EXVIERA Film-coated tablet Ref.[8766] Active ingredients: Dasabuvir
Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061 Ludwigshafen, Germany
Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
Patients with moderate to severe hepatic impairment (Child-Pugh B or C) (see section 5.2).
Use of ethinyloestradiol-containing medicinal products such as those contained in most combined oral contraceptives or contraceptive vaginal rings (see sections 4.4 and 4.5).
Co-administration of dasabuvir with medicinal products that are strong or moderate enzyme inducers is expected to decrease dasabuvir plasma concentrations and reduce its therapeutic effect (see section 4.5 Examples of contraindicated inducers are provided below.
Enzyme inducers:
- carbamazepine, phenytoin, phenobarbital
- efavirenz, nevirapine, etravirine
- apalutamide, enzalutamide
- mitotane
- rifampicin
- St. John’s Wort (Hypericum perforatum)
Medicinal products that are strong CYP2C8 inhibitors may increase dasabuvir plasma concentrations and must not be co-administered with dasabuvir (see section 4.5). Examples of contraindicated CYP2C8 inhibitors are provided below.
CYP2C8 inhibitor:
- gemfibrozil
Dasabuvir is administered with ombitasvir/paritaprevir/ritonavir. For contra-indications with ombitasvir/paritaprevir/ritonavir refer to the Summary of Product Characteristics.
Special warnings and precautions for use
General
Dasabuvir is not recommended for administration as monotherapy and must be used in combination with other medicinal products for the treatment of hepatitis C infection (see section 4.2 and 5.1).
Risk of hepatic decompensation and hepatic failure in patients with cirrhosis
Hepatic decompensation and hepatic failure, including liver transplantation or fatal outcomes, have been reported post-marketing in patients treated with dasabuvir with ombitasvir/paritaprevir/ritonavir with and without ribavirin. Most patients with these severe outcomes had evidence of advanced or decompensated cirrhosis prior to initiating therapy. Although causality is difficult to establish due to background advanced liver disease, a potential risk cannot be excluded.
Dasabuvir should not be used in patients with moderate to severe hepatic impairment (Child-Pugh B or C) (see sections 4.2, 4.3, 4.8 and 5.2).
For patients with cirrhosis:
- Monitoring should be performed for clinical signs and symptoms of hepatic decompensation (such as ascites, hepatic encephalopathy, variceal haemorrhage).
- Hepatic laboratory testing including direct bilirubin levels should be performed at baseline, during the first 4 weeks of starting treatment and as clinically indicated thereafter.
- Treatment should be discontinued in patients who develop evidence of hepatic decompensation.
ALT elevations
During clinical trials with dasabuvir and ombitasvir/paritaprevir/ritonavir with or without ribavirin, transient elevations of ALT to greater than 5 times the upper limit of normal occurred in approximately 1% of subjects (35 of 3,039). ALT elevations were asymptomatic and generally occurred during the first 4 weeks of treatment, without concomitant elevations of bilirubin, and declined within approximately two weeks of onset with continued dosing of dasabuvir and ombitasvir/paritaprevir/ritonavir with or without ribavirin.
These ALT elevations were significantly more frequent in the subgroup of subjects who were using ethinyloestradiol -containing medicinal products such as combined oral contraceptives or contraceptive vaginal rings (6 of 25 subjects); (see section 4.3). In contrast, the rate of ALT elevations in subjects using other types of oestrogens as typically used in hormonal replacement therapy (i.e., oral and topical oestradiol and conjugated oestrogens) was similar to the rate observed in subjects who were not using oestrogen-containing products (approximately 1% in each group).
Patients who are taking ethinyloestradiol-containing medicinal products (i.e. most combined oral contraceptives or contraceptive vaginal rings) must switch to an alternative method of contraception (e.g., progestin only contraception or non-hormonal methods) prior to initiating dasabuvir with ombitasvir/paritaprevir/ritonavir therapy (see sections 4.3 and 4.5).
Although ALT elevations associated with dasabuvir and ombitasvir/paritaprevir/ritonavir have been asymptomatic, patients should be instructed to watch for early warning signs of liver inflammation, such as fatigue, weakness, lack of appetite, nausea and vomiting, as well as later signs such as jaundice and discoloured faeces, and to consult a doctor without delay if such symptoms occur. Routine monitoring of liver enzymes is not necessary in patients that do not have cirrhosis (for cirrhotics, see above). Early discontinuation may result in drug resistance, but implications for future therapy are not known.
