LUMVOA Solution for injection Ref.[116700] Active ingredients: Veligrotug
Source: FDA, National Drug Code (US) Revision Year: 2026
12.1. Mechanism of Action
Veligrotug-vvze's mechanism of action in patients with thyroid eye disease has not been fully characterized. Veligrotug-vvze is a humanized IgG1 monoclonal antibody that binds to IGF-1R and inhibits IGF-1R signaling by blocking ligand-induced receptor autophosphorylation.
12.2. Pharmacodynamics
No formal pharmacodynamic studies have been conducted with veligrotug-vvze.
12.3. Pharmacokinetics
The pharmacokinetics (PK) of veligrotug-vvze were described by a two-compartment population PK model based on data from 298 patients with thyroid eye disease receiving 10 mg/kg LUMVOA every 3 weeks in 4 clinical trials. Following this dose regimen, the geometric mean estimates for steady-state area under the concentration curve (AUC), peak (Cmax), and trough (Ctrough) concentrations of veligrotug-vvze were 3450 mcg∙day/mL, 363 mcg/mL, and 97.8 mcg/mL, respectively.
Distribution
The population PK estimated mean central and peripheral volume of distribution of veligrotug-vvze were 2.80 L and 2.50 L, respectively.
Elimination
The population PK estimated mean (% relative standard error) linear clearance of veligrotug-vvze was 0.216 (2.7) L/day with a corresponding half-life of approximately 18 days.
Metabolism
Metabolism of veligrotug-vvze has not been fully characterized. However, veligrotug-vvze is expected to undergo metabolism via proteolysis.
Specific Populations
No clinically meaningful differences in the pharmacokinetics of veligrotug-vvze were observed following administration of LUMVOA based on patient's age (20-79 years), sex (216 female and 82 male), race/ethnicity (224 White, 22 Black, and 13 Asian), or weight (41-161 kg). Neither renal nor hepatic impairment is expected to influence the pharmacokinetics of veligrotug-vvze.
Drug Interaction Studies
No studies evaluating the drug interaction potential of LUMVOA have been conducted.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
The carcinogenic potential of LUMVOA has not been evaluated in long-term animal studies.
Mutagenesis
The genotoxic potential of LUMVOA has not been evaluated.
Impairment of Fertility
Dedicated fertility studies have not been performed with LUMVOA. In the repeat-dose toxicology studies in sexually mature male and female cynomolgus monkeys, no effects on the reproductive system were observed at exposure higher (7-fold) than the human exposure (AUC) at the maximum recommended human dose.
14. Clinical Studies
LUMVOA was evaluated in 301 patients across 2 randomized, double-masked, placebo-controlled studies: active thyroid eye disease (Study 1: NCT05176639) and chronic thyroid eye disease (Study 2: NCT06021054). Patients were randomized to receive LUMVOA or placebo in a 2:1 ratio. Patients were given intravenous infusions of LUMVOA 10 mg/kg every 3 weeks for a total of 5 infusions. Patients in Study 1 had a clinical diagnosis of thyroid eye disease with onset within 15 months and a clinical activity score of 3 or more. Patients in Study 2 had a clinical diagnosis of thyroid eye disease with onset greater than 15 months and any clinical activity score (0-7). Prior orbital decompression surgery was permitted in either study if surgery was limited to bone. Patients with abnormal baseline audiometry Pure Tone Average (PTA) assessment or history of significant (as determined by the investigator) ear pathology, relevant ear surgery, or hearing loss were excluded. Patients with biopsy proven or clinical evidence of inflammatory bowel disease (IBD) were also excluded.
In Study 1, 75 patients with active thyroid eye disease were randomized to LUMVOA and 38 patients were randomized to placebo. The median age was 50 years (range 23 to 79 years), 77% were female, 62% were White, 6% were Black or African-American, 8% were Asian and 13% identified as Other. At baseline, 17% of patients were current users of tobacco. Proptosis ranged from 13.7 to 33.3 mm and 76 patients (67%) had diplopia at baseline.
In Study 2, 125 patients with chronic thyroid eye disease were randomized to LUMVOA and 63 patients were randomized to placebo. The median age was 52 years (range 20 to 77 years), 75% were female, 76% were White, 10% were Black or African-American, 3% were Asian and 4% identified as Other. At baseline, 26% of patients were current users of tobacco. Proptosis ranged from 14.1 to 35.0 mm and 102 patients (54%) had diplopia at baseline. Clinical activity scores ranged from 0 to 7 with 66 patients (35%) having a clinical activity score of 0 or 1 at baseline.
The proptosis responder rate at Week 15 was defined as the percentage of patients with ≥2 mm reduction in proptosis in the study eye from baseline, without deterioration in proptosis (≥2 mm increase) in the non-study eye. Additional evaluations included signs and symptoms of thyroid eye disease including diplopia, retrobulbar pain, gaze evoked orbital pain, eyelid swelling, eyelid erythema, conjunctival redness, chemosis, inflammation, clinical activity score, and assessments of quality of life (functional vision and patient appearance).
The proptosis results at Week 15 as measured by exophthalmometer in Studies 1 and 2 are provided in Table 2. Similar proptosis results were observed when measured by magnetic resonance imaging (MRI)/computed tomography (CT).
