Source: Pharmaceutical Benefits Scheme (AU) Revision Year: 2022 Publisher: Dr. Reddys Laboratories (Australia) Pty Ltd, Suite 3.03, Level 3, 390 St Kilda Road, MELBOURNE, VIC, AUSTRALIA Phone: 1800 733 397
The precise mechanism of action by which levetiracetam induces seizure protection is unknown, but appears unrelated to the mechanisms of current antiepileptic drugs. In vitro and in vivo experiments suggest that levetiracetam does not alter basic cell characteristics and normal neurotransmission.
In vitro studies show that levetiracetam affects intraneuronal Ca2+ levels by partial inhibition of N type Ca2+ currents and by reducing the release of Ca2+ from intraneuronal stores. In addition, it partially reverses the reductions in GABA and glycine gated currents induced by zinc and betacarbolines. Furthermore, levetiracetam has been shown in in vitro studies to bind to a specific site in rodent brain tissue. This binding site is the synaptic vesicle protein 2A, believed to be involved in vesicle fusion and neurotransmitter exocytosis. Levetiracetam and related analogues show a rank order of affinity for binding to the synaptic vesicle protein 2A which correlates with the potency of their antiseizure protection in the mouse audiogenic model of epilepsy. This finding suggests that the interaction between levetiracetam and the synaptic vesicle protein 2A seems to contribute to the antiepileptic mechanism of action of the drug.
Levetiracetam is not active in the classical screening models for anticonvulsants, however it induces potent protection in a broad range of animal models of partial and primary generalised seizures, with an unusually high safety margin between therapeutic doses and doses inducing adverse effects.
Levetiracetam also displays potential antiepileptogenic properties by dose dependently inhibiting the development of kindling, even after discontinuation of the active substance. Withdrawal from chronic treatment did not decrease the seizure threshold. Anxiolytic action and an absence of undesirable effects on cognitive function have also been observed.
The major metabolite, ucb L057, is inactive in seizure models.
Both partial and generalised epilepsy models (epileptiform discharge/photoparoxysmal response) confirmed the broad spectrum preclinical pharmacological profile.
The monotherapy study was designed as a double blind, parallel group, noninferiority comparison of levetiractam and carbamazepine controlled release (CBZ CR) in patients 16 years of age or older with newly diagnosed epilepsy. The seizures were to be either unprovoked partial seizures (type IA (simple partial seizures with unimpaired consciousness), IB (complex partial seizures with impaired consciousness), IC (partial seizures secondarily generalised (with clear focal origin)) or IIE (generalised tonic clonic seizure (without clear focal origin)), classifiable according to the International Classification of Epileptic Seizures. The study was performed in 85 centers in 13 countries (Europe and South Africa).
At the end of the one week screening period, eligible subjects were stratified by seizure type (IA/IB/IC or IC/IIE without clear focal origin) and randomly assigned to receive CBZ CR (n=291) or levetiracetam (LEV) (n=285) for up to 121 weeks depending on response. Conservatively, a controlled release (CR) formulation of carbamazepine was used to minimise adverse effects. The maximal duration for an individual subject was 121 weeks.
After a one week screening period (no study drug intake), the subject was randomised and entered a two week up titration period to the first target daily dose (LEV 1,000 mg/ CBZ 400 mg), followed by a one week stabilisation period and an evaluation period of 26 weeks in order to achieve a six month seizure freedom (primary efficacy endpoint), and followed by a maintenance period of 26 additional weeks in order to assess safety and maintenance of efficacy.
If a seizure occurred during the evaluation period, dose escalation (made over a two week period) to the second target daily dose (LEV 2,000 mg/CBZ 800 mg) was foreseen. This was followed by a one week stabilisation period, a new evaluation period of 26 weeks and a maintenance period of 26 additional weeks. The same was true if a seizure occurred during the evaluation period at the second dose level: dose escalation (made over a two week period) to the third target daily dose (LEV 3,000 mg/ CBZ 1,200 mg), followed by a one week stabilisation period, a new evaluation period of 26 weeks and a maintenance period of 26 additional weeks. Fall back option: in case a subject did not tolerate the second or third study drug target dose, he/ she had the opportunity, during the evaluation or the maintenance period, to have one fall back to an intermediate dose (decrease by 200 mg/day for CBZ or by 500 mg/day for LEV) and to continue in the trial on that basis. The subject could not resume the previous dose and could not have further up titration in case a new seizure occurred.
