. Overall, the two higher doses (25 to 50 mg in patients <50 kg; 50 to 100 mg in patients ≥50 kg) reduced diastolic blood pressure by 5 to 6 mmHg more than the lowest dose used (2.5 mg in patients <50 kg; 5 mg in patients ≥50 kg). The lowest dose, corresponding to an average daily dose of 0.07 mg/kg, did not appear to offer consistent antihypertensive efficacy. When patients were randomized to continue losartan at the two higher doses or to placebo after 3 weeks of therapy, trough diastolic blood pressure rose in patients on placebo between 5 and 7 mmHg more than patients randomized to continuing losartan. When the low dose of losartan was randomly withdrawn, the rise in trough diastolic blood pressure was the same in patients receiving placebo and in those continuing losartan, again suggesting that the lowest dose did not have significant antihypertensive efficacy. Overall, no significant differences in the overall antihypertensive effect of losartan were detected when the patients were analyzed according to age (<, ≥12 years old) or gender. While blood pressure was reduced in all racial subgroups examined, too few non-White patients were enrolled to compare the dose-response of losartan in the non-White subgroup.
14.2 Hypertensive Patients with Left Ventricular Hypertrophy
The LIFE study was a multinational, double-blind study comparing COZAAR and atenolol in 9193 hypertensive patients with ECG-documented left ventricular hypertrophy. Patients with myocardial infarction or stroke within six months prior to randomization were excluded. Patients were randomized to receive once daily COZAAR 50 mg or atenolol 50 mg. If goal blood pressure (<140/90 mmHg) was not reached, hydrochlorothiazide (12.5 mg) was added first and, if needed, the dose of COZAAR or atenolol was then increased to 100 mg once daily. If necessary, other antihypertensive treatments (e.g., increase in dose of hydrochlorothiazide therapy to 25 mg or addition of other diuretic therapy, calcium-channel blockers, alpha-blockers, or centrally acting agents, but not ACE inhibitors, angiotensin II antagonists, or beta-blockers) were added to the treatment regimen to reach the goal blood pressure.
Of the randomized patients, 4963 (54%) were female and 533 (6%) were Black. The mean age was 67 with 5704 (62%) age ≥65. At baseline, 1195 (13%) had diabetes, 1326 (14%) had isolated systolic hypertension, 1469 (16%) had coronary heart disease, and 728 (8%) had cerebrovascular disease. Baseline mean blood pressure was 174/98 mmHg in both treatment groups. The mean length of follow-up was 4.8 years. At the end of study or at the last visit before a primary endpoint, 77% of the group treated with COZAAR and 73% of the group treated with atenolol were still taking study medication. Of the patients still taking study medication, the mean doses of COZAAR and atenolol were both about 80 mg/day, and 15% were taking atenolol or losartan as monotherapy, while 77% were also receiving hydrochlorothiazide (at a mean dose of 20 mg/day in each group). Blood pressure reduction measured at trough was similar for both treatment groups but blood pressure was not measured at any other time of the day. At the end of study or at the last visit before a primary endpoint, the mean blood pressures were 144.1/81.3 mmHg for the group treated with COZAAR and 145.4/80.9 mmHg for the group treated with atenolol; the difference in systolic blood pressure (SBP) of 1.3 mmHg was significant (p<0.001), while the difference of 0.4 mmHg in diastolic blood pressure (DBP) was not significant (p=0.098).
The primary endpoint was the first occurrence of cardiovascular death, nonfatal stroke, or nonfatal myocardial infarction. Patients with nonfatal events remained in the trial, so that there was also an examination of the first event of each type even if it was not the first event (e.g., a stroke following an initial myocardial infarction would be counted in the analysis of stroke). Treatment with COZAAR resulted in a 13% reduction (p=0.021) in risk of the primary endpoint compared to the atenolol group (see Figure 1 and Table 3); this difference was primarily the result of an effect on fatal and nonfatal stroke. Treatment with COZAAR reduced the risk of stroke by 25% relative to atenolol (p=0.001) (see Figure 2 and Table 3).
