Source: European Medicines Agency (EU) Revision Year: 2019 Publisher: Daiichi Sankyo Europe GmbH, Zielstattstrasse 48, 81379 Munich, Germany
Prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation (NVAF) with one or more risk factors, such as congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke or transient ischaemic attack (TIA).
Treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recurrent DVT and PE in adults (see section 4.4 for haemodynamically unstable PE patients).
The recommended dose is 60 mg edoxaban once daily.
Therapy with edoxaban in NVAF patients should be continued long term.
The recommended dose is 60 mg edoxaban once daily following initial use of parenteral anticoagulant for at least 5 days (see section 5.1). Edoxaban and initial parenteral anticoagulant should not be administered simultaneously.
The duration of therapy for treatment of DVT and PE (venous thromboembolism, VTE), and prevention of recurrent VTE should be individualised after careful assessment of the treatment benefit against the risk for bleeding (see section 4.4). Short duration of therapy (at least 3 months) should be based on transient risk factors (e.g. recent surgery, trauma, immobilisation) and longer durations should be based on permanent risk factors or idiopathic DVT or PE.
For NVAF and VTE the recommended dose is 30 mg edoxaban once daily in patients with one or more of the following clinical factors:
Table 1. Summary of posology in NVAF and VTE (DVT and PE):
| Summary guide for dosing | ||
|---|---|---|
| Recommended dose | 60 mg edoxaban once daily | |
| Dose recommendation for patients with one or more of the following clinical factors: | ||
| Renal impairment | Moderate or severe (CrCL 15–50 mL/min) | 30 mg edoxaban once daily |
| Low body weight | ≤60 kg | |
| P-gp inhibitors | Ciclosporin, dronedarone, erythromycin, ketoconazole | |
If a dose of Lixiana is missed, the dose should be taken immediately and then be continued the following day with the once-daily intake as recommended. The patient should not take double the prescribed dose on the same day to make up for a missed dose.
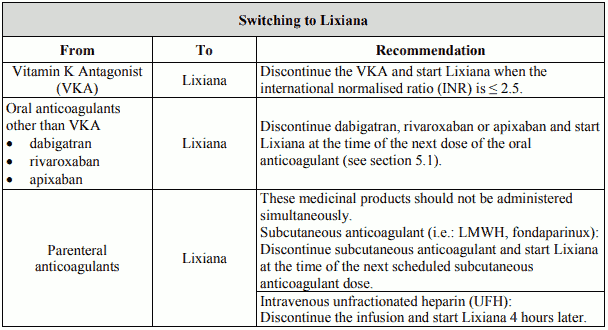
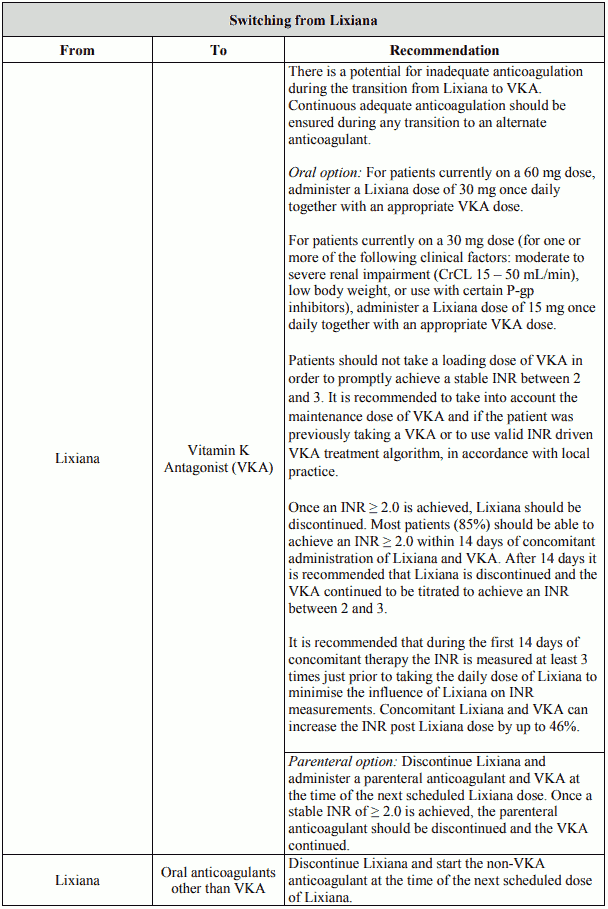
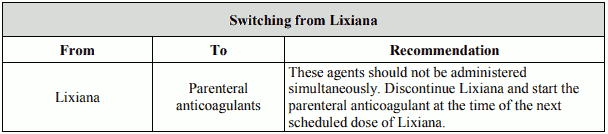
Continued anticoagulant therapy is important in patients with NVAF and VTE. There may be situations that warrant a change in anticoagulation therapy (Table 2).
Table 2. Switching:
The method used to estimate renal function (CrCL in mL/min) during the clinical development of Lixiana was the Cockcroft-Gault method. The formula is as follows:
This method is recommended when assessing patients' CrCL prior to and during Lixiana treatment.