576 subjects were randomised. Approximately one-half of the patients in each treatment group completed the study (53.6% of the patients randomised to CBZ and 54.0% of the patients randomised to LEV), similar between the two treatment groups. The distribution by seizure type categories was similar in both treatment groups, with around 86.7% of subjects lastly classified as experiencing partial seizures with clear focus origin. The majority of subjects remained at dose level 1 (81.7% of subjects randomised to CBZ and 73.4% of subjects randomised to LEV in the per protocol (PP) population).
The prospectively defined primary endpoint was the proportion of subjects from the PP population with six month seizure freedom at the last evaluated dose.
173 (73.0%) of the PP subjects in the LEV arm were seizure free for at least six months at the last evaluated dose, compared to 171 subjects (72.8%) in the CBZ arm. The adjusted absolute difference LEV and CBZ (95% two sided confidence interval (CI)) obtained from a logistic regression model including a factor for the seizure type category as last assessed (IA/IB/IC versus IC/IIE) equalled 0.2% (-7.8%; 8.2%). The lower limit of the CI (-7.8%) was above the noninferiority limit set by protocol (-15%) for this primary efficacy analysis and, therefore, LEV can be considered as noninferior to CBZ on the proportion of subjects seizure free at least six months at the first evaluated dose in the PP population. Considering the other clinically relevant endpoint, 56.6 and 58.5% of subjects on LEV and CBZ, respectively, were seizure free for one year.
The effectiveness of levetiracetam as adjunctive therapy (added to other antiepileptic drugs (AEDs)) in adults was established in three multicentre, randomised, double blind, placebo controlled clinical studies in patients who had refractory partial onset seizures with or without secondary generalisation. In these studies, 904 patients were randomised to placebo, 1,000, 2,000 or 3,000 mg/day. Patients enrolled in study 1 or study 2 had refractory partial onset seizures for at least two years and had taken two or more classical AEDs. Patients enrolled in study 3 had refractory partial onset seizures for at least one year and had taken one classical AED. At the time of the study, patients were taking a stable dose regimen of at least one and could take a maximum of two AEDs. During the baseline period, patients had to have experienced at least two partial onset seizures during each four week period.
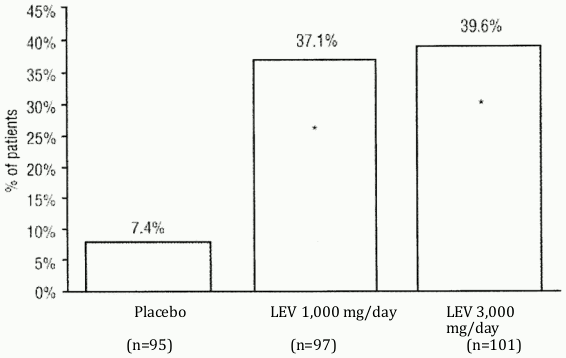
Study 1 was a double blind, placebo controlled, parallel group study conducted at 41 sites in the United States comparing levetiracetam 1,000 mg/day (n=97), levetiracetam 3,000 mg/day (n=101) and placebo (n=95) given in equally divided doses twice daily. After a prospective baseline period of 12 weeks, patients were randomised to one of the three treatment groups described above. The 18 week treatment period consisted of a six week titration period, followed by a 12 week fixed dose evaluation period, during which concomitant AED regimens were held constant. The primary measure of effectiveness was a between group comparison of the percent reduction in weekly partial seizure frequency relative to placebo over the entire randomised treatment period (titration plus evaluation period). Secondary outcome variables included the responder rate (incidence of patients with greater than or equal to 50% reduction from baseline in partial onset seizure frequency). The results of the analysis of study 1 are displayed in Table 7. Please refer to table 7.