Pregnancy and concomitant use with ribavirin
Also see section 4.6.
Extreme caution must be taken to avoid pregnancy in female patients and female partners of male patients when dasabuvir is taken in combination with ribavirin (see section 4.6 and refer to the Summary of Product Characteristics for ribavirin for additional information).
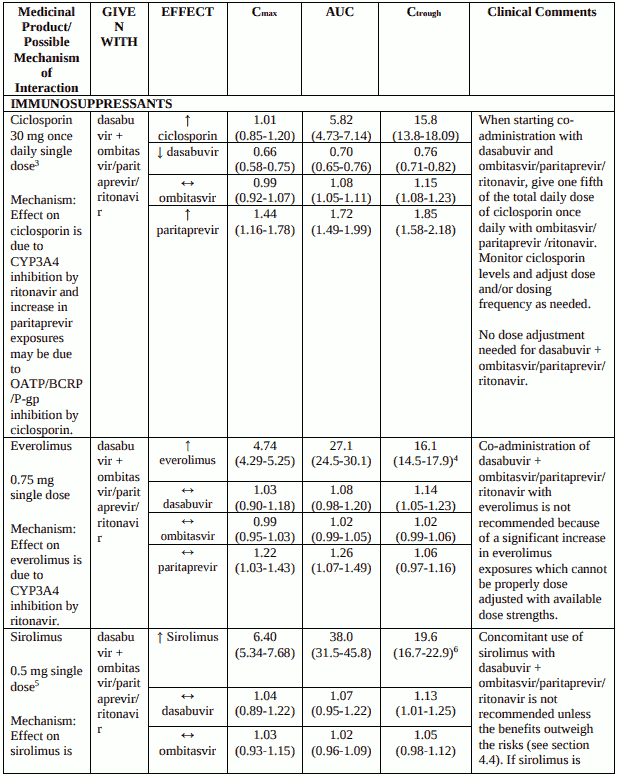
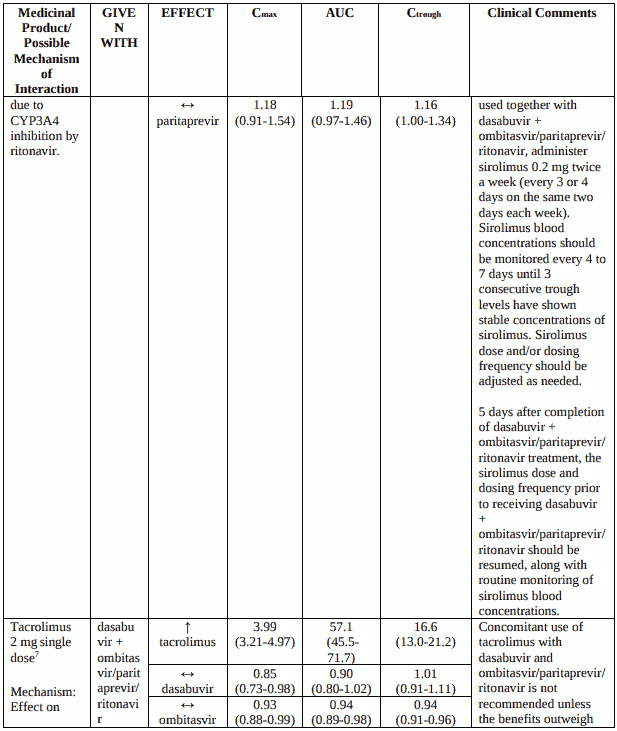
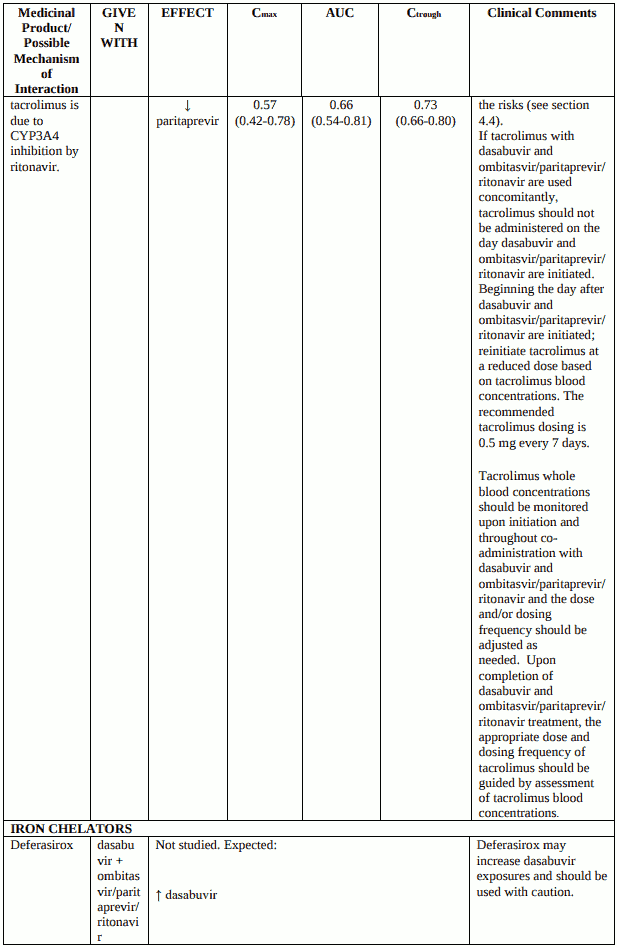
Use with tacrolimus, sirolimus and everolimus
Co-administration of dasabuvir and ombitasvir/paritaprevir/ritonavir with systemic tacrolimus, sirolimus or everolimus increases the concentrations of the immunosuppressant due to CYP3A inhibition by ritonavir (see section 4.5). Serious and/or life threatening events have been observed with co-administration of dasabuvir and ombitasvir/paritaprevir/ritonavir with systemic tacrolimus, and a similar risk can be expected with sirolimus and everolimus.
Avoid concomitant use of tacrolimus or sirolimus with dasabuvir and ombitasvir/paritaprevir/ritonavir unless the benefits outweigh the risks. If tacrolimus or sirolimus are used together with dasabuvir and ombitasvir/paritaprevir/ritonavir, caution is advised, and recommended doses and monitoring strategies can be found in section 4.5. Everolimus cannot be used due to lack of suitable dose strengths for dose adjustments.
Tacrolimus or sirolimus whole blood concentrations should be monitored upon initiation and throughout co-administration with dasabuvir and ombitasvir/paritaprevir/ritonavir and the dose and/or dosing frequency should be adjusted as needed. Patients should be monitored frequently for any changes in renal function or tacrolimus or sirolimus associated adverse reactions. Refer to the tacrolimus or sirolimus Summary of Product Characteristics for additional dosing and monitoring instructions.
Depression or psychiatric illness
Cases of depression and more rarely of suicidal ideation and suicide attempt have been reported with dasabuvir with or without ombitasvir/paritaprevir/ritonavir treatment in combination with ribavirin in the majority of the cases. Although some cases had previous history of depression, psychiatric illness and/or substance abuse, a causal relation with dasabuvir with or without ombitasvir/paritaprevir/ritonavir treatment cannot be excluded. Caution should be used in patients with a pre-existing history of depression or psychiatric illness. Patients and caregivers should be instructed to notify the prescriber of any changes in behaviour or mood and of any suicidal ideation.
Genotype-specific activity
Concerning recommended regimens with different HCV genotypes, see section 4.2. Concerning genotype-specific virological and clinical activity, see section 5.1.
The efficacy of dasabuvir has not been established in patients with HCV genotypes other than genotype 1; dasabuvir should not be used for the treatment of patients infected with other genotypes than 1.
Co-administration with other direct-acting antivirals against HCV
Dasabuvir safety and efficacy have been established in combination with ombitasvir/paritaprevir/ritonavir with or without ribavirin. Co-administration of dasabuvir with other antivirals has not been studied and, therefore, cannot be recommended.
Retreatment
The efficacy of dasabuvir in patients previously exposed to dasabuvir, or to medicinal products anticipated to be cross-resistant, has not been demonstrated.
Use with statins
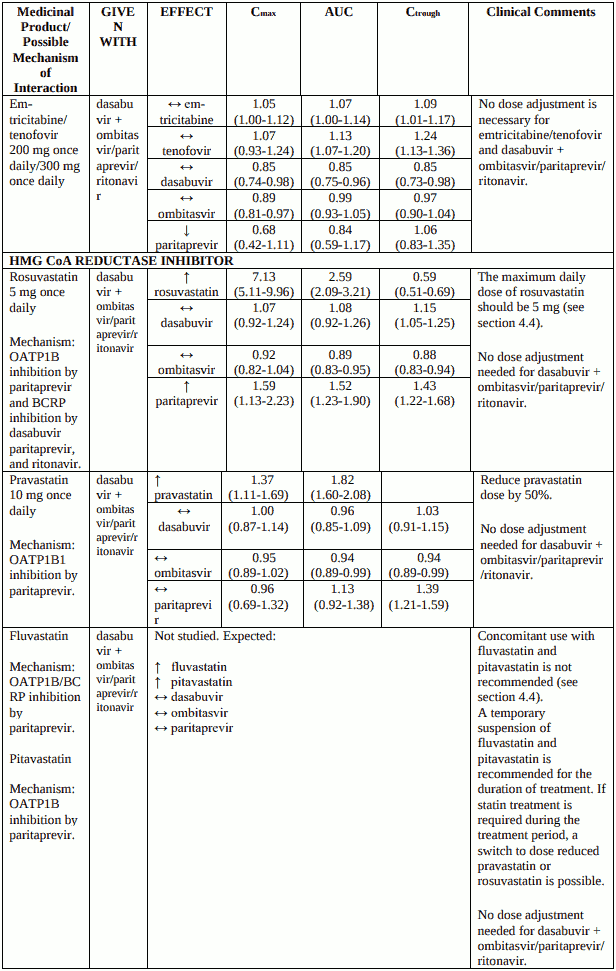
Rosuvastatin
Dasabuvir with ombitasvir/paritaprevir/ritonavir is expected to increase the exposure to rosuvastatin more than 3-fold. If rosuvastatin treatment is required during the treatment period, the maximum daily dose of rosuvastatin should be 5 mg (see section 4.5, Table 2).
Pitavastatin and fluvastatin
The interactions with pitavastatin and fluvastatin have not been investigated. Theoretically, dasabuvir with ombitasvir/paritaprevir/ritonavir is expected to increase the exposure to pitavastatin and fluvastatin. A temporary suspension of pitavastatin/fluvastatin is recommended for the duration of treatment with ombitasvir/paritaprevir/ritonavir. If statin treatment is required during the treatment period, a switch to a reduced dose of pravastatin/rosuvastatin is possible (see section 4.5, Table 2).
