GIOTRIF Film-coated tablet Ref.[6091] Active ingredients: Afatinib
Source: European Medicines Agency (EU) Revision Year: 2020 Publisher: Boehringer Ingelheim International GmbH, Binger Strasse 173, D-55216 Ingelheim am Rhein, Germany
Contraindications
Hypersensitivity to afatinib or to any of the excipients listed in section 6.1.
Special warnings and precautions for use
Assessment of EGFR mutation status
When assessing the EGFR mutation status of a patient, it is important that a well-validated and robust methodology is chosen to avoid false negative or false positive determinations.
Diarrhoea
Diarrhoea, including severe diarrhoea, has been reported during treatment with GIOTRIF (see section 4.8). Diarrhoea may result in dehydration with or without renal impairment, which in rare cases has resulted in fatal outcomes. Diarrhoea usually occurred within the first 2 weeks of treatment. Grade 3 diarrhoea most frequently occurred within the first 6 weeks of treatment.
Proactive management of diarrhoea including adequate hydration combined with anti-diarrhoeal medicinal products especially within the first 6 weeks of the treatment is important and should start at first signs of diarrhoea. Antidiarrhoeal medicinal products (e.g. loperamide) should be used and if necessary their dose should be escalated to the highest recommended approved dose. Anti-diarrhoeal medicinal products should be readily available to the patients so that treatment can be initiated at first signs of diarrhoea and continued until loose bowel movements cease for 12 hours. Patients with severe diarrhoea may require interruption and dose reduction or discontinuation of therapy with GIOTRIF (see section 4.2). Patients who become dehydrated may require administration of intravenous electrolytes and fluids.
Skin related adverse events
Rash/acne has been reported in patients treated with this medicinal product (see section 4.8). In general, rash manifests as a mild or moderate erythematous and acneiform rash, which may occur or worsen in areas exposed to sun. For patients who are exposed to sun, protective clothing, and use of sun screen is advisable. Early intervention (such as emollients, antibiotics) of dermatologic reactions can facilitate continuous GIOTRIF treatment. Patients with severe skin reactions may also require temporary interruption of therapy, dose reduction (see section 4.2), additional therapeutic intervention, and referral to a specialist with expertise in managing these dermatologic effects.
Bullous, blistering and exfoliative skin conditions have been reported including rare cases suggestive of Stevens-Johnson syndrome and toxic epidermal necrolysis. Treatment with this medicinal product should be interrupted or discontinued if the patient develops severe bullous, blistering or exfoliating conditions (see section 4.8).
Female gender, lower body weight, and underlying renal impairment
Higher exposure to afatinib has been observed in female patients, patients with lower body weight and those with underlying renal impairment (see section 5.2). This could result in a higher risk of developing adverse reactions in particular diarrhoea, rash/acne and stomatitis. Closer monitoring is recommended in patients with these risk factors.
Interstitial Lung Disease (ILD)
There have been reports of ILD or ILD-like adverse reactions (such as lung infiltration, pneumonitis, acute respiratory distress syndrome, allergic alveolitis), including fatalities, in patients receiving GIOTRIF for treatment of NSCLC. ILD-like adverse reactions were reported in 0.7% of patients treated with GIOTRIF across all clinical trials (including 0.5% of patients with CTCAE Grade ≥ 3 ILD-like adverse reactions). Patients with a history of ILD have not been studied.
Careful assessment of all patients with an acute onset and/or unexplained worsening of pulmonary symptoms (dyspnoea, cough, fever) should be performed to exclude ILD. Treatment with this medicinal product should be interrupted pending investigation of these symptoms. If ILD is diagnosed, GIOTRIF should be permanently discontinued and appropriate treatment initiated as necessary (see section 4.2).