Table 7. Reduction in weekly frequency of partial onset seizures in study 1:
| Placebo (n=95) | LEV 1,000 mg/day (n=97) | LEV 3,000 mg/day (n=101) | |
|---|---|---|---|
| Percent reduction in partial seizure frequency over placebo | 26.1% p<0.001 | 30.1% p<0.001 |
The percentage of patients (y-axis) who achieved greater than or equal to 50% reduction in weekly seizure rates from baseline in partial onset seizure frequency over the entire randomised treatment period (titration plus evaluation period) within the three treatment groups (x-axis) is presented in Figure 1. Please refer to figure 1.
Figure 1. Responder rate (≥50% reduction from baseline) in study 1:
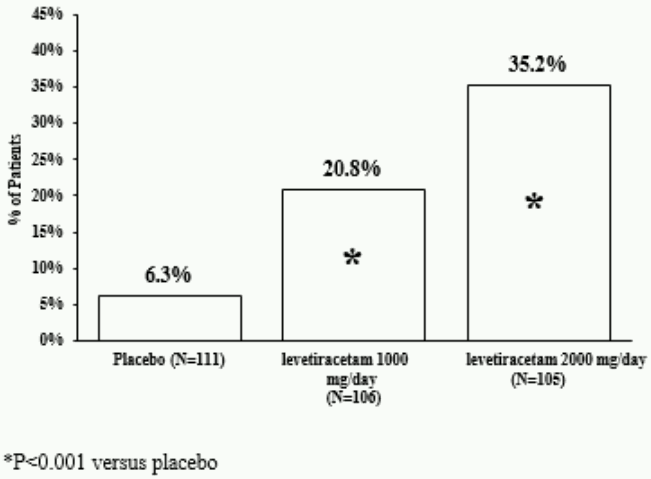
Study 2 was a double blind, placebo controlled, crossover study conducted at 62 centres in Europe comparing levetiracetam 1,000 mg/day (n = 106), levetiracetam 2,000 mg/day (n = 105) and placebo (n = 111) given in equally divided doses twice daily.
The first period of the study (period A) was designed to be analysed as a parallel group study. After a prospective baseline period of up to 12 weeks, patients were randomised to one of the three treatment groups described above. The 16 week treatment period consisted of the four week titration period followed by a 12 week fixed dose evaluation period, during which concomitant AED regimens were held constant. The primary measure of effectiveness was a between group comparison of the percent reduction in weekly partial seizure frequency relative to placebo over the entire randomised treatment period (titration plus evaluation period). Secondary outcome variables included the responder rate (incidence of patients with greater than or equal to 50% reduction from baseline in partial onset seizure frequency). The results of the analysis of period A are displayed in Table 8. Please refer to table 8.
Table 8. Reduction in weekly frequency of partial onset seizures in study 2 – period A:
| Placebo (n=111) | LEV 1,000 mg/day (n=106) | LEV 2,000 mg/day (n=105) | |
|---|---|---|---|
| Percent reduction in partial seizure frequency over placebo | 17.1% p<0.001 | 21.4% p<0.001 |
The percentage of patients (y-axis) who achieved greater than or equal to 50% reduction in weekly seizure rates from baseline in partial onset seizure frequency over the entire randomised treatment period (titration plus evaluation period) within the three treatment groups (x-axis) is presented in Figure 2. Please refer to figure 2.
Figure 2. Responder rate (≥50% reduction from baseline) in study 2 – period A:
The comparison of levetiracetam 2,000 mg/day to levetiracetam 1,000 mg/day for responder rate was statistically significant (p = 0.02). Analysis of the trial as a crossover yielded similar results.
