KYNMOBI Sublingual film Ref.[10859] Active ingredients: Apomorphine
Source: FDA, National Drug Code (US) Revision Year: 2020
12.1. Mechanism of Action
KYNMOBI is a non-ergoline dopamine agonist with high in vitro binding affinity for the dopamine D4 receptor, and moderate affinity for the dopamine D2, D3, and D5, and adrenergic α1D, α2B, α2C receptors. The precise mechanism of action of KYNMOBI as a treatment for "off" episodes associated with Parkinson's disease is unknown, although it is believed to be due to stimulation of post-synaptic dopamine D2-type receptors within the caudate-putamen in the brain.
12.2. Pharmacodynamics
Cardiac Electrophysiology
In a thorough QT study with subcutaneous apomorphine at exposures similar to those achieved with the recommended subcutaneous apomorphine dosing (i.e, 6 mg), apomorphine resulted in a prolongation of QTcF of 10 msec (90% upper confidence interval of 16 msec). The thorough QT study also identified a significant exposure-response relationship between apomorphine concentration and QTcF.
Although the extent of the exposure and the Cmax of apomorphine are lower following the maximum recommended dose of KYNMOBI (30 mg) than following the maximum recommend dose of subcutaneous apomorphine (6 mg), QTc prolongation with KYNMOBI cannot be excluded.
Decreases in Blood Pressure
In Study 1, systolic orthostatic hypotension (reduction of 20 mmHg or more in standing minus supine/sitting systolic blood pressure) or diastolic hypotension (10 mmHg or more for standing minus supine/sitting diastolic blood pressure) occurred in 43% of patients treated with KYNMOBI, compared to 36% of patients who received placebo [see Warnings and Precautions (5.4) and Drug Interactions (7.2, 7.3)].
12.3. Pharmacokinetics
Absorption
Following sublingual administration of 15 mg of apomorphine, the time to maximum concentration (Tmax) ranged from 0.5 to 1 hour. Apomorphine exhibits less than dose proportional increase in exposures over a dose range of 10 mg to 35 mg (1.2 times the highest recommended dosage) following a single sublingual administration of KYNMOBI in patients with Parkinson's disease.
Distribution
Following sublingual administration of 15 mg of apomorphine, the geometric mean (CV%) of the apparent volume of distribution was 3630 L (66%).
Elimination
12.3.114 SPL UNCLASSIFIED SECTION
Metabolism
The major metabolic pathways for sublingual apomorphine are sulfation by multiple sulfotransferase (SULT) enzymes; glucuronidation by multiple glycosyltransferase (UGT) enzymes; N-demethylation catalyzed by multiple enzymes, including CYP2B6, CYP2C8, and CYP3A4/5; followed by conjugation. Metabolism of sublingual apomorphine results in three major inactive metabolites: apomorphine sulfate, apomorphine glucuronide, and norapomorphine glucuronide.
12.3.115 SPL UNCLASSIFIED SECTION
Excretion
Following sublingual administration of 15 mg of apomorphine, the geometric mean (CV%) of the apparent clearance was 1440 L/h (68%), and the geometric mean of the terminal elimination half-life is about 1.7 hours (range about 0.8 hour to 3 hours).
Specific Populations
The apparent clearance of apomorphine does not appear to be influenced by age, gender, race, weight, duration of Parkinson's disease, levodopa dose, use of antiemetic, or duration of therapy.
Renal Impairment
The clinical studies of KYNMOBI included patients with mild renal impairment (CLcr of ≥60 mL/min and <90 mL/min). There were no differences in apomorphine exposure after administration of KYNMOBI in patients with mild renal impairment as compared to patients with normal renal function (CLcr of ≥90 mL/min). Studies with KYNMOBI in patients with moderate to severe renal impairment have not been conducted.
In a study with subcutaneous apomorphine comparing patients with moderate renal impairment (as determined by estimated creatinine clearance) to healthy matched volunteers, the AUC0-∞ and Cmax values were increased by approximately 16% and 50%, respectively, following a single administration. The mean time to peak concentrations and the mean terminal half-life of apomorphine were unaffected by the renal status of the individual.
Since the Cmax and AUC0-∞ of apomorphine following the sublingual administration are lower as compared to the subcutaneous route of administration and the KYNMOBI dose is titrated individually, these changes are not expected to be clinically significant for patients with mild or moderate renal impairment [see Use in Specific Populations (8.6)].
Hepatic Impairment
Studies with KYNMOBI in patients with hepatic impairment have not been conducted.
In a study with subcutaneous apomorphine comparing patients with moderate hepatic impairment (as determined by the Child-Pugh classification method) to healthy matched volunteers, the AUC0-∞ and Cmax values were increased by approximately 10% and 25%, respectively, following a single administration. These changes are not expected to be clinically significant for patients with mild or moderate hepatic impairment [see Use in Specific Populations (8.7)].