Treatment of patients with HIV co-infection
Dasabuvir is recommended in combination with paritaprevir/ombitasvir/ritonavir, and ritonavir may select for PI resistance in HIV co-infected patients without ongoing antiretroviral therapy. HIV coinfected patients without suppressive antiretroviral therapy should not be treated with dasabuvir. Drug interactions need to be carefully taken into account in the setting of HIV co-infection (for details see section 4.5, Table 2).
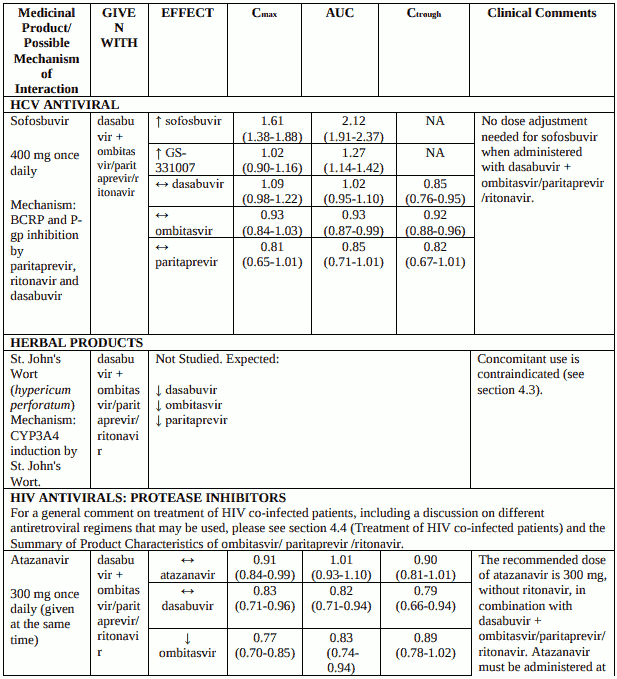
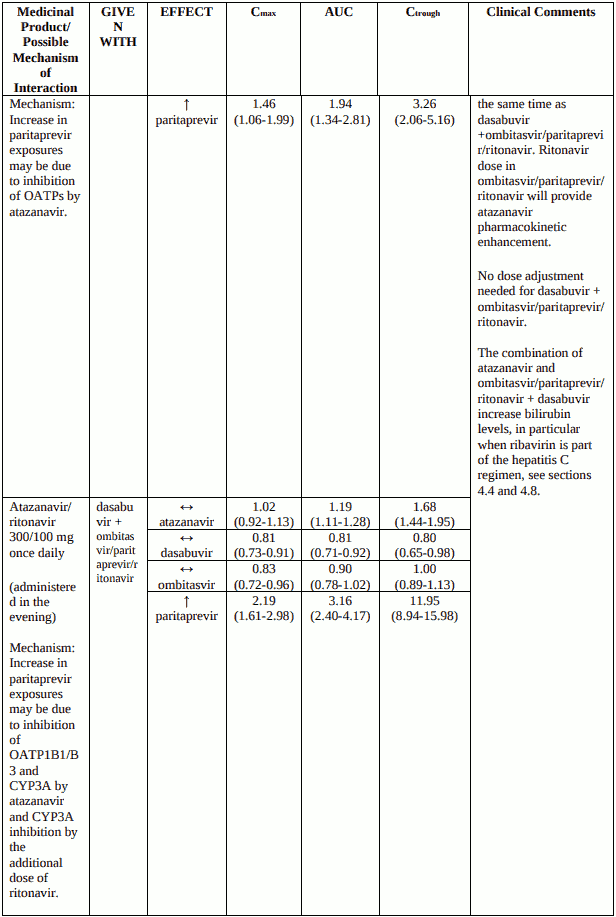
Atazanavir can be used in combination with dasabuvir with ombitasvir/paritaprevir/ritonavir if administered at the same time. To be noted, atazanavir should be taken without ritonavir, since ritonavir 100 mg once daily is provided as part of the ombitasvir/paritaprevir/ritonavir fixed dose combination. The combination carries an increased risk for hyperbilirubinemia (including ocular icterus), in particular when ribavirin is part of the hepatitis C regimen.
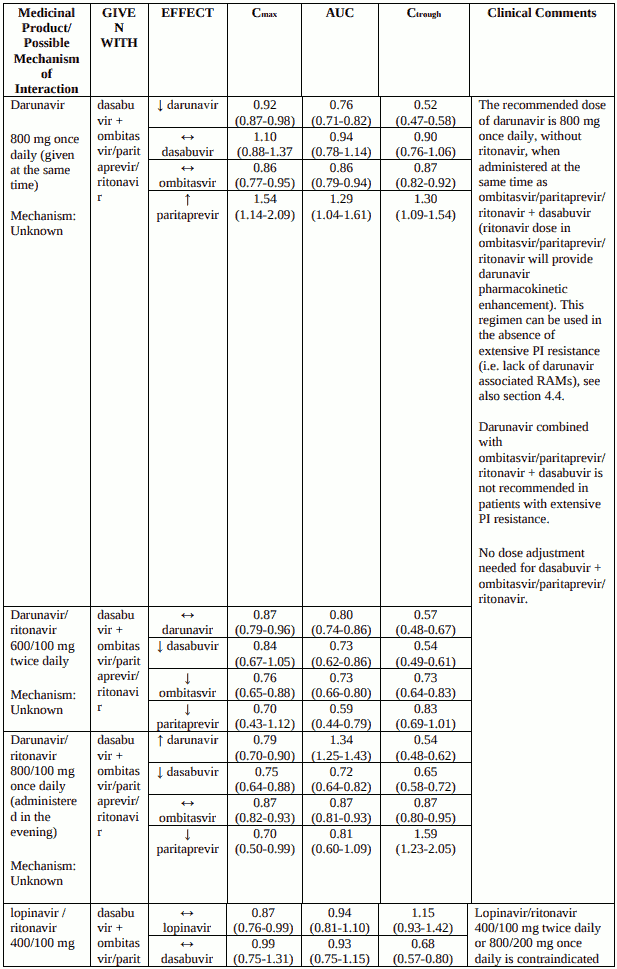
Darunavir, dosed 800 mg once daily, if administered at the same time as ombitasvir/paritaprevir/ritonavir, can be used in the absence of extensive PI resistance (darunavir exposure lowered). To be noted, darunavir should be taken without ritonavir, since ritonavir 100 mg once daily is provided as part of the ombitasvir/paritaprevir/ritonavir fixed dose combination.
For the use of HIV protease inhibitors other than atazanavir and darunavir refer to the Summary of Product Characteristics of ombitasvir/paritaprevir/ritonavir.