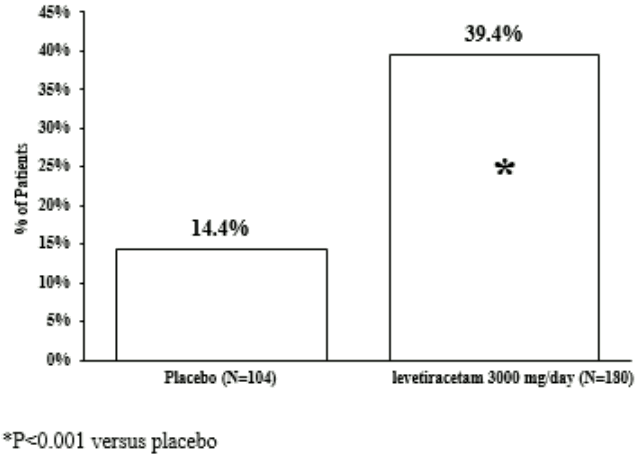
Study 3 was a double blind, placebo controlled, parallel group study conducted at 47 centres in Europe comparing levetiracetam 3,000 mg/day (n = 180) and placebo (n = 104) in patients with refractory partial onset seizures, with or without secondary generalisation, receiving only one concomitant AED. Study drug was given in two divided doses. After a prospective baseline period of 12 weeks, patients were randomised to one of two treatment groups described above. The 16 week treatment period consisted of a four week titration period, followed by a 12 week fixed dose evaluation period, during which concomitant AED doses were held constant. The primary measure of effectiveness was a between group comparison of the percent reduction in weekly seizure frequency relative to placebo over the entire randomised treatment period (titration plus evaluation period). Secondary outcome variables included the responder rate (incidence of patients with greater than or equal to 50% reduction from baseline in partial onset seizure frequency). Table 9 displays the results of the analysis of study 3. Please refer to table 9.
Table 9. Reduction in weekly frequency of partial onset seizures in study 3:
| Placebo (n=104) | LEV 3,000 mg/day (n=180) | |
|---|---|---|
| Percent reduction in partial seizure frequency over placebo | - | 23.0% p<0.001 |
Figure 3. Responder rate (≥50% reduction from baseline) in study 3:
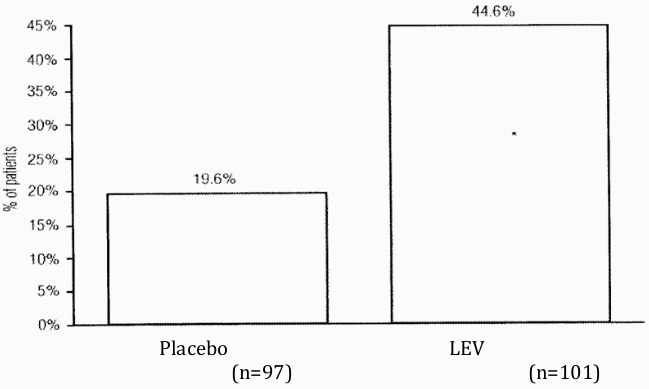
The effectiveness of levetiracetam as adjunctive therapy (added to other antiepileptic drugs) in paediatric patients was established in a multicentre, randomised double blind, placebo controlled study, conducted at 60 sites in North America, in children 4 to 16 years of age with partial seizures uncontrolled by standard AEDs. Eligible patients on a steady dose of one to two AEDs, who still experienced at least four partial onset seizures during the four weeks prior to screening, as well as at least four partial onset seizures in each of the two four week baseline periods, were randomised to receive either levetiracetam or placebo. The population included 198 patients (levetiracetam n = 101, placebo n = 97) with uncontrolled partial onset seizures, whether or not secondarily generalised. The study consisted of an eight week baseline period and four week titration period followed by a ten week evaluation period. Dosing was initiated at a target dose of 20 mg/kg/day in two divided doses. During the treatment period, levetiracetam doses were adjusted in 20 mg/kg/day increments, at two week intervals to the target dose of 60 mg/kg/day (or 40 mg/kg/day as a maximum tolerated dose).
The primary measure of effectiveness was a between group comparison of the percent reduction in weekly partial seizure frequency relative to placebo over the entire randomised treatment period (titration plus evaluation period). Secondary outcome variables included the responder rate (incidence of patients with greater than or equal to 50% reduction from baseline in partial onset seizure frequency per week). Table 4 displays the results of this study. Please refer to table 4.