Severe hepatic impairment
Hepatic failure, including fatalities, has been reported during treatment with this medicinal product in less than 1% of patients. In these patients, confounding factors have included pre-existing liver disease and/or comorbidities associated with progression of underlying malignancy. Periodic liver function testing is recommended in patients with pre-existing liver disease. In the pivotal trials Grade 3 alanine aminotransferase (ALT) and aspartate aminotransferase (AST) elevations were observed in 2.4% (LUX-Lung-3) and 1.6% (LUX-Lung 8) of patients with normal baseline liver tests treated with 40 mg/day. In LUX-Lung-3 Grade 3 ALT/AST elevations were about 3.5 fold higher in patients with abnormal baseline liver tests. There were no Grade 3 ALT/AST elevations in patients with abnormal baseline liver tests in LUX-Lung 8 (see section 4.8). Dose interruption may become necessary in patients who experience worsening of liver function (see section 4.2). In patients who develop severe hepatic impairment while taking GIOTRIF, treatment should be discontinued.
Gastrointestinal perforations
Gastrointestinal perforation, including fatalities, has been reported during treatment with GIOTRIF in 0.2% of patients across all randomized controlled clinical trials. In the majority of cases, gastrointestinal perforation was associated with other known risk factors, including concomitant medications such as corticosteroids, NSAIDs, or anti-angiogenic agents, an underlying history of gastrointestinal ulceration, underlying diverticular disease, age, or bowel metastases at sites of perforation. In patients who develop gastrointestinal perforation while taking GIOTRIF, treatment should be permanently discontinued.
Keratitis
Symptoms such as acute or worsening eye inflammation, lacrimation, light sensitivity, blurred vision, eye pain and/or red eye should be referred promptly to an ophthalmology specialist. If a diagnosis of ulcerative keratitis is confirmed, treatment should be interrupted or discontinued. If keratitis is diagnosed, the benefits and risks of continuing treatment should be carefully considered. This medicinal product should be used with caution in patients with a history of keratitis, ulcerative keratitis or severe dry eye. Contact lens use is also a risk factor for keratitis and ulceration (see section 4.8).
Left ventricular function
Left ventricular dysfunction has been associated with HER2 inhibition. Based on the available clinical trial data, there is no suggestion that this medicinal product causes an adverse reaction on cardiac contractility. However, this medicinal product has not been studied in patients with abnormal left ventricular ejection fraction (LVEF) or those with significant cardiac history. In patients with cardiac risk factors and those with conditions that can affect LVEF, cardiac monitoring, including an assessment of LVEF at baseline and during treatment, should be considered. In patients who develop relevant cardiac signs/symptoms during treatment, cardiac monitoring including LVEF assessment should be considered.
In patients with an ejection fraction below the institution's lower limit of normal, cardiac consultation as well as treatment interruption or discontinuation should be considered.
P-glycoprotein (P-gp) interactions
Concomitant treatment with strong inducers of P-gp may decrease exposure to afatinib (see section 4.5).
Lactose
This medicinal product contains lactose. Patients with rare hereditary conditions of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.
Interaction with other medicinal products and other forms of interaction
Interactions with drug transport systems
Effects of P-gp and breast cancer resistance protein (BCRP) inhibitors on afatinib
In vitro studies have demonstrated that afatinib is a substrate of P-gp and BCRP. When the strong P-gp and BCRP inhibitor ritonavir (200 mg twice a day for 3 days) was administered 1 hour before a single dose of 20 mg GIOTRIF, exposure to afatinib increased by 48% (area under the curve (AUC0-∞)) and 39% (maximum plasma concentration (Cmax)). In contrast, when ritonavir was administered simultaneously or 6 hours after 40 mg GIOTRIF, the relative bioavailability of afatinib was 119% (AUC0-∞) and 104% (Cmax) and 111% (AUC0-∞) and 105% (Cmax), respectively. Therefore, it is recommended to administer strong P-gp inhibitors (including but not limited to ritonavir, cyclosporine A, ketoconazole, itraconazole, erythromycin, verapamil, quinidine, tacrolimus, nelfinavir, saquinavir, and amiodarone) using staggered dosing, preferably 6 hours or 12 hours apart from GIOTRIF (see section 4.2).
Effects of P-gp inducers on afatinib
Pre-treatment with rifampicin (600 mg once daily for 7 days), a potent inducer of P-gp, decreased the plasma exposure to afatinib by 34% (AUC0-∞) and 22% (Cmax) after administration of a single dose of 40 mg GIOTRIF. Strong P-gp inducers (including but not limited to rifampicin, carbamazepine, phenytoin, phenobarbital or St. John's wort (Hypericum perforatum)) may decrease exposure to afatinib (see section 4.4).
