ELVANSE Capsule, hard Ref.[7642] Active ingredients: Lisdexamfetamine
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2019 Publisher: Shire Pharmaceutical Contracts Limited, 1 Kingdom Street, London, W2 6BD, UNITED KINGDOM
Contraindications
Hypersensitivity to sympathomimetic amines or any of the excipients listed in section 6.1.
Concomitant use of monoamine oxidase inhibitors (MAOI) or within 14 days after MAOI treatment (hypertensive crisis may result; see section 4.5).
Hyperthyroidism or thyrotoxicosis.
Agitated states.
Symptomatic cardiovascular disease.
Advanced arteriosclerosis.
Moderate to severe hypertension.
Glaucoma.
Special warnings and precautions for use
Abuse and dependence
Stimulants including Elvanse have a potential for abuse, misuse, dependence, or diversion for non-therapeutic uses that physicians should consider when prescribing this product. Stimulants should be prescribed cautiously to patients with a history of substance abuse or dependence.
Tolerance, extreme psychological dependence, and severe social disability have occurred with the abuse of stimulants. There are reports of patients who have increased the dosage of amfetamine to levels many times higher than recommended; abrupt cessation following prolonged high dosage administration results in extreme fatigue and mental depression. Changes are also noted on the sleep EEG. Manifestations of chronic intoxication with amfetamines may include severe dermatoses, marked insomnia, irritability, hyperactivity, and personality changes. The most severe manifestation of chronic intoxication is psychosis, often clinically indistinguishable from schizophrenia.
Cardiovascular adverse events
Sudden death in patients with pre-existing structural cardiac abnormalities or other serious heart problems
Children and adolescents: Sudden death has been reported in children and adolescents taking CNS stimulants, including those with structural cardiac abnormalities or other serious heart problems. Although some serious heart problems alone carry an increased risk of sudden death, stimulant products generally should not be used in children or adolescents with known serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, or other serious cardiac problems that may place them at increased vulnerability to the sympathomimetic effects of a stimulant drug.
Adults: Sudden deaths, stroke, and myocardial infarction have been reported in adults taking stimulant drugs at usual doses for ADHD. Although the role of stimulants in these adult cases is also unknown, adults have a greater likelihood than children of having serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, coronary artery disease, or other serious cardiac problems. Adults with such abnormalities should also generally not be treated with stimulant drugs.
Hypertension and other cardiovascular conditions
Stimulant medications cause a modest increase in average blood pressure (about 2-4 mmHg) and average heart rate (about 3-6 bpm), and individuals may have larger increases. While the mean changes alone would not be expected to have short-term consequences, all patients should be monitored for larger changes in heart rate and blood pressure. Caution is indicated in treating patients whose underlying medical conditions might be compromised by increases in blood pressure or heart rate, e.g. those with pre-existing hypertension, heart failure, recent myocardial infarction, or ventricular arrhythmia.
The use of Elvanse is contraindicated in patients with symptomatic cardiovascular disease and also in those patients with moderate to severe hypertension (see section 4.3).
Cardiomyopathy
Cardiomyopathy has been reported with chronic amfetamine use. It has also been reported with Elvanse.
Assessing cardiovascular status in patients being treated with stimulant medications
All patients who are being considered for treatment with stimulant medications should have a careful history (including assessment for a family history of sudden death or ventricular arrhythmia) and physical exam to assess for the presence of cardiac disease, and should receive further cardiac evaluation if findings suggest such disease (e.g. electrocardiogram or echocardiogram). Patients who develop symptoms such as exertional chest pain, unexplained syncope, or other symptoms suggestive of cardiac disease during stimulant treatment should undergo a prompt cardiac evaluation.
Psychiatric adverse events
Pre-existing psychosis
Administration of stimulants may exacerbate symptoms of behaviour disturbance and thought disorder in patients with pre-existing psychotic disorders.