Table 10. Reduction in weekly frequency of partial onset seizures:
| Placebo (n=97) | LEV (n=101) | |
|---|---|---|
| Percent reduction in partial seizure frequency over placebo | --- | 26.8%* |
* p=0.0002
The percentage of patients (y-axis) who achieved greater than or equal to 50% reduction in weekly seizure rates from baseline in partial onset seizure frequency over the entire randomised treatment period (titration plus evaluation period) within the two treatment groups (x-axis) is presented in Figure 4. Please refer to figure 4.
Figure 4. Responder rate (≥50% reduction from baseline):
The effectiveness of levetiracetam as adjunctive therapy in patients 12 years of age and older with juvenile myoclonic epilepsy experiencing myoclonic seizures was established in one multicentre, randomised, double blind, placebo controlled study conducted at 37 sites in 14 countries. Eligible patients on a stable dose of one AED experiencing one or more myoclonic seizures/day for at least eight days during the prospective eight week baseline period were randomised to either levetiracetam or placebo. The population included 120 patients (levetiracetam n=60, placebo n=60) with idiopathic generalised epilepsy which included juvenile myoclonic epilepsy, juvenile absence epilepsy or epilepsy with generalised tonic clonic seizures on awakening. The majority were patients with juvenile myoclonic epilepsy. Patients were titrated over four weeks to a target dose of 3,000 mg/day and treated at a stable dose of 3,000 mg/day over 12 weeks (evaluation period). Study drug was given in two divided doses.
The primary measure of effectiveness was the proportion of patients with at least 50% reduction in the number of days/week with one or more myoclonic seizures during the treatment period (titration + evaluation periods) as compared to baseline. Secondary outcome variables included seizure frequency/week over the treatment period. Table 5 displays the results of this study. Please refer to table 5.
Table 11. Responder rate (≥ 50% reduction from baseline) in myoclonic seizure days per week for patients with JME:
| Placebo (n=60) | LEV (n=60) | |
|---|---|---|
| Percentage of responders | 23.3% | 58.3%* |
^* P=0.0002
The effectiveness of levetiracetam as adjunctive therapy (added to other AEDs) in patients 4 years of age and older with idiopathic generalised epilepsy experiencing primary generalised tonic clonic (PGTC) seizures was established in one multicentre, randomised, double blind, placebo controlled study conducted at 50 sites in eight countries. Eligible patients on a stable dose of one or two AEDs experiencing at least three PGTC seizures during the eight week combined baseline period (at least one PGTC seizure during the four weeks prior to the prospective baseline period and at least one PGTC seizure during the four week prospective baseline period) were randomised to either levetiracetam or placebo. The eight week combined baseline period is referred to as ‘baseline’ in the remainder of this section. The population included 164 patients (levetiracetam n = 80, placebo n = 84) with idiopathic generalised epilepsy (predominately juvenile myoclonic epilepsy, juvenile absence epilepsy, childhood absence epilepsy or epilepsy with grand mal seizures on awakening) experiencing primary generalised tonic clonic seizures. Each of these syndromes of idiopathic generalised epilepsy was well represented in this patient population. Patients were titrated over four weeks to a target dose of 3,000 mg/day for adults or a pediatric target dose of 60 mg/kg/day and treated at a stable dose of 3,000 mg/day (or 60 mg/kg/day for children) over 20 weeks (evaluation period). Study drug was given in two equally divided doses/day.
The primary measure of effectiveness was the percent reduction from baseline in weekly PGTC seizure frequency for levetiracetam and placebo treatment groups over the treatment period (titration + evaluation periods). There was a statistically significant decrease from baseline in PGTC frequency in the levetiracetam treated patients compared to the placebo treated patients. (See Table 6.)