Drug Interaction Studies
Carbidopa/levodopa
Levodopa pharmacokinetics were unchanged when subcutaneous apomorphine and levodopa were co-administrated in patients. However, motor response differences were significant. The threshold levodopa concentration necessary for an improved motor response was reduced significantly, leading to an increased duration of effect without a change in the maximal response to levodopa therapy.
Nitroglycerin
Co-administration of nitroglycerin (0.4 mg) with subcutaneous apomorphine in healthy subjects did not have a significant impact on the pharmacokinetics of apomorphine. However, concomitant administration of nitroglycerin (0.4 mg) with subcutaneous apomorphine caused greater decreases in blood pressure than with subcutaneous apomorphine alone [see Warnings and Precautions (5.4) and Drug Interactions (7.2)].
When nitroglycerin and subcutaneous apomorphine were concomitantly administered to healthy subjects, the mean largest decrease (the mean of each subject's largest drop in blood pressure measured within the 6-hour period following administration of subcutaneous apomorphine) in supine systolic and diastolic blood pressure (measured over 6 hours) was 9.7 mm Hg and 9.3 mm Hg, respectively. The mean largest decrease in standing systolic and diastolic blood pressure was 14.3 mm Hg and 13.5 mm Hg, respectively. Some individuals experienced very large decreases in standing systolic and diastolic blood pressure, up to a maximum decrease of 65 mm Hg and 43 mm Hg, respectively. In comparison, the mean largest decrease in supine systolic and diastolic blood pressure when subcutaneous apomorphine was administered alone was 6.1 mm Hg and 7.3 mm Hg, respectively, and in standing systolic and diastolic blood pressure was 6.7 mm Hg and 8.4 mm Hg, respectively.
A similar study has not been performed with KYNMOBI.
Ethanol
Co-administration of low dose ethanol (0.3 g/kg) with subcutaneous apomorphine in healthy subjects did not have a significant impact on the pharmacokinetics of apomorphine, but high dose ethanol (0.6 g/kg), equivalent to approximately 3 standardized alcohol-containing beverages, increased the Cmax of apomorphine by about 63%.
When high dose ethanol (0.6 g/kg) and subcutaneous apomorphine were concomitantly administered to healthy subjects, the mean largest decrease (the mean of each subject's largest drop in blood pressure measured within the 6-hour period following administration of subcutaneous apomorphine) for supine systolic and diastolic blood pressure was 9.1 mm Hg and 10.5 mm Hg, respectively. The mean largest standing systolic and diastolic blood pressure decrease was 11.3 mm Hg and 12.6 mm Hg, respectively. In some individuals, the decrease was as high as 61 mm Hg and 51 mm Hg, respectively, for standing systolic and diastolic blood pressure.
When low dose ethanol (0.3 g/kg) and subcutaneous apomorphine were concomitantly administered, the mean largest decrease in supine systolic and diastolic blood pressure was 10.2 mm Hg and 9.9 mm Hg, respectively. The mean largest decrease in standing systolic and diastolic blood pressure was 8.4 mm Hg and 7.1 mm Hg, respectively. In comparison, the mean largest decrease in supine systolic and diastolic blood pressure when subcutaneous apomorphine was administered alone was 6.1 mm Hg and 7.3 mm Hg, respectively, and in standing systolic and diastolic blood pressure was 6.7 mm Hg 8.4 mm Hg, respectively.
A similar study has not been performed with KYNMOBI.
COMT Interactions
A pharmacokinetic interaction of apomorphine with catechol-O-methyl transferase (COMT) inhibitors or drugs metabolized by this route is unlikely since apomorphine appears not to be metabolized by COMT.
In vitro studies
Based on in vitro studies, the potential for KYNMOBI to interact with concomitant medications to cause a CYP metabolism or transporter-based drug-drug interaction is considered low.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Lifetime carcinogenicity studies of apomorphine were conducted in male (0.1, 0.3, or 0.8 mg/kg/day) and female (0.3, 0.8, or 2 mg/kg/day) rats. Apomorphine was administered by subcutaneous injection for 22 months or 23 months, respectively. In males, there was an increase in Leydig cell tumors at the highest dose tested. This finding is of questionable significance because the endocrine mechanisms believed to be involved in the production of Leydig cell tumors in rats are not relevant to humans. No drug-related tumors were observed in females.
In a 26-week carcinogenicity study in P53-knockout transgenic mice, there was no evidence of carcinogenic potential when apomorphine was administered by subcutaneous injection at doses up to 20 mg/kg/day (male) or 40 mg/kg/day (female).
Mutagenesis
Apomorphine was mutagenic in the in vitro bacterial reverse mutation (Ames) and the in vitro mouse lymphoma tk assays. Apomorphine was clastogenic in the in vitro chromosomal aberration assay in human lymphocytes and in the in vitro mouse lymphoma tk assay. Apomorphine was negative in the in vivo micronucleus assay in mice.
