LOTRONEX Tablet Ref.[9948] Active ingredients: Alosetron
Source: FDA, National Drug Code (US) Revision Year: 2019
12.1. Mechanism of Action
Alosetron is a potent and selective 5-HT3 receptor antagonist. 5-HT3 receptors are ligand-gated cation channels that are extensively distributed on enteric neurons in the human gastrointestinal tract, as well as other peripheral and central locations. Activation of these channels and the resulting neuronal depolarization affect the regulation of visceral pain, colonic transit, and gastrointestinal secretions, processes that relate to the pathophysiology of IBS. 5-HT3 receptor antagonists such as alosetron inhibit activation of non-selective cation channels, which results in the modulation of the enteric nervous system.
The cause of IBS is unknown. IBS is characterized by visceral hypersensitivity and hyperactivity of the gastrointestinal tract, which lead to abnormal sensations of pain and motor activity. Following distention of the rectum, patients with IBS exhibit pain and discomfort at lower volumes than healthy volunteers. Following such distention, alosetron reduced pain and exaggerated motor responses, possibly due to blockade of 5-HT3 receptors.
12.2. Pharmacodynamics
In healthy volunteers and patients with IBS, alosetron (2 mg orally, twice daily for 8 days) increased colonic transit time without affecting orocecal transit time. In healthy volunteers, alosetron also increased basal jejunal water and sodium absorption after a single 4 mg dose. In patients with IBS, multiple oral dosages of alosetron (4 mg twice daily for 6.5 days) significantly increased colonic compliance.
Single oral doses of alosetron administered to healthy men produced a dose-dependent reduction in the flare response seen after intradermal injection of serotonin. Urinary 6-β-hydroxycortisol excretion decreased by 52% in elderly subjects after 27.5 days of alosetron 2 mg administered orally twice daily. This decrease was not statistically significant. In another study utilizing alosetron 1 mg administered orally twice daily for 4 days, there was a significant decrease in urinary 6-β-hydroxycortisol excretion. However, there was no change in the ratio of 6-β-hydroxycortisol to cortisol, indicating a possible decrease in cortisol production. The clinical significance of these findings is unknown.
12.3. Pharmacokinetics
The pharmacokinetics of alosetron have been studied after single oral doses ranging from 0.05 to 16 mg in healthy men. The pharmacokinetics of alosetron have also been evaluated in healthy women and men and in patients with IBS after repeated oral dosages ranging from 1 mg twice daily to 8 mg twice daily.
Absorption
Alosetron was rapidly absorbed after oral administration with a mean absolute bioavailability of approximately 50% to 60% (approximate range, 30% to >90%). After administration of radiolabeled alosetron, only 1% of the dose was recovered in the feces as unchanged drug. Following oral administration of a 1 mg alosetron dose to young men, a peak plasma concentration of approximately 5 ng/mL occurred at 1 hour. In young women, the mean peak plasma concentration was approximately 9 ng/mL, with a similar time to peak.
Plasma concentrations were 30% to 50% lower and less variable in men compared to women given the same oral dose. Population pharmacokinetic analysis in IBS patients confirmed that alosetron concentrations were influenced by gender (27% lower in men).
Food Effects: Alosetron absorption is decreased by approximately 25% by co-administration with food, with a mean delay in time to peak concentration of 15 minutes [see Dosage and Administration (2.1)].
Distribution
Alosetron demonstrates a volume of distribution of approximately 65 to 95 L. Plasma protein binding is 82% over a concentration range of 20 to 4,000 ng/mL.
Metabolism and Elimination
Plasma concentrations of alosetron increase proportionately with increasing single oral doses up to 8 mg and more than proportionately at a single oral dose of 16 mg. Twice-daily oral dosing of alosetron does not result in accumulation. The terminal elimination half-life of alosetron is approximately 1.5 hours (plasma clearance is approximately 600 mL/min). Population pharmacokinetic analysis in patients with IBS confirmed that alosetron clearance is minimally influenced by doses up to 8 mg.
Renal elimination of unchanged alosetron accounts for only 13% of the dose. Renal clearance is approximately 112 mL/min.