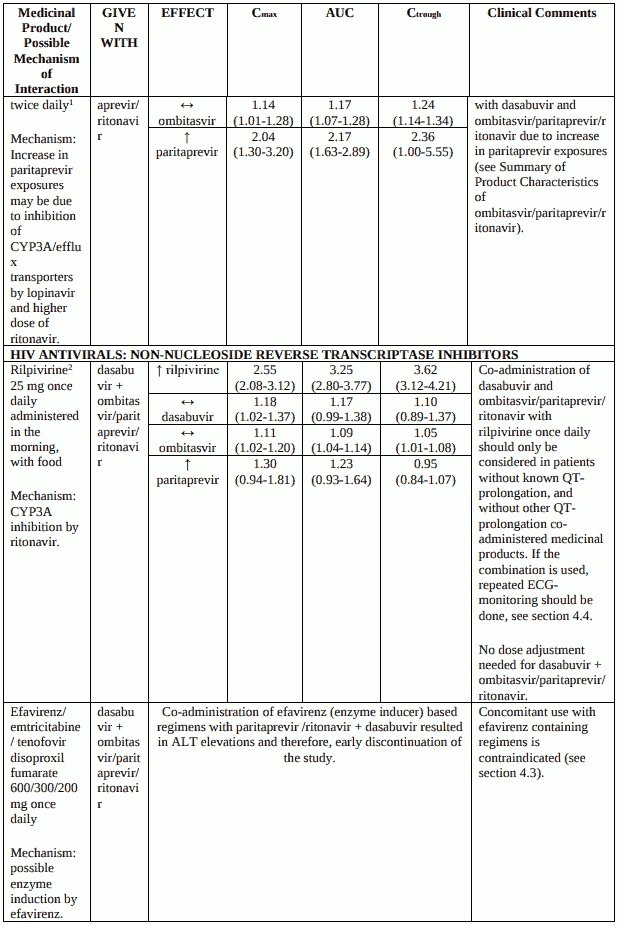
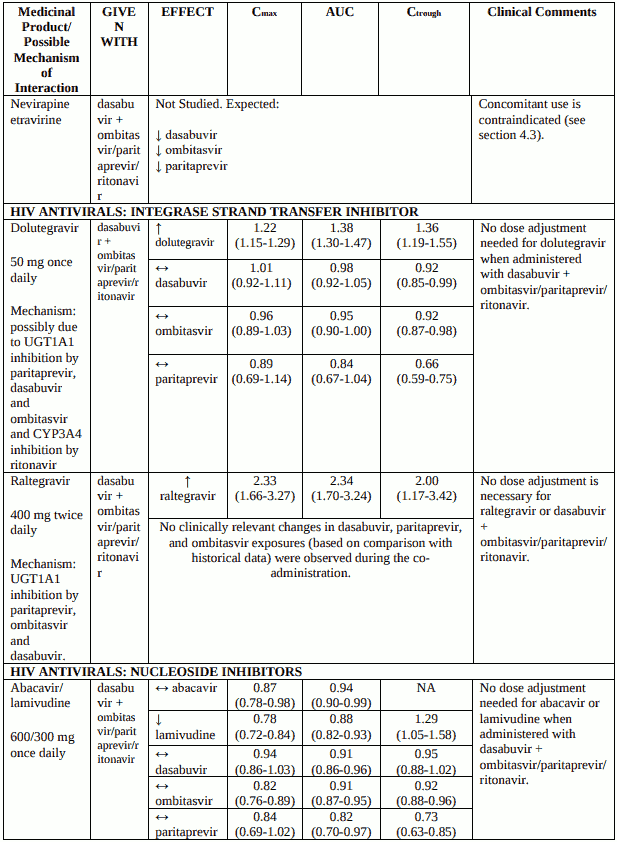
Raltegravir exposure is substantially increased (2-fold). The combination was not linked to any particular safety issues in a limited set of patients treated for 12-24 weeks.
Rilpivirine exposure is substantially increased (3-fold) when rilpivirine is given in combination with dasabuvir with ombitasvir/paritaprevir/ritonavir, with a consequent potential for QT-prolongation. If an HIV protease inhibitor is added (atazanavir, darunavir), rilpivirine exposure may increase even further and is, therefore, not recommended. Rilpivirine should be used cautiously, in the setting of repeated ECG monitoring.
NNRTIs other than rilpivirine (efavirenz, etravirine, and nevirapine) are contraindicated (see section 4.3).
Hepatitis B virus reactivation
Cases of hepatitis B virus (HBV) reactivation, some of them fatal, have been reported during or after treatment with direct-acting antiviral agents. HBV screening should be performed in all patients before initiation of treatment. HBV/HCV co-infected patients are at risk of HBV reactivation, and should, therefore, be monitored and managed according to current clinical guidelines.
Use in diabetic patients
Diabetics may experience improved glucose control, potentially resulting in symptomatic hypoglycaemia, after initiating HCV direct acting antiviral treatment. Glucose levels of diabetic patients initiating direct acting antiviral therapy should be closely monitored, particularly within the first 3 months, and their diabetic medicinal products modified when necessary. The physician in charge of the diabetic care of the patient should be informed when direct acting antiviral therapy is initiated.
Lactose
Exviera contains lactose. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.
Interaction with other medicinal products and other forms of interaction
Dasabuvir must always be administered together with ombitasvir/paritaprevir/ritonavir. When coadministered they exert mutual effects on each other (see section 5.2). Therefore, the interaction profile of the compounds must be considered as a combination.
Pharmacodynamic interactions
Coadministration with enzyme inducers may lead to an increased risk of adverse reactions and ALT elevations (see Table 2).
Coadministration with ethinyloestradiol may lead to increased risk of ALT elevations (see sections 4.3 and 4.4). Contraindicated enzyme inducers are provided in section 4.3.
Pharmacokinetic interactions
Potential for dasabuvir to affect the pharmacokinetics of other medicinal products In vivo drug interaction studies evaluated the net effect of the combination treatment, including ritonavir. The following section describes the specific transporters and metabolizing enzymes that are affected by dasabuvir when combined with ombitasvir/paritaprevir/ritonavir. See Table 2 for guidance regarding potential drug interactions and dosing recommendations for dasabuvir administered with ombitasvir/paritaprevir/ritonavir.
Medicinal products metabolised by CYP3A4
Refer to the ombitasvir/paritaprevir/ritonavir Summary of Product Characteristics for details (see also Table 2).
Medicinal products transported by the OATP family
Refer to the ombitasvir/paritaprevir/ritonavir Summary of Product Characteristics for details on OATP1B1, OATP1B3 and OATP2B1 substrates (see also Table 2).
Medicinal products transported by BCRP
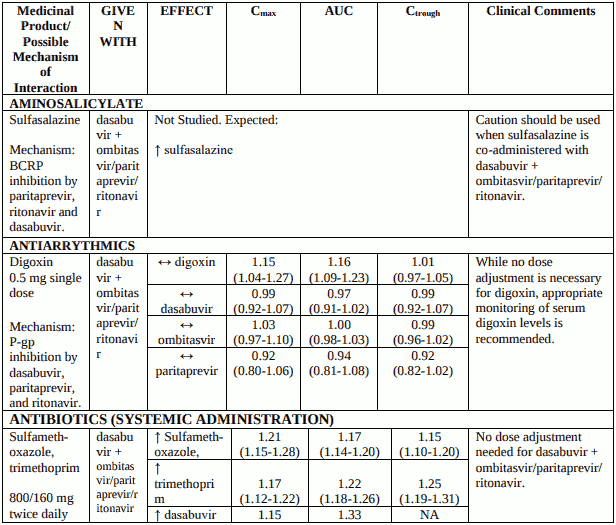
Dasabuvir is an inhibitor of BCRP in vivo. Co-administration of dasabuvir with ombitasvir/paritaprevir/ritonavir together with medicinal products that are substrates of BCRP may increase plasma concentrations of these transporter substrates, potentially requiring dose adjustment/clinical monitoring. Such medicinal products include sulfasalazine, imatinib and some of the statins (see Table 2). See also Table 2 for specific advice on rosuvastatin which has been evaluated in a drug interaction study.