Effects of afatinib on P-gp substrates
Based on in vitro data, afatinib is a moderate inhibitor of P-gp. However, based on clinical data it is considered unlikely that GIOTRIF treatment will result in changes of the plasma concentrations of other P-gp substrates.
Interactions with BCRP
In vitro studies indicated that afatinib is a substrate and an inhibitor of the transporter BCRP. Afatinib may increase the bioavailability of orally administered BCRP substrates (including but not limited to rosuvastatin and sulfasalazine
Food effect on afatinib
Co-administration of a high-fat meal with GIOTRIF resulted in a significant decrease of exposure to afatinib by about 50% in regard to Cmax and 39% in regard to AUC0-∞. This medicinal product should be administered without food (see sections 4.2 and 5.2).
Pregnancy and lactation
Women of childbearing potential
As a precautionary measure, women of childbearing potential should be advised to avoid becoming pregnant while receiving treatment with GIOTRIF. Adequate contraceptive methods should be used during therapy and for at least 1 month after the last dose.
Pregnancy
Mechanistically, all EGFR targeting medicinal products have the potential to cause foetal harm. Animal studies with afatinib did not indicate direct or indirect harmful effects with respect to reproductive toxicity (see section 5.3). Studies in animals have shown no signs of teratogenicity up to and including maternally lethal dose levels. Adverse changes were restricted to toxic dose levels. However, systemic exposures achieved in animals were either in a similar range or below the levels observed in patients (see section 5.3).
There are no or limited amount of data from the use of this medicinal product in pregnant women. The risk for humans is thus unknown. If used during pregnancy or if the patient becomes pregnant while or after receiving GIOTRIF, she should be informed of the potential hazard to the foetus.
Breast-feeding
Available pharmacokinetic data in animals have shown excretion of afatinib in milk (see section 5.3). Based on this, it is likely that afatinib is excreted in human milk. A risk to the breast-feeding child cannot be excluded. Mothers should be advised against breast-feeding while receiving this medicinal product.
Fertility
Fertility studies in humans have not been performed with afatinib. Available non-clinical toxicology data have shown effects on reproductive organs at higher doses. Therefore, an adverse effect of this medicinal product on human fertility cannot be excluded.
Effects on ability to drive and use machines
GIOTRIF has minor influence on the ability to drive and use machines. During treatment, ocular adverse reactions (conjunctivitis, dry eye, keratitis) have been reported in some patients (see section 4.8) which may affect patients ability to drive or use machines.
Undesirable effects
Summary of the safety profile
The types of adverse reactions (ADRs) were generally associated with the EGFR inhibitory mode of action of afatinib. The summary of all ADRs is shown in Table 2. The most frequent ADRs were diarrhoea and skin related adverse events (see section 4.4) as well as stomatitis and paronychia (see also Table 3, 4 and 5). Overall, dose reduction (see section 4.2) led to a lower frequency of common adverse reactions.
In patients treated with once daily GIOTRIF 40 mg, dose reductions due to ADRs occurred in 57% of the patients in the LUX-Lung 3 trial and in 25% of the patients in the LUX-Lung 8 trial. Discontinuation due to
ADRs diarrhoea and rash/acne was 1.3% and 0% in LUX-Lung 3 and 3.8% and 2.0% in LUX-Lung 8, respectively.
ILD-like adverse reactions were reported in 0.7% of afatinib treated patients. Bullous, blistering and exfoliative skin conditions have been reported including rare cases suggestive of Stevens-Johnson syndrome and toxic epidermal necrolysis although in these cases there were potential alternative aetiologies (see section 4.4).
Tabulated list of adverse reactions
Table 2 summarises the frequencies of ADRs from all NSCLC trials and from post-marketing experience with daily GIOTRIF doses of 40 mg or 50 mg as monotherapy. The following terms are used to rank the ADRs by frequency: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.