A study with 14C-labeled alosetron in Caucasian males (n = 3) and females (n = 3) and an Asian male (n = 1) showed similar serum metabolite profiles. Unchanged alosetron was the major component in serum, with other metabolites being present at low concentrations, none amounting to more than 15% of the unmetabolized alosetron concentration. The circulating metabolites were identified as 6-hydroxy glucuronide, 6-hydroxy sulphate, 7-hydroxy sulphate, hydroxymethyl imidazole, and mono- and bis-oxygenated imidazole derivatives of alosetron. The metabolites are unlikely to contribute to the biological activity of alosetron. Of the circulating Phase I metabolites, only the hydroxymethyl imidazole has weak pharmacological activity, around 10-fold less potent than alosetron. Total recovery of radioactivity in the excreta was 85 ± 6%. The majority of the radiolabeled dose is excreted in the urine (74 ± 5%). The major urinary metabolites were the 6-hydroxy glucuronide and the mono- and bis-oxygenated imidazole derivatives of alosetron. 11 ± 4% of the radiolabeled dose was excreted in the feces with less than 1% of the dose being excreted as the unchanged alosetron.
Alosetron is metabolized by human microsomal cytochrome P450 (CYP), shown in vitro to involve enzymes 2C9 (30%), 3A4 (18%), and 1A2 (10%). Non-CYP-mediated Phase I metabolic conversion also contributes to an extent of about 11%. However, in vivo data suggest that CYP1A2 plays a more prominent role in alosetron metabolism (62 to 97% of alosetron clearance) based on correlation of alosetron clearance with in vivo CYP1A2 activity measured by probe substrate, increased clearance induced by smoking, and inhibition of clearance by fluvoxamine [see Contraindications (4), Drug Interactions (7)].
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
In 2-year oral studies, alosetron was not carcinogenic in mice at doses up to 30 mg/kg/day or in rats at doses up to 40 mg/kg/day. These doses are about 60 to 160 times, respectively, the recommended human dose of alosetron of 2 mg/day (1 mg twice daily) based on body surface area. Alosetron was not genotoxic in the Ames tests, the mouse lymphoma cell (L5178Y/TK±) forward gene mutation test, the human lymphocyte chromosome aberration test, the ex vivo rat hepatocyte unscheduled DNA synthesis (UDS) test, or the in vivo rat micronucleus test for mutagenicity. Alosetron at oral doses up to 40 mg/kg/day (about 160 times the recommended daily human dose based on body surface area) was found to have no effect on fertility and reproductive performance of male or female rats.
14. Clinical Studies
14.1 Dose-Ranging Study
Data from a dose-ranging study of women (n = 85) who received LOTRONEX 0.5 mg twice daily indicated that the incidence of constipation (14%) was lower than that experienced by women receiving 1 mg twice daily (29%). Therefore, to lower the risk of constipation, LOTRONEX should be started at a dosage of 0.5 mg twice a day. The efficacy of the 0.5 mg twice-daily dosage in treating severe diarrhea-predominant IBS has not been adequately evaluated in clinical trials [See Dosage and Administration (2.1)].
14.2 Efficacy Studies
LOTRONEX has been studied in women with IBS in five 12-week US multicenter, randomized, double-blind, placebo-controlled clinical studies.
Table 3. Efficacy Studies Conducted in Women With Irritable Bowel Syndrome (IBS):
| Study | Patient Population | Placebo(n) | Lotronex Dose (n) |
|---|---|---|---|
| 1 and 2 | Non-constipated women with IBS | (640) | 1 mg twice daily (633) |
| 3 and 4 | Women with severe diarrhea-predominantIBS (defined as bowel urgency ≥50% of days) | (515) | 1 mg twice daily (778) |
| 5 | Women with severe diarrhea-predominant IBS (defined as average pain ≥moderate,urgency ≥50% of days, and/or restriction ofdaily activities ≥25% of days) | (176) | 0.5 mg once daily (177) |
| 1 mg once daily (175) | |||
| 1 mg once daily (177) |
Studies in Non-Constipated Women with Irritable Bowel Syndrome: Studies 1 and 2 were conducted in non-constipated women with IBS meeting the Rome Criteria1 for at least 6 months. Women with severe pain or a history of severe constipation were excluded. A 2-week run-in period established baseline IBS symptoms.
About two thirds of the women had diarrhea-predominant IBS. Compared with placebo, 10% to 19% more women with diarrhea-predominant IBS who received LOTRONEX had adequate relief of IBS abdominal pain and discomfort during each month of the study.
Studies in Women With Severe Diarrhea-Predominant Irritable Bowel Syndrome: LOTRONEX is indicated only for women with severe diarrhea-predominant IBS [see Indications and Usage (1)]. The efficacy of LOTRONEX in this subset of the women studied in clinical trials is supported by prospective and retrospective analyses.
Prospective Analyses: Studies 3 and 4 were conducted in women with diarrhea-predominant IBS and bowel urgency on at least 50% of days at entry. Women receiving LOTRONEX had significant increases over placebo (13% to 16%) in the median percentage of days with urgency control.