Medicinal products transported by Pgp in the intestine
While dasabuvir is an in vitro inhibitor of P-gp, no significant change was observed in the exposure of the P-gp substrate, digoxin, when administered with dasabuvir with ombitasvir/paritaprevir/ritonavir. It may not be excluded that the systemic exposure of dabigatran etexilate is increased by dasabuvir due to inhibition of P-gp in the intestine.
Medicinal products metabolised by glucuronidation
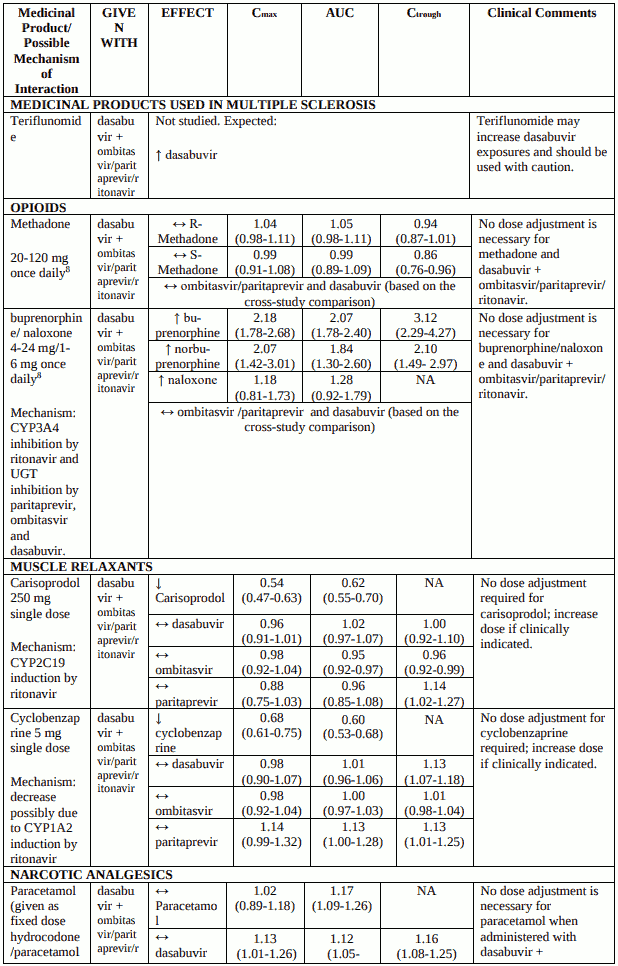
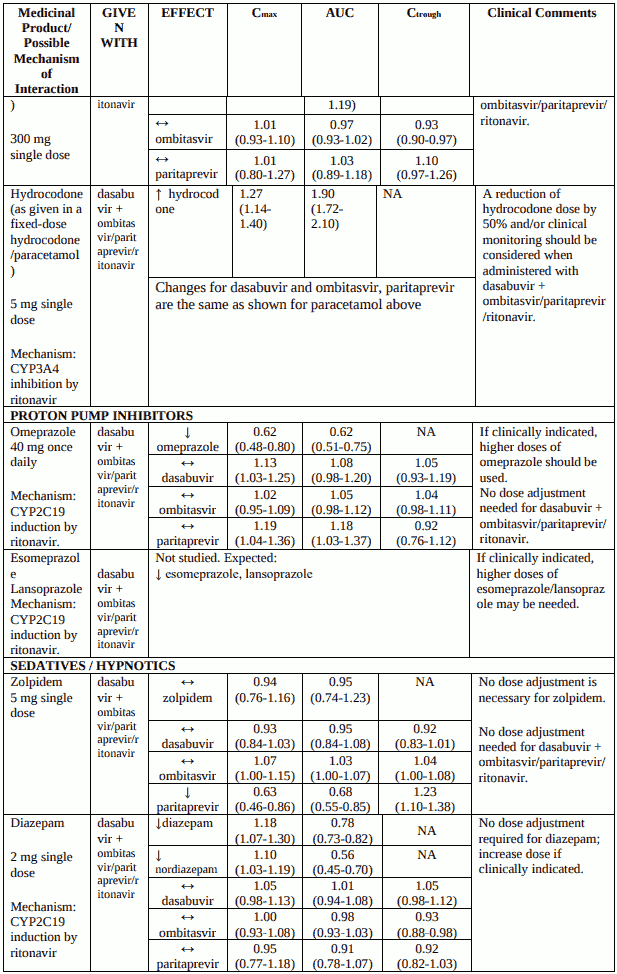
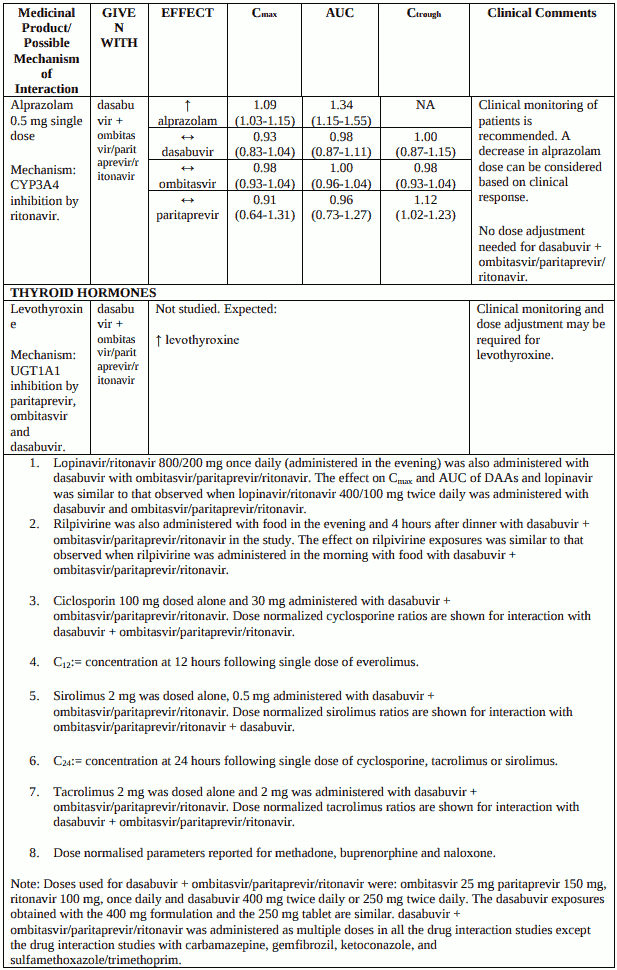
Dasabuvir is an inhibitor of UGT1A1 in vivo. Co-administration of dasabuvir with medicinal products that are primarily metabolized by UGT1A1 result in increased plasma concentrations of such medicinal products; routine clinical monitoring is recommended for narrow therapeutic index medicinal products (i.e. levothyroxine). See also Table 2 for specific advice on raltegravir and buprenorphine which have been evaluated in drug interaction studies. Dasabuvir has also been found to inhibit UGT1A4, 1A6 and intestinal UGT2B7 in vitro at in vivo relevant concentrations.
Medicinal products metabolised by CYP2C19
Co-administration of dasabuvir with ombitasvir/paritaprevir/ritonavir can decrease exposures of medicinal products that are metabolized by CYP2C19 (e.g. lansoprazole, esomeprazole, smephenytoin), which may require dose adjustment/clinical monitoring. CYP2C19 substrates evaluated in drug interaction studies include omeprazole and escitalopram (Table 2).