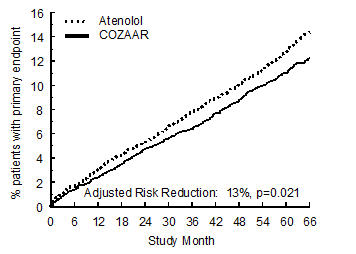
Figure 1: Kaplan-Meier estimates of the primary endpoint of time to cardiovascular death, nonfatal stroke, or nonfatal myocardial infarction in the groups treated with COZAAR and atenolol. The Risk Reduction is adjusted for baseline Framingham risk score and level of electrocardiographic left ventricular hypertrophy.
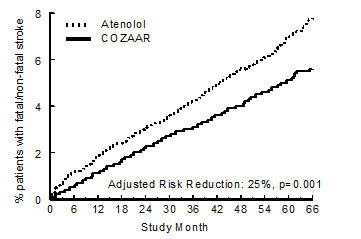
Figure 2: Kaplan-Meier estimates of the time to fatal/nonfatal stroke in the groups treated with COZAAR and atenolol. The Risk Reduction is adjusted for baseline Framingham risk score and level of electrocardiographic left ventricular hypertrophy.
Table 3 shows the results for the primary composite endpoint and the individual endpoints. The primary endpoint was the first occurrence of stroke, myocardial infarction or cardiovascular death, analyzed using an ITT approach. The table shows the number of events for each component in two different ways. The Components of Primary Endpoint (as a first event) counts only the events that define the primary endpoint, while the Secondary Endpoints count all first events of a particular type, whether or not they were preceded by a different type of event.
Table 3. Incidence of Primary Endpoint Events:
| COZAAR | Atenolol | Risk Reduction* | 95% CI | p-Value | |||
|---|---|---|---|---|---|---|---|
| N (%) | Rate† | N (%) | Rate† | ||||
| Primary Composite Endpoint | 508 (11) | 23.8 | 588 (13) | 27.9 | 13% | 2% to 23% | 0.021 |
| Components of Primary Composite Endpoint (as a first event) | |||||||
| Stroke (nonfatal) | 209 (5) | 286 (6) | |||||
| Myocardial infarction (nonfatal) | 174 (4) | 168 (4) | |||||
| Cardiovascular mortality | 125 (3) | 134 (3) | |||||
| Secondary Endpoints (any time in study) | |||||||
| Stroke (fatal/nonfatal) | 232 (5) | 10.8 | 309 (7) | 14.5 | 25% | 11% to 37% | 0.001 |
| Myocardial infarction (fatal/nonfatal) | 198 (4) | 9.2 | 188 (4) | 8.7 | -7% | -13% to 12% | 0.491 |
| Cardiovascular mortality | 204 (4) | 9.2 | 234 (5) | 10.6 | 11% | -7% to 27% | 0.206 |
| Due to CHD | 125 (3) | 5.6 | 124 (3) | 5.6 | -3% | -32% to 20% | 0.839 |
| Due to Stroke | 40 (1) | 1.8 | 62 (1) | 2.8 | 35% | 4% to 67% | 0.032 |
| Other‡ | 39 (1) | 1.8 | 48 (1) | 2.2 | 16% | -28% to 45% | 0.411 |
* Adjusted for baseline Framingham risk score and level of electrocardiographic left ventricular hypertrophy
† Rate per 1000 patient-years of follow-up
‡ Death due to heart failure, non-coronary vascular disease, pulmonary embolism, or a cardiovascular cause other than stroke or coronary heart disease
Although the LIFE study favored COZAAR over atenolol with respect to the primary endpoint (p=0.021), this result is from a single study and, therefore, is less compelling than the difference between COZAAR and placebo. Although not measured directly, the difference between COZAAR and placebo is compelling because there is evidence that atenolol is itself effective (vs. placebo) in reducing cardiovascular events, including stroke, in hypertensive patients.
Other clinical endpoints of the LIFE study were: total mortality, hospitalization for heart failure or angina pectoris, coronary or peripheral revascularization procedures, and resuscitated cardiac arrest. There were no significant differences in the rates of these endpoints between the COZAAR and atenolol groups.