Table 2. Summary of ADRs per frequency category:
Infections and infestations
Very common: Paronychia^1^
Common: Cystitis
Metabolism and nutrition disorders
Very common: Decreased appetite
Common: Dehydration, Hypokalaemia
Nervous system disorders
Common: Dysgeusia
Eye disorders
Common: Conjunctivitis, Dry eye
Uncommon: Keratitis
Respiratory, thoracic and mediastinal disorders
Very common: Epistaxis
Common: Rhinorrhoea
Uncommon: Interstitial lung disease
Gastrointestinal disorders
Very common: Diarrhoea, Stomatitis^2^, Nausea, Vomiting
Common: Dyspepsia, Cheilitis
Uncommon: Pancreatitis, Gastrointestinal perforation
Hepatobiliary disorders
Common: Alanine aminotransferase increased, Aspartate aminotransferase increased
Skin and subcutaneous tissue disorders
Very common: Rash^3^, Dermatitis acneiform^4^, Pruritus^5^, Dry skin^6^
Common: Palmar-plantar erythrodysaesthesia syndrome, Nail disorders^8^
Rare: Stevens-Johnson syndrome^7^, Toxic epidermal necrolysis^7^
Musculoskeletal and connective tissue disorders
Common: Muscle spasms
Renal and urinary disorders
Common: Renal impairment/Renal failure
General disorders and administration site conditions
Common: Pyrexia
Investigations
Common: Weight decreased
1 Includes Paronychia, Nail infection, Nail bed infection
2 Includes Stomatitis, Aphthous stomatitis, Mucosal inflammation, Mouth ulceration, Oral mucosa erosion, Mucosal erosion, Mucosal ulceration
3 Includes group of rash preferred terms
4 Includes Acne, Acne pustular, Dermatitis acneiform
5 Includes Pruritus, Pruritus generalised
6 Includes Dry skin, Skin chapped
7 Based on post-marketing experience
8 Includes Nail disorder, Onycholysis, Nail toxicity, Onychoclasis, Ingrowing nail, Nail pitting, Onychomadesis, Nail discoloration, Nail dystrophy, Nail ridging, and Onychogryphosis
Description of selected adverse reactions
Very common ADRs in GIOTRIF-treated patients occurring in at least 10% of patients in trial LUX-Lung 3 and LUX-Lung 7 are summarised by National Cancer Institute-Common Toxicity Criteria (NCI-CTC) Grade in Tables 3 and 4.
Table 3. Very common ADRs in trial LUX-Lung 3:
| GIOTRIF (40 mg/ημέρα) N=229 | Pemetrexed/Cisplatin N=111 | |||||
|---|---|---|---|---|---|---|
| NCI-CTC Grade | Any Grade | 3 | 4 | Any Grade | 3 | 4 |
| MedDRA Preferred Term | % | % | % | % | % | % |
| Infections and infestations | ||||||
| Paronychia1 | 57,6 | 11,4 | 0 | 0 | 0 | 0 |