Bipolar illness
Particular care should be taken in using stimulants to treat ADHD patients with comorbid bipolar disorder because of concern for possible induction of mixed/manic episode in such patients. Prior to initiating treatment with a stimulant, patients with comorbid depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression.
Emergence of new psychotic or manic symptoms
Treatment emergent psychotic or manic symptoms, e.g., hallucinations, delusional thinking, or mania in children and adolescents without prior history of psychotic illness or mania can be caused by stimulants at usual doses. If such symptoms occur, consideration should be given to a possible causal role of the stimulant, and discontinuation of treatment may be appropriate.
Aggression
Aggressive behaviour or hostility is often observed in children and adolescents with ADHD, and has been reported in clinical trials and the postmarketing experience of some medications indicated for the treatment of ADHD including Elvanse. Stimulants may cause aggressive behaviour or hostility. Patients beginning treatment for ADHD should be monitored for the appearance of or worsening of aggressive behaviour or hostility.
Tics
Stimulants have been reported to exacerbate motor and phonic tics and Tourette's syndrome. Therefore, clinical evaluation for tics and Tourette's syndrome in children and their families should precede use of stimulant medications.
Long-term suppression of growth (height and weight)
Stimulants have been associated with a slowing of weight gain and a reduction in attained height. Growth should be monitored during treatment with stimulants, and patients who are not growing or gaining weight as expected may need to have their treatment interrupted. Height, weight, and appetite should be recorded at least 6-monthly.
In a controlled study of patients aged 6 to 17 years the mean (SD) changes in body weight after seven weeks were -2.35 (2.084) kg for Elvanse, +0.87 (1.102) kg for placebo, and -1.36 (1.552) kg for methylphenidate hydrochloride.
Seizures
There is some clinical evidence that stimulants may lower the convulsive threshold in patients with prior history of seizure, in patients with prior EEG abnormalities in absence of seizures, and very rarely, in patients without a history of seizures and no prior EEG evidence of seizures. In the presence of new onset or worsening seizures, the drug should be discontinued.
Visual disturbance
Difficulties with accommodation and blurring of vision have been reported with stimulant treatment.
Prescribing and dispensing
The least amount of Elvanse feasible should be prescribed or dispensed in order to minimise the risk of possible overdose by the patient.
Use with other sympathomimetic drugs
Elvanse should be used with caution in patients who use other sympathomimetic drugs (see section 4.5).
Use in adults
If treatment withdrawal has not been successful when an adolescent has reached 18 years of age continued treatment into adulthood may be necessary. The need for further treatment of these adults should be reviewed regularly and undertaken annually.
Excipients
This medicine contains less than 1 mmol sodium (23 mg) per capsule, that is to say essentially 'sodium-free'.
Interaction with other medicinal products and other forms of interaction
In vitro enzyme inhibition
In vitro experiments with human microsomes indicate minor inhibition of CYP2D6 by amfetamine and minor inhibition of CYP1A2, 2D6, and 3A4 by one or more metabolites. Although the clinical significance of this interaction is likely to be minimal, consideration should be given when medications metabolised by these pathways are administered.
Agents whose blood levels may be impacted by Elvanse
Extended release guanfacine: In a drug interaction study, administration of an extended release guanfacine in combination with Elvanse induced a 19% increase in guanfacine maximum plasma concentrations, whereas, exposure (area under the curve; AUC) was increased by 7%. These small changes are not expected to be clinically meaningful. In this study, no effect on dexamfetamine exposure was observed following co-administration of extended release guanfacine and Elvanse.
Extended release venlafaxine: In a drug interaction study, administration of 225 mg extended release venlafaxine, a CYP2D6 substrate, in combination with 70 mg Elvanse induced a 9% decrease in the Cmax and 17% decrease in the AUC for the primary active metabolite o-desmethylvenlafaxine and a 10% increase in Cmax and 13% increase in AUC for venlafaxine. Dexamfetamine may be a weak inhibitor of CYP2D6. Lisdexamfetamine has no effect on the AUC and Cmax of the composite of venlafaxine and o-desmethylvenlafaxine. These small changes are not expected to be clinically meaningful. In this study, no effect on dexamfetamine exposure was observed following co-administration of extended release venlafaxine and Elvanse.