The lower gastrointestinal functions of stool consistency, stool frequency, and sense of incomplete evacuation were also evaluated by patients' daily reports. Stool consistency was evaluated on a scale of 1 to 5 (1 = very hard, 2 = hard, 3 = formed, 4 = loose, and 5 = watery). At baseline, average stool consistency was approximately 4 (loose) for both treatment groups. During the 12 weeks of treatment, the average stool consistency decreased to approximately 3.0 (formed) for patients who received LOTRONEX and 3.5 for the patients who received placebo in the 2 studies.
At baseline, average stool frequency was approximately 3.2 per day for both treatment groups. During the 12 weeks of treatment, the average daily stool frequency decreased to approximately 2.1 and 2.2 for patients receiving LOTRONEX and 2.7 and 2.8 for patients receiving placebo in the 2 studies.
There was no consistent effect upon the sense of incomplete evacuation during the 12 weeks of treatment for patients receiving LOTRONEX as compared to patients receiving placebo in either study.
Study 5 was conducted in women with severe diarrhea-predominant IBS and 1 or more of the following: frequent and severe abdominal pain or discomfort, frequent bowel urgency or fecal incontinence, disability or restriction of daily activities due to IBS. To evaluate the proportion of patients who responded to treatment, patients were asked every 4 weeks to compare their IBS symptoms during the previous month of treatment with how they usually felt during the 3 months prior to the study using an ordered 7-point scale (substantially worse to substantially improved). A responder was defined as a subject who reported moderate or substantial improvement on this global improvement scale (GIS). At Week 12, all three groups receiving LOTRONEX had significantly greater percentages of GIS responders compared to the placebo group (43% to 51% vs. 31%) using a Last Observation Carried Forward (LOCF) analysis. It should be noted that approximately 4% of subjects in each LOTRONEX dose group who were classified as responders using this approach were observed only through week 4. At each of the 4 week intervals of the treatment phase, all three dosages of LOTRONEX provided improvement in the average adequate relief rate of IBS pain and discomfort, stool consistency, stool frequency, and sense of urgency compared with placebo.
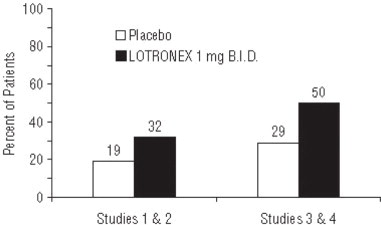
Retrospective Analyses: In analyses of patients from Studies 1 and 2 who had diarrhea-predominant IBS and indicated their baseline run-in IBS symptoms were severe at the start of the trial, LOTRONEX provided greater adequate relief of IBS pain and discomfort than placebo. In further analyses of Studies 1 and 2, 57% of patients had urgency at baseline on 5 or more days per week. In this subset, 32% of patients on LOTRONEX had urgency no more than 1 day in the last week of the trial, compared with 19% of patients on placebo.
In Studies 3 and 4, 66% of patients had urgency at baseline on 5 or more days per week. In this subset, 50% of patients on LOTRONEX had urgency no more than 1 day in the last week of the trial, compared with 29% of patients on placebo. Moreover, in the same subset, 12% on LOTRONEX had urgency no more than 2 days per week in any of the 12 weeks on treatment compared with 1% of placebo patients.
In Studies 1 and 2, patient-reported subjective outcomes related to IBS were assessed by questionnaires obtained at baseline and week 12. Patients in the more severe subset who received LOTRONEX reported less difficulty sleeping, less tiredness, fewer eating problems, and less interference with social activities and work/main activities due to IBS symptoms or problems compared to those who received placebo. Change in the impact of IBS symptoms and problems on emotional and mental distress and on physical and sexual activity in women who received LOTRONEX were not statistically different from those reported by women who received placebo.
14.3 Long-Term Use
In a 48-week multinational, double-blind, placebo-controlled study, LOTRONEX 1 mg twice daily was evaluated in 714 women with non-constipated IBS. A retrospective analysis of the subset of women with severe diarrhea-predominant IBS (urgency on at least 10 days during the 2-week baseline period) was performed. Of the 417 patients with severe diarrhea-predominant IBS, 62% completed the trial.
LOTRONEX (n = 198) provided a greater average rate of adequate relief of IBS pain and discomfort (52% vs. 41%) and a greater average rate of satisfactory control of bowel urgency (60% vs. 48%) compared with placebo (n = 219). Significant improvement of these symptoms occurred for most of the 48-week treatment period with no evidence of tachyphylaxis.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.