Table 12. Median % reduction from baseline in PGTC seizure frequency per week:
| Placebo (n=84) | LEV (n=78) | |
|---|---|---|
| Percent reduction in PGTC seizure frequency | 44.6% | 77.6%* |
* statistically significant versus placebo
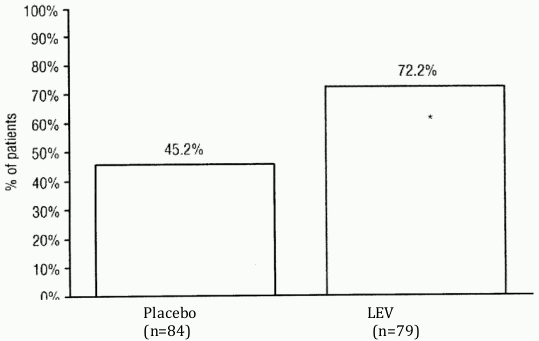
The percentage of patients (y-axis) who achieved greater than or equal to 50% reduction in weekly seizure rates from baseline in PGTC seizure frequency over the entire randomised treatment period (titration + evaluation period) within the two treatment groups (x-axis) is presented in Figure 5.
Figure 5. Responder rate (≥ 50% reduction from baseline) in PGTC seizure frequency per week:
* statistically significant versus placebo
When levetiracetam was used to treat PGTC seizures in adults and adolescents with idiopathic generalised epilepsy, there was no effect on the frequency of absences.
Levetiracetam is a highly soluble and permeable compound. The pharmacokinetic profile is linear and time independent with low intrasubject and intersubject variability. There is no modification of the clearance after repeated administration. There is no evidence for any relevant gender, race or circadian variability. The pharmacokinetic profile is comparable in healthy volunteers and in patients with epilepsy.
Due to its complete and linear absorption, plasma levels can be predicted from the oral dose of levetiracetam expressed as mg/kg bodyweight. Therefore, there is no need for plasma level monitoring of levetiracetam.
A significant correlation between saliva and plasma concentrations has been shown in adults and children (ratio of saliva/ plasma concentrations ranged from 1 to 1.7 for oral tablet formulation and after four hours postdose for oral solution formulation).
A single dose of levetiracetam 1,500 mg diluted in 100 mL of a compatible diluent and infused intravenously over 15 minutes is bioequivalent to levetiracetam 1,500 mg oral intake, given as three 500 mg tablets.
The intravenous administration of doses up to 4,000 mg diluted in sodium chloride 0.9% 100 mL infused over 15 minutes and doses up to 2,500 mg diluted in sodium chloride 0.9% 100 mL infused over five minutes was evaluated. The pharmacokinetic and safety profiles did not identify any safety concerns.
Levetiracetam is rapidly absorbed after oral administration. Oral absolute bioavailability is close to 100%. Peak plasma concentrations (Cmax) are achieved at 1.3 hours after dosing. Steady state is achieved after two days of a twice daily administration schedule. Peak concentrations (Cmax) are typically 31 and 43 microgram/mL following a single 1,000 mg dose and repeated 1,000 mg twice daily (bid) dose, respectively. The extent of absorption is doseindependent and is not altered by food but the rate of absorption is slightly reduced.
No tissue distribution data are available in humans. Neither levetiracetam nor its major metabolite (ucb L057) are significantly bound to plasma proteins (<10%). The volume of distribution of levetiracetam is approximately 0.5 to 0.7 L/kg, a value close to the volume of distribution of intracellular and extracellular water.
The major metabolic pathway (24% of the dose) is an enzymatic hydrolysis of the acetamide group. Production of this metabolite, ucb L057, is not supported by liver cytochrome P450 isoforms. Hydrolysis of the acetamide group was measurable in a large number of tissues including whole blood but not plasma. The metabolite ucb L057 is pharmacologically inactive.
Two minor metabolites were also identified. One was obtained by hydroxylation of the pyrrolidone ring (1.6% of the dose) and the other one by opening of the pyrrolidone ring (0.9% of the dose).
Other unidentified components accounted for only 0.6% of the dose.
No enantiomeric interconversion was evidenced in vivo for either levetiracetam or its major metabolite ucb L057.