Agents and conditions that alter urinary pH and impact the urinary excretion and half-life of amfetamine
Ascorbic acid and other agents and conditions (thiazide diuretics, diets high in animal protein, diabetes, respiratory acidosis) that acidify urine increase urinary excretion and decrease the half-life of amfetamine. Sodium bicarbonate and other agents and conditions (diets high in fruits and vegetables, urinary tract infections and vomiting) that alkalinise urine decrease urinary excretion and extend the half-life of amfetamine.
Monoamine oxidase inhibitors
Amfetamine should not be administered during or within 14 days following the administration of monoamine oxidase inhibitors (MAOI) because it can increase the release of norepinephrine and other monoamines. This can cause severe headaches and other signs of hypertensive crisis. A variety of toxic neurological effects and malignant hyperpyrexia can occur, sometimes with fatal outcomes (see section 4.3).
Serotonergic drugs
Serotonin syndrome has rarely occurred in association with the use of amphetamines such as Elvanse, when given in conjunction with serotonergic drugs, including selective serotonin reuptake inhibitors (SSRIs) and serotonin and noradrenaline reuptake inhibitors (SNRIs). It has also been reported in association with overdose of amphetamines, including Elvanse (see section 4.9).
Agents whose effects may be reduced by amfetamines
Antihypertensives: Amfetamines may decrease the effectiveness of guanethidine or other antihypertensive medications.
Agents whose effects may be potentiated by amfetamines
Amfetamines potentiate the analgesic effect of narcotic analgesics.
Agents that may reduce the effects of amfetamines
Chlorpromazine: Chlorpromazine blocks dopamine and norepinephrine receptors, thus inhibiting the central stimulant effects of amfetamines.
Haloperidol: Haloperidol blocks dopamine receptors, thus inhibiting the central stimulant effects of amfetamines.
Lithium carbonate: The anorectic and stimulatory effects of amfetamines may be inhibited by lithium carbonate.
Use with alcohol
There are limited data on the possible interaction with alcohol.
Drug/laboratory test interactions
Amfetamines can cause a significant elevation in plasma corticosteroid levels. This increase is greatest in the evening. Amfetamine may interfere with urinary steroid determinations.
Fertility, pregnancy and lactation
Pregnancy
There are no adequate and well controlled studies of Elvanse in pregnant women. Dexamfetamine, the active metabolite of lisdexamfetamine, crosses the placenta.
Lisdexamfetamine dimesylate had no effect on embryofoetal development or survival when administered orally to pregnant rats and rabbits (see section 5.3). Administration of lisdexamfetamine dimesylate to juvenile rats was associated with reductions in growth measurements at clinically relevant exposures.
The physician should discuss Elvanse treatment with female patients who have started menstruation. Elvanse should only be used during pregnancy if the potential benefit justifies the potential risk to the foetus.
Breast-feeding
Amfetamines are excreted in human milk. Elvanse should not be used during breast-feeding.
Fertility
Amfetamine has shown no harmful effects on fertility in a rat study (see section 5.3). The effect of Elvanse on human fertility has not been investigated.
Effects on ability to drive and use machines
Elvanse can cause dizziness, drowsiness and visual disturbances including difficulties with accommodation and blurred vision. These could have a moderate influence on the ability to drive and use machines. Patients should be warned of these possible effects and advised that if affected, they should avoid potentially hazardous activities such as driving or operating machinery.
This medicine can impair cognitive function and can affect a patient's ability to drive safely. This class of medicine is in the list of drugs included in regulations under 5a of the Road Traffic Act 1988. When prescribing this medicine, patients should be told:
- The medicine is likely to affect your ability to drive.