Medicinal products metabolised by CYP2C9
Dasabuvir administered with ombitasvir/paritaprevir/ritonavir did not affect the exposures of the CYP2C9 substrate warfarin. Other CYP2C9 substrates (NSAIDs (e.g. ibuprofen), antidiabetics (e.g. glimepiride, glipizide) are not expected to require dose adjustments.
Medicinal products metabolised by CYP2D6 or CYP1A2
Dasabuvir administered with ombitasvir/paritaprevir/ritonavir did not affect the exposures of the CYP2D6 /CYP1A2 substrate duloxetine. Exposures of cyclobenzaprine, a CYP1A2 substrate, were decreased. Clinical monitoring and dose adjustment may be needed for other CYP1A2 substrates (e.g. ciprofloxacin, cyclobenzaprine, theophylline and caffeine). CYP2D6 substrates (e.g. desipramine, metoprolol and dextromethorphan) are not expected to require dose adjustments.
Medicinal products renally excreted via transport proteins
Dasabuvir does not inhibit organic anion transporter (OAT1) in vivo as shown by the lack of interaction with tenofovir (OAT1 substrate). In vitro studies show that dasabuvir is not an inhibitor of organic cation transporters (OCT2), organic anion transporters (OAT3), or multidrug and toxin extrusion proteins (MATE1 and MATE2K) at clinically relevant concentrations.
Therefore, dasabuvir is not expected to affect medicinal products which are primarily excreted by the renal route via these transporters (see section 5.2).
Potential for other medicinal products to affect the pharmacokinetics of dasabuvir
Medicinal products that inhibit CYP2C8
Co-administration of dasabuvir with medicinal productsthat inhibit CYP2C8 (e.g. teriflunomide, deferasirox) may increase dasabuvir plasma concentrations. Strong CYP2C8 inhibitors are contraindicated with dasabuvir (see section 4.3 and Table 2).
Enzyme inducers
Co-administration of dasabuvir with medicinal products that are moderate or strong enzyme inducers is expected to decrease dasabuvir plasma concentrations and reduce its therapeutic effect. Contraindicated enzyme inducers are provided in section 4.3 and Table 2.
Dasabuvir is a substrate of P-gp and BCRP and its major metabolite M1 is a substrate of OCT1 in vitro. Inhibition of P-gp and BCRP is not expected to show clinically relevant increases in exposures of dasabuvir (Table 2).
Dasabuvir M1 metabolite was quantified in all the drug interaction studies. Changes in exposures of the metabolite were generally consistent with that observed with dasabuvir except for studies with CYP2C8 inhibitor, gemfibrozil, where the metabolite exposures decreased by up to 95% and CYP3A inducer, carbamazepine, where the metabolite exposures decreased by only up to 39%.
Patients treated with vitamin K antagonists
As liver function may change during treatment with dasabuvir administered with ombitasvir/paritaprevir/ritonavir, a close monitoring of International Normalised Ratio (INR) values is recommended.
Drug interaction studies
Recommendations for co-administration of dasabuvir with ombitasvir/paritaprevir/ritonavir for a number of medicinal products are provided in Table 2.
If a patient is already taking medicinal product(s) or initiating a medicinal product while receiving dasabuvir and ombitasvir/paritaprevir/ritonavir for which potential for drug interaction is expected, dose adjustment of the concomitant medicinal product(s) or appropriate clinical monitoring should be considered (Table 2).
If dose adjustments of concomitant medicinal products are made due to treatment with dasabuvir and ombitasvir/paritaprevir/ritonavir, doses should be re-adjusted after administration of dasabuvir and ombitasvir/paritaprevir/ritonavir is completed.
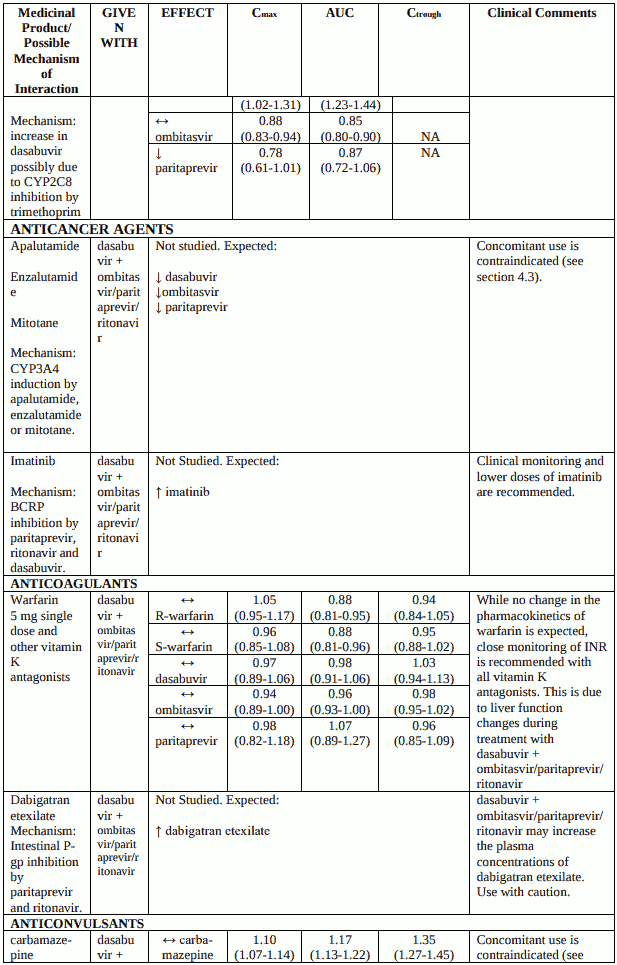
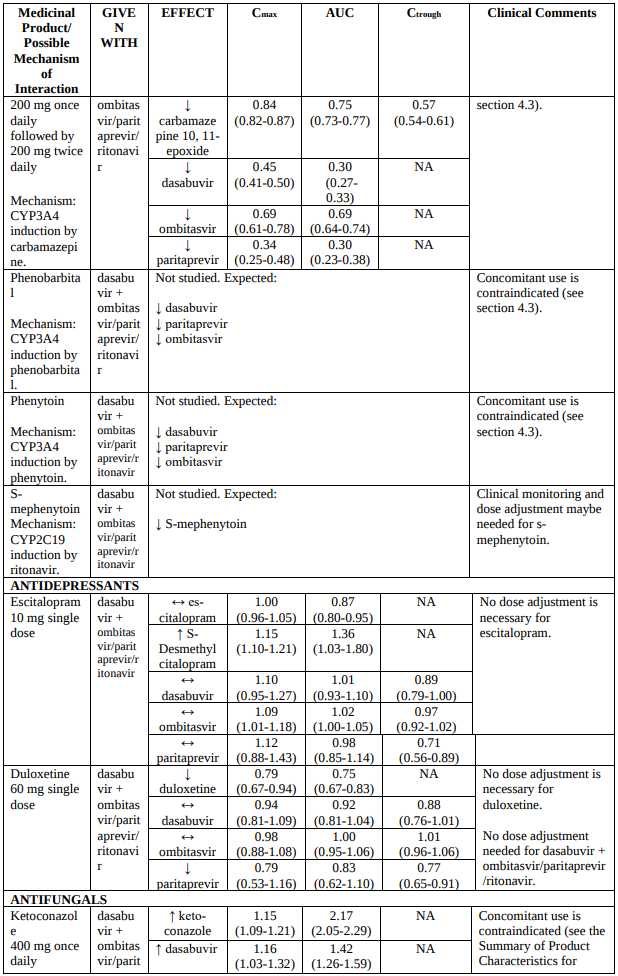
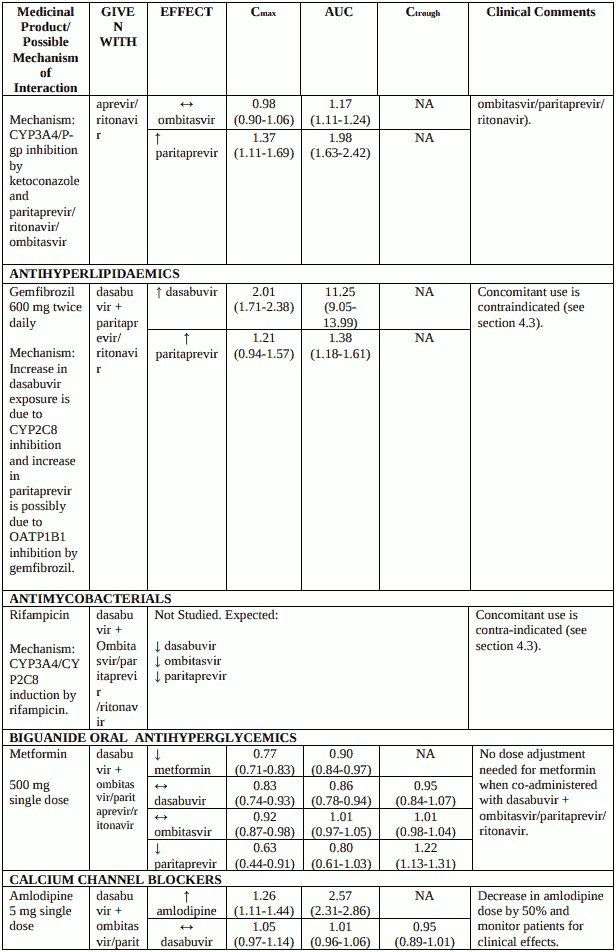
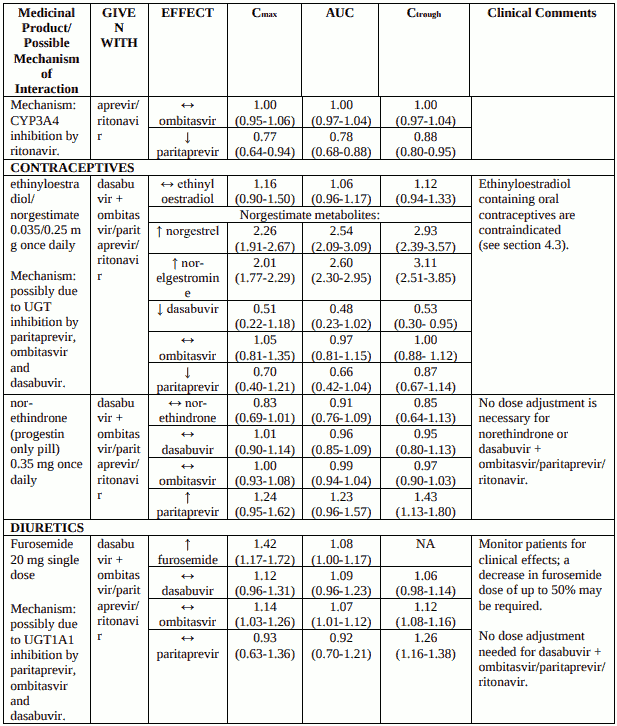
Table 2 provides the Least Squares Means Ratio (90% Confidence Interval) effect on concentration of dasabuvir and ombitasvir/paritaprevir/ritonavir and concomitant medicinal products. The direction of the arrow indicates the direction of the change in exposures (Cmax, and AUC) in the paritaprevir, ombitasvir, dasabuvir and the co-administered medicinal product (↑= increase more than 20%, ↓ = decrease more than 20%, ↔ = no change or change less than 20%).