| Metabolism and nutrition disorders | ||||||
| Decreased appetite | 20,5 | 3,1 | 0 | 53,2 | 2,7 | 0 |
| Respiratory, thoracic and mediastinal disorders | ||||||
| Epistaxis | 13,1 | 0 | 0 | 0,9 | 0,9 | 0 |
| Gastrointestinal disorders | ||||||
| Diarrhoea | 95,2 | 14,4 | 0 | 15,3 | 0 | 0 |
| Stomatitis2 | 69,9 | 8,3 | 0,4 | 13,5 | 0,9 | 0 |
| Cheilitis | 12,2 | 0 | 0 | 0,9 | 0 | 0 |
| Skin and subcutaneous tissue disorders | ||||||
| Rash3 | 70,3 | 14 | 0 | 6,3 | 0 | 0 |
| Dermatitis acneiform4 | 34,9 | 2,6 | 0 | 0 | 0 | 0 |
| Dry skin5 | 29,7 | 0,4 | 0 | 1,8 | 0 | 0 |
| Pruritus6 | 19,2 | 0,4 | 0 | 0,9 | 0 | 0 |
| Investigations | ||||||
| Weight decreased | 10,5 | 0 | 0 | 9,0 | 0 | 0 |
1 Includes Paronychia, Nail infection, Nail bed infection
2 Includes Stomatitis, Aphthous stomatitis, Mucosal inflammation, Mouth ulceration, Oral mucosa erosion, Mucosal erosion, Mucosal ulceration
3 Includes group of rash preferred terms
4 Includes Acne, Acne pustular, Dermatitis acneiform
5 Includes Dry skin, Skin chapped
6 Includes Pruritus, Pruritus generalised
Table 4. Very common ADRs in trial LUX-Lung 7:
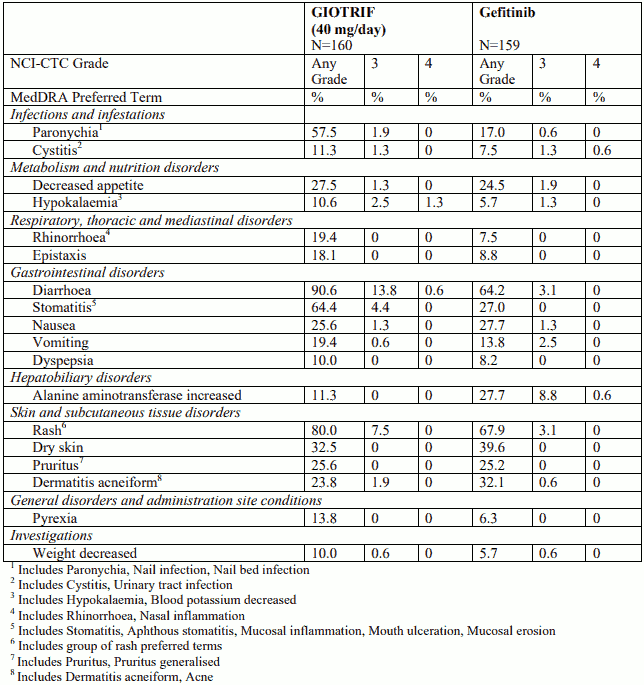
Liver function test abnormalities
Liver function test abnormalities (including elevated ALT and AST) were observed in patients receiving GIOTRIF 40 mg. These elevations were mainly transient and did not lead to discontinuation. Grade 2 (>2.5 to 5.0 times upper limit of normal (ULN)) ALT elevations occurred in <8% of patients treated with this medicinal product. Grade 3 (>5.0 to 20.0 times ULN) elevations occurred in <4% of patients treated with GIOTRIF (see section 4.4).
Description of selected adverse reactions
Very common ADRs in GIOTRIF-treated patients occurring in at least 10% of patients in trial LUX-Lung 8 are summarised by National Cancer Institute-Common Toxicity Criteria (NCI-CTC) Grade in Table 5.
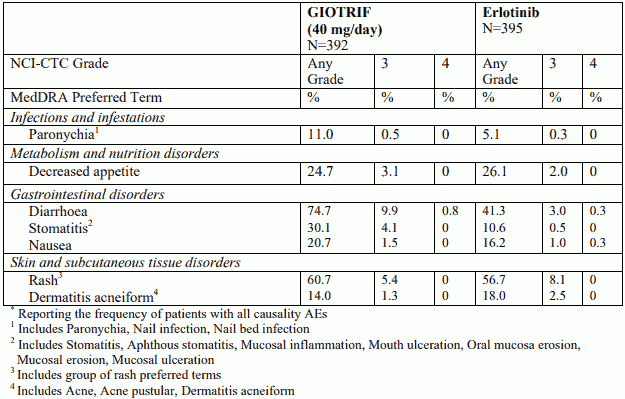
Table 5. Very common ADRs in trial LUX-Lung 8*:
Liver function test abnormalities
Liver function test abnormalities (including elevated ALT and AST) were observed in patients receiving GIOTRIF 40 mg. These elevations were mainly transient and did not lead to discontinuation. Grade 2 ALT elevations occurred in 1% and Grade 3 elevations occurred in 0.8% of patients treated with GIOTRIF (see section 4.4).
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.