In vitro, levetiracetam and its primary metabolite have been shown not to inhibit the major human liver cytochrome P450 isoforms (CYP3A4, 2A6, 2C9, 2C19, 2D6, 2E1, 1A2) glucuronyl transferase (UGT1A1 and UGT1A6) AND EPOXIDE HYDROXYLASE ACTIVITIES. In addition, levetiracetam does not affect the in vitro glucuronidation of valproic acid.
In human hepatocytes in vitro, levetiracetam had no effect on CYP1A/2 or UGT isoform activities (including ethinyloestradiol conjugation). Levetiracetam caused mild induction of CYP2B6 and CYP3A4, but only at high concentrations not considered to be clinically relevant. Therefore, the interaction of levetiracetam with other substances, or vice versa, is unlikely.
The plasma half-life in adults was 7.2 +/- 1.1 hours and did not vary either with dose, route of administration or repeated administration. The total body clearance was a mean of 0.96 +/- 0.14 mL/minute/kg.
The major route of excretion was via urine, accounting for a mean 95% of the dose, with approximately 93% of the dose excreted within 48 hours. Excretion via faeces accounted for only 0.3% of the dose. The cumulative urinary excretion of levetiracetam and its major metabolite (ucb L057) accounted for 66 and 24% of the dose, respectively, during the first 48 hours. The renal clearance of levetiracetam is 0.6 mL/minute/kg, indicating that it is excreted by glomerular filtration with subsequent tubular reabsorption. The renal clearance of the major metabolite, ucb L057, is 4.2 mL/minute/kg indicating active tubular secretion in addition to glomerular filtration.
In elderly patients, the half-life is increased by about 40% (ten to eleven hours) and is attributed to the decrease in renal function in this population (see 4.2 Dose and method of administration).
Following single dose administration (20 mg/kg) to epileptic children (6 to 12 years of age), the half-life of levetiracetam was 6.0 +/- 1.1 hours. The apparent body clearance was approximately 30% higher than in epileptic adults.
Following repeated oral dose administration (20 to 60 mg/kg/day) to epileptic children (4 to 12 years of age), levetiracetam was rapidly absorbed. Peak plasma concentration was observed 0.5 to 1.0 hour after dosing. Linear and dose proportional increases were observed for peak plasma concentrations and area under the curve. The elimination half-life was approximately five hours. The apparent body clearance was 1.1 mL/minute/kg.
Following single dose administration (20 mg/kg) of a 10% oral solution to epileptic children (1 month to 4 years of age), levetiracetam was rapidly absorbed and peak plasma concentrations were observed approximately one hour after dosing. The pharmacokinetic results indicated that half-life was shorter (5.3 hours) than for adults (7.2 hours) and apparent clearance was faster (1.5 mL/minute/kg) than for adults (0.96 mL/minute/kg).
The apparent body clearance of both levetiracetam and its major metabolite (ucb L057) is correlated to the creatinine clearance. It is, therefore, recommended to adjust the maintenance daily dose of levetiracetam, based on creatinine clearance in patients with moderate and severe renal impairment (see 4.2 Dose and method of administration).
In anuric endstage renal disease adult subjects the half-life was approximately 25 and 3.1 hours during interdialytic and intradialytic periods, respectively. The fractional removal of levetiracetam was 51% during a typical four hour dialysis session.
In subjects with mild and moderate hepatic impairment, there was no relevant modification of the clearance of levetiracetam. In most subjects with severe hepatic impairment, the clearance of levetiracetam was reduced by more than 50% due to concomitant renal impairment (see 4.2 Dose and method of administration).
Levetiracetam was negative in gene mutation assays (bacterial, Chinese hamster ovary/HGPRT locus) and in assays for chromosomal damage in vitro and in vivo (Chinese hamster ovary cells, mouse micronucleus assay). The hydrolysis product and major human metabolite (ucb L057) was not mutagenic in bacterial reverse mutation assays or the in vitro mouse lymphoma assay.
There was no evidence of carcinogenicity following administration of levetiracetam in the diet to rats or orally to mice for 104 weeks, associated with respective systemic exposures (plasma AUC) up to fourfold and eightfold that in humans at the maximal recommended clinical dose of 3,000 mg/day.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.