- Do not drive until you know how the medicine affects you.
- It is an offence to drive while under the influence of this medicine.
- However, you would not be committing an offence (called 'statutory defence') if:
- The medicine has been prescribed to treat a medical problem and
- You have taken it according to the instructions given by the prescriber and in the information provided with the medicine and
- It was not affecting your ability to drive safely.
Undesirable effects
Summary of the safety profile
Adverse reactions observed with Elvanse treatment mainly reflect side effects commonly associated with stimulant use. Very common adverse reactions include decreased appetite, insomnia, dry mouth, headache, upper abdominal pain, and weight decreased.
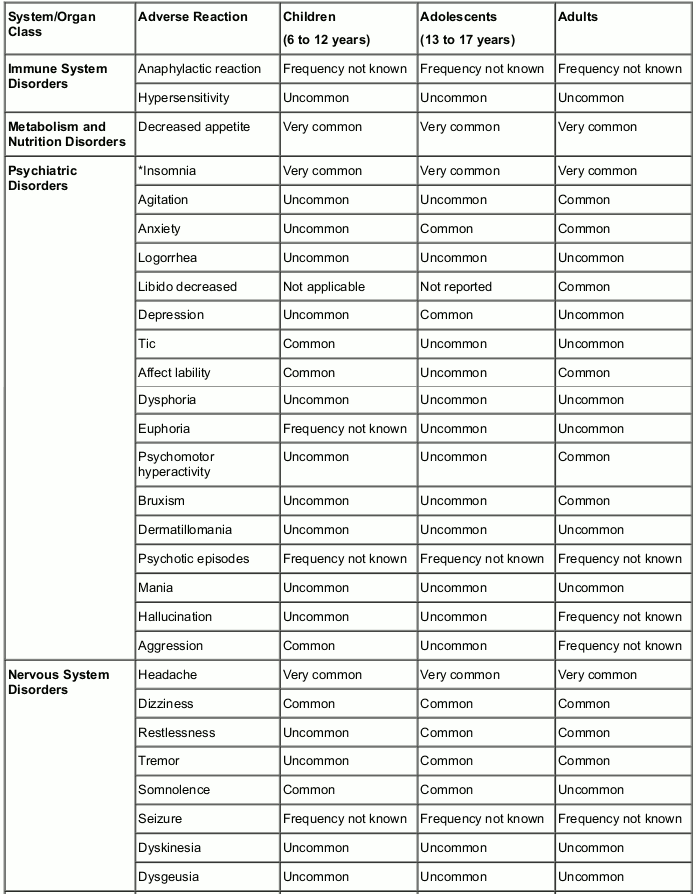
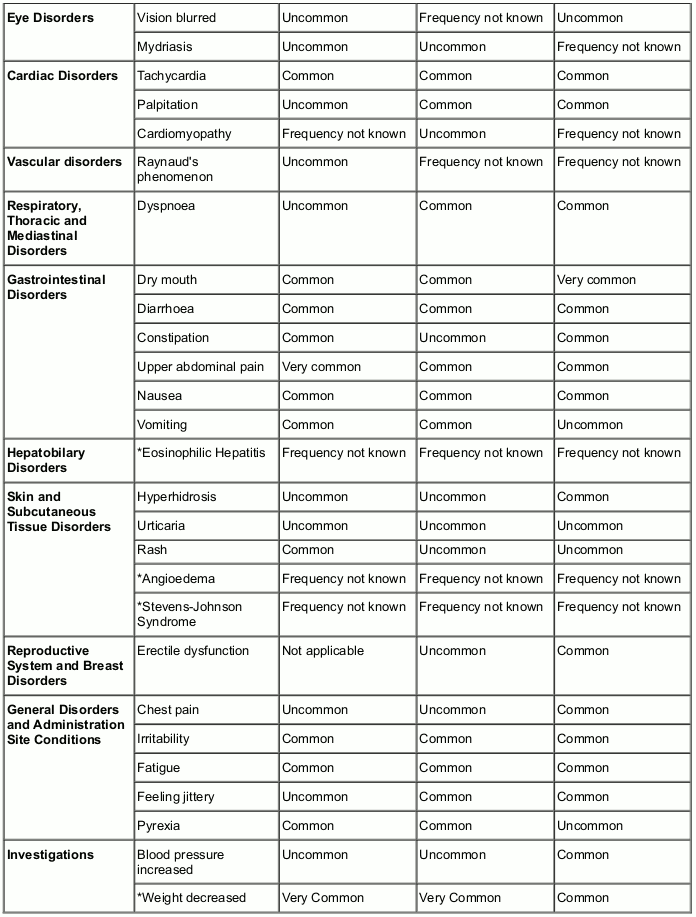
Tabulated summary of adverse reactions
The following table presents all adverse reactions based on clinical trials and spontaneous reporting.