This is not an exclusive list. Dasabuvir is administered with ombitasvir/paritaprevir/ritonavir. For interactions with ombitasvir/paritaprevir/ritonavir refer to the Summary of Product Characteristics.
Table 2. Interactions between dasabuvir with ombitasvir/paritaprevir/ritonavir and other medicinal products:
Paediatric population
Drug interaction studies have only been performed in adults.
Fertility, pregnancy and lactation
Women of childbearing potential/contraception in males and females
Extreme caution must be taken to avoid pregnancy in female patients and female partners of male patients when dasabuvir is used with ribavirin. Significant teratogenic and/or embryocidal effects have been demonstrated in all animal species exposed to ribavirin; therefore, ribavirin is contraindicated in women who are pregnant and in the male partners of women who are pregnant. Refer to the Summary of Product Characteristics for ribavirin for additional information.
Female patients: Women of childbearing potential should not receive ribavirin unless they are using an effective form of contraception during treatment with ribavirin and for 4 months after treatment.
Male patients and their female partners: Either male patients or their female partners of childbearing potential must use a form of effective contraception during treatment with ribavirin and for 7 months after treatment.
Ethinyloestradiol is contraindicated in combination with dasabuvir (see section 4.3). See additional information on specific hormonal contraceptives in sections 4.3 and 4.4.
Pregnancy
There are very limited data from the use of dasabuvir in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity (see section 5.3). As a precautionary measure, it is preferable to avoid the use of dasabuvir during pregnancy.
If ribavirin is co-administered with dasabuvir and ombitasvir/paritaprevir/ritonavir, the contraindications regarding use of ribavirin during pregnancy apply (see also the Summary of Product Characteristics of ribavirin).
Breast-feeding
It is not known whether dasabuvir and metabolites are excreted in human breast milk. Available pharmacokinetic data in animals have shown excretion of dasabuvir and metabolites in milk (see section 5.3). Because of the potential for adverse reactions from the medicinal product in breastfed infants, a decision must be made whether to discontinue breastfeeding or discontinue treatment with dasabuvir, taking into account the importance of the therapy to the mother. Patients receiving ribavirin should also refer to the Summary of Product Characteristics of ribavirin.
Fertility
No human data on the effect of dasabuvir on fertility are available. Animal studies do not indicate harmful effects on fertility (see section 5.3).
Effects on ability to drive and use machines
Dasabuvir has no or negligible influence on the ability to drive and use machines. Patients should be informed that fatigue has been reported during treatment with dasabuvir in combination with ombitasvir/paritaprevir/ritonavir and ribavirin (see section 4.8).
Undesirable effects
Summary of the safety profile
In subjects receiving dasabuvir and ombitasvir/paritaprevir/ritonavir with ribavirin, the most commonly reported adverse reactions (greater than 20% of subjects) were fatigue and nausea. The proportion of subjects who permanently discontinued treatment due to adverse reactions was 0.2% (5/2,044) and 4.8% (99/2,044) of subjects had ribavirin dose reductions due to adverse reactions.
Tabulated list of adverse reactions
The safety summary is based on pooled data from phase 2 and 3 clinical trials in subjects who received dasabuvir and ombitasvir/paritaprevir/ritonavir with or without ribavirin. The majority of adverse reactions presented in Table 3 were of grade 1 severity in dasabuvir- and ombitasvir/paritaprevir/ritonavir-containing regimens.
The adverse reactions are listed below by system organ class and frequency. Frequencies are defined as follows: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000) or very rare (<1/10,000).