Table 2. Efficacy Results in Patients with Active Thyroid Eye Disease (Study 1) or Chronic Thyroid Eye Disease (Study 2):
| Study 1 (Active Thyroid Eye Disease) | Study 2 (Chronic Thyroid Eye Disease) | |||||
| LUMVOA (N=75) | Placebo (N=38) | Difference (95% CI) p-value | LUMVOA (N=125) | Placebo (N=63) | Difference (95% CI) p-value | |
| Proptosis responder rate at Week 15 – exophthalmometer, %1 | 70% | 5% | 65% (52, 78) <0.01 | 57% | 8% | 49% (38, 60) <0.01 |
| Proptosis (mm) average change from baseline at Week 15 – exophthalmometer, LS Mean (SE)2 | -2.9 (0.2) | -0.5 (0.2) | -2.4 (-3.0, -1.8) <0.01 | -2.4 (0.2) | -0.5 (0.2) | -1.9 (-2.4, -1.4) <0.01 |
1 Proptosis responder rate (PRR) results via exophthalmometer were analyzed based on a generalized estimating equation (GEE) model of baseline through Week 15 data.
2 Results were obtained from a mixed model for repeated measures (MMRM) with an unstructured covariance matrix and included treatment, baseline value, visit, treatment by visit, and visit by baseline value interaction as fixed effects. A change from Baseline of 0 was imputed at the first post-Baseline visit for any subject without a post-Baseline value.
In Studies 1 and 2, improvement of proptosis as measured by mean change from baseline was observed as early as 3 weeks and proptosis continued to improve through Week 15 in both active thyroid eye disease (Figure 1) and chronic thyroid eye disease (Figure 2).
Figure 1. Change from Baseline in Proptosis by Exophthalmometer over 15 Weeks for Patients with Active Thyroid Eye Disease (Study 1):
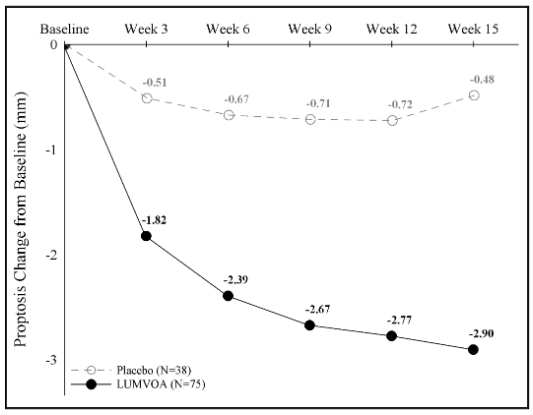
P<0.01 at each timepoint.
Figure 2. Change from Baseline in Proptosis by Exophthalmometer over 15 Weeks for Patients with Chronic Thyroid Eye Disease (Study 2):
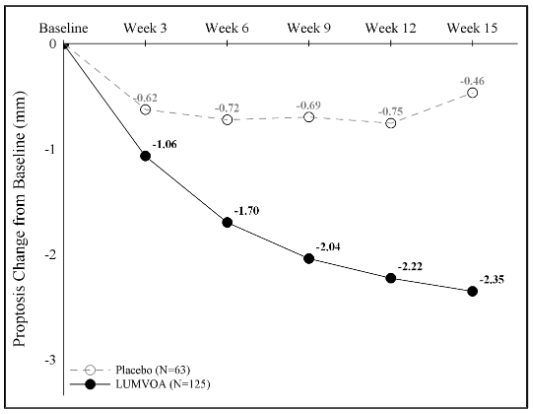
P<0.01 at each timepoint.
In both studies, LUMVOA also led to improvement in the less severely impacted non-study eye and a reduction in extraocular muscle volume in both eyes.
Diplopia (double vision) was evaluated in patients who had diplopia at baseline in Studies 1 and 2. Results are shown in Table 3. Diplopia resolution was observed as early as 3 weeks in active thyroid eye disease and 6 weeks in chronic thyroid eye disease.
Table 3. Diplopia in Patients with Active Thyroid Eye Disease (Study 1) or Chronic Thyroid Eye Disease (Study 2):
| Study 1 (Active Thyroid Eye Disease) | Study 2 (Chronic Thyroid Eye Disease) | |||||
| LUMVOA N=50 | Placebo N=26 | Difference (95% CI) p-value | LUMVOA N=65 | Placebo N=37 | Difference (95% CI) p-value | |
| Diplopia responder rate at Week 15, %1,2 | 59% | 20% | 39.2 (18.8, 59.6) <0.01 | 56% | 25% | 30.9 (12.3, 49.5) <0.01 |
| Diplopia resolution rate at Week 15, %1,3 | 49% | 12% | 37.7 (18.9, 56.6) <0.01 | 32% | 14% | 17.7 (1.6, 33.9) 0.02 |
1 Diplopia was evaluated on a 4-point scale where scores ranged from 0 for no diplopia to 3 for constant diplopia. Diplopia results were analyzed based on a GEE model of baseline through Week 15 data.
2 Diplopia response in a patient was defined as having a diplopia score >0 at baseline and achieving a reduction of at least 1 point on the diplopia scale at Week 15.
3 Diplopia resolution in a patient was defined as having a diplopia score >0 at baseline and a score of 0 at Week 15.
In Study 1, 71% of patients who were proptosis responders at Week 15 maintained proptosis response at 52 weeks and 50% of patients who achieved diplopia resolution at Week 15 maintained resolution at Week 52.
In Study 2, 57% of patients who were proptosis responders at Week 15 maintained proptosis response at 52 weeks and 80% of patients who achieved diplopia resolution at Week 15 maintained resolution at Week 52.
Subgroups
Examination of age and sex subgroups did not identify differences in response to LUMVOA among these subgroups. Reduction in proptosis and diplopia was similar between smokers and non-smokers in both studies.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.