In patients with mild renal impairment (CrCL >50-80 mL/min), the recommended dose is 60 mg Lixiana once daily.
In patients with moderate or severe renal impairment (CrCL 15-50 mL/min), the recommended dose is 30 mg Lixiana once daily (see section 5.2).
In patients with end stage renal disease (ESRD) (CrCL <15 mL/min) or on dialysis, the use of Lixiana is not recommended (see sections 4.4 and 5.2).
Lixiana is contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk (see section 4.3).
In patients with severe hepatic impairment Lixiana is not recommended (see sections 4.4 and 5.2).
In patients with mild to moderate hepatic impairment the recommended dose is 60 mg Lixiana once daily (see section 5.2). Lixiana should be used with caution in patients with mild to moderate hepatic impairment (see section 4.4).
Patients with elevated liver enzymes (ALT/AST >2 x ULN) or total bilirubin ≥1.5 x ULN were excluded in clinical trials. Therefore Lixiana should be used with caution in this population (see sections 4.4 and 5.2). Prior to initiating Lixiana, liver function testing should be performed.
For patients with body weight ≤60 kg, the recommended dose is 30 mg Lixiana once daily (see section 5.2).
No dose reduction is required (see section 5.2).
No dose reduction is required (see section 5.2).
In patients concomitantly taking Lixiana and the following P-gp inhibitors: ciclosporin, dronedarone, erythromycin, or ketoconazole, the recommended dose is 30 mg Lixiana once daily (see section 4.5). No dose reduction is required for concomitant use of amiodarone, quinidine or verapamil (see section 4.5).
The use of Lixiana with other P-gp inhibitors including HIV protease inhibitors has not been studied.
The safety and efficacy of Lixiana in children and adolescents less than 18 years of age have not been established. No data are available.
Lixiana can be initiated or continued in patients who may require cardioversion. For transoesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, Lixiana treatment should be started at least 2 hours before cardioversion to ensure adequate anticoagulation (see sections 5.1 and 5.2). Cardioversion should be performed no later than 12 hours after the dose of Lixiana on the day of the procedure.
For all patients undergoing cardioversion: Confirmation should be sought prior to cardioversion that the patient has taken Lixiana as prescribed. Decisions on initiation and duration of treatment should follow established guidelines for anticoagulant treatment in patients undergoing cardioversion.
For oral use.
Lixiana can be taken with or without food (see section 5.2).
Overdose with edoxaban may lead to haemorrhage. Experience with overdose cases is very limited.
A specific antidote antagonising the pharmacodynamic effect of edoxaban is not available.
Early administration of activated charcoal may be considered in case of edoxaban overdose to reduce absorption. This recommendation is based on standard treatment of drug overdose and data available with similar compounds, as the use of activated charcoal to reduce absorption of edoxaban has not been specifically studied in the edoxaban clinical programme.
Should a bleeding complication arise in a patient receiving edoxaban, the next edoxaban administration should be delayed or treatment should be discontinued as appropriate. Edoxaban has a half-life of approximately 10 to 14 hours (see section 5.2). Management should be individualised according to the severity and location of the haemorrhage. Appropriate symptomatic treatment could be used as needed, such as mechanical compression (e.g. for severe epistaxis), surgical haemostasis with bleeding control procedures, fluid replacement and haemodynamic support, blood products (packed red cells or fresh frozen plasma, depending on associated anaemia or coagulopathy) or platelets.
For life-threatening bleeding that cannot be controlled with the measures such as transfusion or haemostasis, the administration of a 4-factor prothrombin complex concentrate (PCC) at 50 IU/kg has been shown to reverse the effects of Lixiana 30 minutes after completing the infusion.
Recombinant factor VIIa (r-FVIIa) can also be considered. However, there is limited clinical experience with the use of this product in individuals receiving edoxaban.
Depending on local availability, a consultation with a coagulation expert should be considered in case of major bleedings.
Protamine sulfate and vitamin K are not expected to affect the anticoagulant activity of edoxaban.
There is no experience with antifibrinolytic agents (tranexamic acid, aminocaproic acid) in individuals receiving edoxaban. There is neither scientific rationale for benefit nor experience with the use of systemic haemostatics (desmopressin, aprotinin) in individuals receiving edoxaban. Due to the high plasma protein binding edoxaban is not expected to be dialysable.
5 years.
This medicinal product does not require any special storage conditions.
15 mg film-coated tablets: PVC/Aluminium blisters. Cartons of 10 film-coated tablets. PVC/Aluminium perforated unit dose blisters of 10 × 1 film-coated tablets.
30 mg and 60 mg film-coated tablets: PVC/Aluminium blisters. Cartons of 10, 14, 28, 30, 56, 60, 84, 90, 98, 100 film-coated tablets. PVC/Aluminium perforated unit dose blisters of 10 × 1, 50 × 1 and 100 × 1 film-coated tablets.
Not all pack sizes may be marketed.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.