Table 3. Adverse reactions identified with dasabuvir in combination with ombitasvir/paritaprevir/ritonavir or ombitasvir/paritaprevir/ritonavir and ribavirin:
| Frequency | dasabuvir and ombitasvir/paritaprevir/ritonavir + ribavirin* N=2,044 | dasabuvir and ombitasvir/paritaprevir/ritonavir N=588 |
|---|---|---|
| Blood and lymphatic system disorders | ||
| Common | Anaemia | |
| Immune system disorders | ||
| Frequency unknown | Anaphylactic reactions | Anaphylactic reactions |
| Metabolism and nutrition disorders | ||
| Uncommon | Dehydration | |
| Psychiatric disorders | ||
| Very common | Insomnia | |
| Gastrointestinal disorders | ||
| Very common | Nausea, Diarrhoea | |
| Common | Vomiting | |
| Hepatobiliary disorders | ||
| Frequency unknown | Hepatic decompensation and hepatic failure | Hepatic decompensation and hepatic failure |
| Skin and subcutaneous tissue disorders | ||
| Very common | Pruritus | |
| Common | Pruritus | |
| Rare | Angioedema | Angioedema |
| General disorders and administration and administration site conditions | ||
| Very common | Asthenia, Fatigue | |
* Data set includes all genotype 1-infected subjects in Phase 2 and 3 trials including subjects with cirrhosis. Note: For laboratory abnormalities refer to Table 4.
Description of selected adverse reactions
Compared to subjects without cirrhosis, in subjects with compensated cirrhosis there was an increased rate of indirect hyperbilirubinemia when ribavirin was part of the regimen.
Laboratory abnormalities
Changes in selected laboratory parameters are described in Table 4. A side-by-side tabulation is provided to simplify presentation; direct comparisons should not be made across trials that differ in trial designs.
Table 4. Selected treatment emergent laboratory abnormalities
| Laboratory parameters | SAPPHIRE I and II | PEARL II, III, and IV | TURQUOISE II (subjects with cirrhosis) |
|---|---|---|---|
| dasabuvir and ombitasvir/paritaprevir/ritonavir + ribavirin 12 weeks N=770 n(%) | dasabuvir and ombitasvir/paritaprevir/ritonavir 12 weeks N=509 n(%) | dasabuvir and ombitasvir/paritaprevir/ritonavir + ribavirin 12 or 24 weeks N=380 n(%) | |
| ALT | |||
| >5-20 × ULN* (Grade 3) | 6/765 (0.8%) | 1/509 (0.2%) | 4/380 (1.1%) |
| >20 × ULN (Grade 4) | 3/765 (0.4%) | 0 | 2/380 (0.5%) |
| Haemoglobin | |||
| <100-80 g/L (grade 2) | 41/765 (5.4%) | 0 | 30/380 (7.9%) |
| <80-65 g/L (grade 3) | 1/765 (0.1%) | 0 | 3/380 (0.8%) |
| <65 g/L (Grade 4) | 0 | 0 | 1/380 (0.3%) |
| Total bilirubin | |||
| >3-10 × ULN (grade 3) | 19/765 (2.5%) | 2/509 (0.4%) | 37/380 (9.7%) |
| >10 × ULN (grade 4) | 1/765 (0.1%) | 0 | 0 |
* ULN: Upper Limit of Normal
Serum ALT elevations
In a pooled analysis of clinical trials with dasabuvir and ombitasvir/paritaprevir/ritonavir with and without ribavirin, 1% of subjects experienced serum ALT levels greater than 5 times the upper limit of normal (ULN) after starting treatment. As the incidence of such elevations was 26% among women taking a concomitant ethinyloestradiol-containing medicine, such medicinal products are contraindicated with dasabuvir and ombitasvir/paritaprevir/ritonavir. No increase in incidence of ALT elevations was observed with other types of systemic oestrogens commonly used for hormone replacement therapy (e.g., oestradiol and conjugated oestrogens). ALT elevations were typically asymptomatic, generally occurred during the first 4 weeks of treatment (mean time 20 days, range 8- 57 days) and most resolved with ongoing therapy. Two patients discontinued dasabuvir and ombitasvir/paritaprevir/ritonavir due to elevated ALT, including one on ethinyloestradiol. Three interrupted dasabuvir and ombitasvir/paritaprevir/ritonavir for one to seven days, including one on ethinyloestradiol. The majority of these ALT elevations were transient and assessed as related to dasabuvir and ombitasvir/paritaprevir/ritonavir. Elevations in ALT were generally not associated with bilirubin elevations. Cirrhosis was not a risk factor for elevated ALT (see section 4.4).
Serum bilirubin elevations
Transient elevations in serum bilirubin (predominantly indirect) were observed in subjects receiving dasabuvir and ombitasvir/paritaprevir/ritonavir with ribavirin, related to the inhibition of the bilirubin transporters OATP1B1/1B3 by paritaprevir and ribavirin-induced haemolysis. Bilirubin elevations occurred after initiation of treatment, peaked by study Week 1, and generally resolved with ongoing therapy. Bilirubin elevations were not associated with aminotransferase elevations. The frequency of indirect bilirubin elevations was lower among subjects who did not receive ribavirin.
Liver transplant recipients
The overall safety profile in HCV-infected transplant recipients who were administered dasabuvir and ombitasvir/paritaprevir/ritonavir and ribavirin (in addition to their immunosuppressant medicinal products) was similar to subjects treated with dasabuvir and ombitasvir/paritaprevir/ritonavir and ribavirin in phase 3 clinical trials, although some adverse reactions were increased in frequency. 10 subjects (29.4%) had at least one post baseline haemoglobin value of less than 10 g/dL. 10 of 34 subjects (29.4%) dose modified ribavirin due to decrease in haemoglobin and 2.9% (1/34) had an interruption of ribavirin. Ribavirin dose modification did not impact SVR rates. 5 subjects required erythropoietin, all of whom initiated ribavirin at the starting dose of 1000 to 1200 mg daily. No subject received a blood transfusion.
HIV/HCV co-infected patients
The overall safety profile in HCV/HIV-1 co-infected subjects was similar to that observed in HCV mono-infected subjects. Transient elevations in total bilirubin >3 x ULN (mostly indirect) occurred in 17 (27.0%) subjects; 15 of these subjects were receiving atazanavir. None of the subjects with hyperbilirubinemia had concomitant elevations of aminotransferases.
GT1-infected subjects with or without cirrhosis with severe renal impairment or end-stage renal disease (ESRD)
Dasabuvir and ombitasvir/paritaprevir/ritonavir with or without ribavirin were assessed in 68 subjects with genotype 1 infection with or without cirrhosis who have severe renal impairment or ESRD (see Section 5.1). The overall safety profile in subjects with severe renal impairment was similar to that seen in prior Phase 3 studies in subjects without severe renal impairment, except that a greater proportion of subjects required intervention due to ribavirin-associated decreases in serum haemoglobin. The mean baseline haemoglobin level was 12.1 g/dL and the mean decline in haemoglobin at the end of treatment for subjects taking RBV was 1.2 g/dL. Thirty-nine of the 50 subjects who received ribavirin required interruption of ribavirin, and 11 of these subjects were also treated with erythropoietin. Four subjects experienced a haemoglobin level <8 g/dL. Two subjects received a blood transfusion. Adverse events of anaemia were not seen in the 18 GT1b-infected subjects who did not receive ribavirin. Ombitasvir/paritaprevir/ritonavir with or without dasabuvir was also evaluated without ribavirin in 18 GT1a- and GT4-infected patients; no adverse events of anaemia were seen in these subjects.
Paediatric population
The safety of dasabuvir in children and adolescents aged < 18 years has not yet been established. No data are available.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.