The following definitions apply to the frequency terminology used hereafter:
Very common (≥1/10)
Common (≥1/100 to <1/10)
Uncommon (≥1/1,000 to <1/100)
Rare (≥1/10,000 to <1/1,000)
Very rare (<1/10,000)
Frequency not known (cannot be estimated from the available data).
An asterisk (*) indicates that additional information on the respective adverse reaction is provided below the table.
Description of selected adverse reactions
Insomnia
Includes insomnia, initial insomnia, middle insomnia, and terminal insomnia.
Weight decreased
In a 4-week controlled trial of Elvanse in children aged 6 to 12 years, mean weight loss from baseline to endpoint was 0.4, 0.9, and 1.1 kg, for patients assigned to receive 30 mg, 50 mg, and 70 mg of Elvanse respectively, compared to a 0.5 kg weight gain for patients receiving placebo. Higher doses were associated with greater weight loss with 4 weeks of treatment. Careful follow-up for weight in children aged 6 to 12 years who received Elvanse over 12 months suggests that continuous treatment (i.e. treatment for 7 days per week throughout the year) slows growth rate measured by body weight as demonstrated by an age- and sex-normalised mean change from baseline in percentile of -13.4 over 1 year. The average percentiles at baseline (n=271) and 12 months (n=146) were 60.9 and 47.2, respectively.
In a 4-week controlled trial of Elvanse in adolescents aged 13 to 17 years, mean weight loss from baseline to endpoint was 1.2, 1.9, and 2.3 kg for patients assigned to receive 30 mg, 50 mg, and 70 mg of Elvanse respectively, compared to a 0.9 kg weight gain for patients receiving placebo. Careful follow-up for weight in adolescents aged 13 to 17 years who received Elvanse over 12 months suggests that continuous treatment (i.e. treatment for 7 days per week throughout the year) slows growth rate measured by body weight as demonstrated by an age- and sex-normalised mean change from baseline in percentile of -6.5 over 1 year. The average percentiles at baseline (n=265) and 12 months (n=156) were 66.0 and 61.5, respectively.
In children and adolescents (aged 6-17) who received Elvanse over two years, careful monitoring of weight suggested that consistent medication (ie, treatment for 7 days per week throughout the two years) resulted in a slowing of growth as measured by body weight. In children and adolescents, the average weight percentiles and standard deviations (SD) at baseline (n=314) and 24 months (week 104, n=189), were 65.4 (SD 27.11) and 48.2 (SD 29.94), respectively. The age- and sex-normalized mean change from baseline in percentile over 2 years was -16.9 (SD17.33).
Eosinophilic hepatitis
No cases were reported in the clinical studies.
Angioedema
No cases were reported in the clinical studies.
Stevens-Johnson syndrome
No cases were reported in the clinical studies.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme (Website: www.mhra.gov.uk/yellowcard) or search for MHRA Yellow Card in the Google Play or Apple App Store.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.