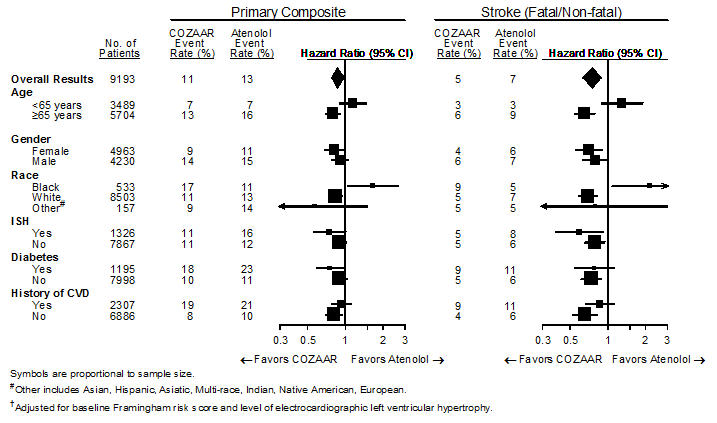
For the primary endpoint and stroke, the effects of COZAAR in patient subgroups defined by age, gender, race and presence or absence of isolated systolic hypertension (ISH), diabetes, and history of cardiovascular disease (CVD) are shown in Figure 3 below. Subgroup analyses can be difficult to interpret and it is not known whether these represent true differences or chance effects.
Figure 3. Primary Endpoint Events† within Demographic Subgroups:
14.3 Nephropathy in Type 2 Diabetic Patients
The RENAAL study was a randomized, placebo-controlled, double-blind, multicenter study conducted worldwide in 1513 patients with type 2 diabetes with nephropathy (defined as serum creatinine 1.3 to 3.0 mg/dL in females or males ≤60 kg and 1.5 to 3.0 mg/dL in males >60 kg and proteinuria [urinary albumin to creatinine ratio ≥300 mg/g]).
Patients were randomized to receive COZAAR 50 mg once daily or placebo on a background of conventional antihypertensive therapy excluding ACE inhibitors and angiotensin II antagonists. After one month, investigators were instructed to titrate study drug to 100 mg once daily if the trough blood pressure goal (140/90 mmHg) was not achieved. Overall, 72% of patients received the 100-mg daily dose more than 50% of the time they were on study drug. Because the study was designed to achieve equal blood pressure control in both groups, other antihypertensive agents (diuretics, calcium-channel blockers, alpha- or beta-blockers, and centrally acting agents) could be added as needed in both groups. Patients were followed for a mean duration of 3.4 years.
The study population was diverse with regard to race (Asian 16.7%, Black 15.2%, Hispanic 18.3%, White 48.6%). Overall, 63.2% of the patients were men, and 66.4% were under the age of 65 years. Almost all of the patients (96.6%) had a history of hypertension, and the patients entered the trial with a mean serum creatinine of 1.9 mg/dL and mean proteinuria (urinary albumin/creatinine) of 1808 mg/g at baseline.
The primary endpoint of the study was the time to first occurrence of any one of the following events: doubling of serum creatinine, end-stage renal disease (ESRD) (need for dialysis or transplantation), or death. Treatment with COZAAR resulted in a 16% risk reduction in this endpoint (see Figure 4 and Table 4). Treatment with COZAAR also reduced the occurrence of sustained doubling of serum creatinine by 25% and ESRD by 29% as separate endpoints, but had no effect on overall mortality (see Table 4).
The mean baseline blood pressures were 152/82 mmHg for COZAAR plus conventional antihypertensive therapy and 153/82 mmHg for placebo plus conventional antihypertensive therapy. At the end of the study, the mean blood pressures were 143/76 mmHg for the group treated with COZAAR and 146/77 mmHg for the group treated with placebo.
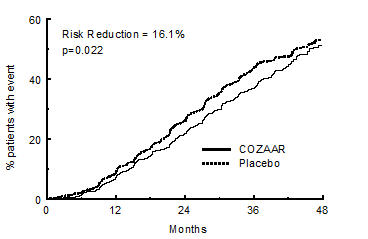
Figure 4: Kaplan-Meier curve for the primary composite endpoint of doubling of serum creatinine, end stage renal disease (need for dialysis or transplantation) or death.