Impairment of Fertility
Apomorphine was administered subcutaneously at doses up to 3 mg/kg/day to male and female rats prior to and throughout the mating period and continuing in females through gestation day 6. There was no evidence of adverse effects on fertility or on early fetal viability. A significant decrease in testis weight was observed in a 39-week study in cynomolgus monkey at all subcutaneous doses tested (0.3, 1, or 1.5 mg/kg/day).
In a published fertility study, apomorphine was administered to male rats at subcutaneous doses of 0.2, 0.8, or 2 mg/kg prior to and throughout the mating period. Fertility was reduced at the highest dose tested.
14. Clinical Studies
The efficacy of KYNMOBI for the acute, intermittent treatment of "off" episodes in patients with Parkinson's disease was established in one randomized, double-blind, placebo-controlled, parallel-group study (Study 1; NCT02469090).
The study enrolled patients with a mean duration of Parkinson's disease of approximately 9 years (range: 2 years to 22 years) who were Hoehn and Yahr Stage III or less in the "on" state, and who were all receiving concomitant levodopa with a stable dose for at least 4 weeks before screening. The most commonly used concomitant Parkinson's disease medications in addition to levodopa were oral dopaminergic agonists (51%), monoamine oxidase B inhibitors (41%), amantadine derivatives (21%), and other dopaminergic agents (8%).
At baseline, the mean number of daily "off" episodes was 4 and the mean duration of "off" episodes was slightly over an hour in both groups. The study included a titration phase and a 12-week maintenance phase. Patients were titrated to the dose that achieved a full "on" response and was tolerated during the titration phase. Patients were treated with an oral antiemetic starting 3 days before the titration phase. In the titration phase, patients (N=141) arrived at the study site in an "off" state having not taken their regular morning dose of carbidopa/levodopa or any other adjunctive PD medications, as well as having taken their last dose of carbidopa/levodopa and any other adjunctive PD medications no later than midnight the night before. Treatment was initiated in the clinic with a 10 mg dose of KYNMOBI. If the patient responded to treatment and tolerated the 10 mg KYNMOBI dose, the patient was randomized in a blinded fashion to KYNMOBI or placebo in a 1:1 ratio. If the patient tolerated the dose but did not adequately respond, the patient was asked to return to the clinic within 3 days and the dose was increased by 5 mg. The titration process was continued up to a maximum KYNMOBI dose of 35 mg or until a full "on" was achieved as determined by the investigator and the patient [see Dosage and Administration (2.2)]. Dose administration was permitted up to five times per day in the maintenance phase. The Movement Disorder Society-Unified Parkinson's Disease Rating Scale, Part III (MDS-UPDRS III) (motor examination) was measured pre dose, and at 15, 30, 45, 60, and 90 minutes post dose.
The primary endpoint of the study was the mean change from pre dose to 30 minutes post dose in the MDS-UPDRS III at the 12-week visit of the maintenance phase.
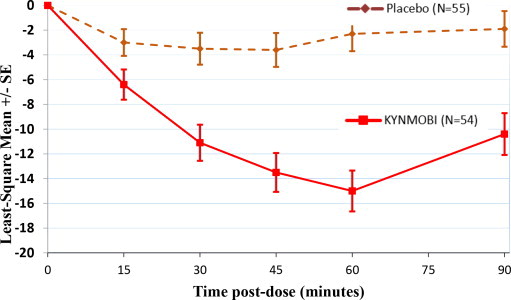
A total of 54 patients were randomized to KYNMOBI and 55 patients to placebo. The KYNMOBI treatment group showed a least-square mean improvement (i.e., reduction in score) of -11.1 points (95% CI: -14.0, -8.2), versus -3.5 points for the placebo group (95% CI: -6.1, -0.9). The least-square mean treatment difference between KYNMOBI and placebo was -7.6 (95% CI: -11.5, -3.7; p=0.0002) (Table 2).
Table 2. Change from Pre-dose to 30 Minutes Post-dose in the MDS-UPDRS III Score at Week 12 (Least-Square Mean) in Study 1:
| Treatment | Number of Patients at Week 12 | Observed Pre-dose MDS-UPDRS III Score at Week 12 | Least-Square Mean Change from Pre-dose to 30 Minutes Post-dose | Least-Square Mean Difference from placebo |
|---|---|---|---|---|
| Placebo | 46 | 42.2 | - 3.5 | N/A |
| KYNMOBI | 34 | 37.2 | - 11.1 | - 7.6 (p=0.0002) |
Figure 2 describes the least-square mean change from pre-dose in MDS-UPDRS Part III Motor Scores after administration of KYNMOBI versus placebo at week 12.
Figure 2. Estimated Least-Square Mean Change in MDS-UPDRS Part III Motor Score After Administration of KYNMOBI vs. Placebo (at Week 12) in Study 1:
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.