Table 4. Incidence of Primary Endpoint Events:
| Incidence | Risk Reduction | 95% C.I. | p-Value | ||
|---|---|---|---|---|---|
| Losartan | Placebo | ||||
| Primary Composite Endpoint | 43.5% | 47.1% | 16.1% | 2.3% to 27.9% | 0.022 |
| Doubling of Serum Creatinine, ESRD and Death Occurring as a First Event | |||||
| Doubling of Serum Creatinine | 21.6% | 26.0% | |||
| ESRD | 8.5% | 8.5% | |||
| Death | 13.4% | 12.6% | |||
| Overall Incidence of Doubling of Serum Creatinine, ESRD and Death | |||||
| Doubling of Serum Creatinine | 21.6% | 26.0% | 25.3% | 7.8% to 39.4% | 0.006 |
| ESRD | 19.6% | 25.5% | 28.6% | 11.5% to 42.4% | 0.002 |
| Death | 21.0% | 20.3% | -1.7% | -26.9% to 18.6% | 0.884 |
The secondary endpoints of the study were change in proteinuria, change in the rate of progression of renal disease, and the composite of morbidity and mortality from cardiovascular causes (hospitalization for heart failure, myocardial infarction, revascularization, stroke, hospitalization for unstable angina, or cardiovascular death). Compared with placebo, COZAAR significantly reduced proteinuria by an average of 34%, an effect that was evident within 3 months of starting therapy, and significantly reduced the rate of decline in glomerular filtration rate during the study by 13%, as measured by the reciprocal of the serum creatinine concentration. There was no significant difference in the incidence of the composite endpoint of cardiovascular morbidity and mortality.
The favorable effects of COZAAR were seen in patients also taking other anti-hypertensive medications (angiotensin II receptor antagonists and angiotensin converting enzyme inhibitors were not allowed), oral hypoglycemic agents and lipid-lowering agents.
For the primary endpoint and ESRD, the effects of COZAAR in patient subgroups defined by age, gender and race are shown in Table 5 below. Subgroup analyses can be difficult to interpret and it is not known whether these represent true differences or chance effects.
Table 5. Efficacy Outcomes within Demographic Subgroups:
| Primary Composite Endpoint | ESRD | ||||||
|---|---|---|---|---|---|---|---|
| No. of Patients | COZAAR Event Rate % | Placebo Event Rate % | Hazard Ratio (95% CI) | COZAAR Event Rate % | Placebo Event Rate % | Hazard Ratio (95% CI) | |
| Overall Results | 1513 | 43.5 | 47.1 | 0.84 (0.72, 0.98) | 19.6 | 25.5 | 0.71 (0.58, 0.89) |
| Age | |||||||
| <65 years | 1005 | 44.1 | 49.0 | 0.78 (0.65, 0.94) | 21.1 | 28.5 | 0.67 (0.52, 0.86) |
| ≥65 years | 508 | 42.3 | 43.5 | 0.98 (0.75, 1.28) | 16.5 | 19.6 | 0.85 (0.56, 1.28) |
| Gender | |||||||
| Female | 557 | 47.8 | 54.1 | 0.76 (0.60, 0.96) | 22.8 | 32.8 | 0.60 (0.44, 0.83) |
| Male | 956 | 40.9 | 43.3 | 0.89 (0.73, 1.09) | 17.5 | 21.5 | 0.81 (0.60, 1.08) |
| Race | |||||||
| Asian | 252 | 41.9 | 54.8 | 0.66 (0.45, 0.95) | 18.8 | 27.4 | 0.63 (0.37, 1.07) |
| Black | 230 | 40.0 | 39.0 | 0.98 (0.65, 1.50) | 17.6 | 21.0 | 0.83 (0.46, 1.52) |
| Hispanic | 277 | 55.0 | 54.0 | 1.00 (0.73, 1.38) | 30.0 | 28.5 | 1.02 (0.66, 1.59) |
| White | 735 | 40.5 | 43.2 | 0.81 (0.65, 1.01) | 16.2 | 23.9 | 0.60 (0.43, 0.83) |
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.