NEORAL Oral solution Ref.[6694] Active ingredients: Ciclosporin
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2017 Publisher: Novartis Pharmaceuticals UK Ltd Trading as: Sandoz Pharmaceuticals, Frimley Business Park, Frimley, Camberley, Surrey, GU16 7SR
Therapeutic indications
Transplantation indications
Solid organ transplantation
Prevention of graft rejection following solid organ transplantation.
Treatment of transplant cellular rejection in patients previously receiving other immunosuppressive agents.
Bone marrow transplantation
Prevention of graft rejection following allogeneic bone marrow and stem cell transplantation.
Prevention or treatment of graft-versus-host disease (GVHD).
Non-transplantation indications
Endogenous uveitis
Treatment of sight-threatening intermediate or posterior uveitis of non-infectious aetiology in patients in whom conventional therapy has failed or caused unacceptable side effects.
Treatment of Behçet uveitis with repeated inflammatory attacks involving the retina in patients without neurological manifestations.
Nephrotic syndrome
Steroid-dependent and steroid-resistant nephrotic syndrome, due to primary glomerular diseases such as minimal change nephropathy, focal and segmental glomerulosclerosis, or membranous glomerulonephritis.
Neoral can be used to induce and maintain remissions. It can also be used to maintain steroid-induced remission, allowing withdrawal of steroids.
Rheumatoid arthritis
Treatment of severe, active rheumatoid arthritis.
Psoriasis
Treatment of severe psoriasis in patients in whom conventional therapy is inappropriate or ineffective.
Atopic dermatitis
Neoral is indicated in patients with severe atopic dermatitis when systemic therapy is required.
Posology and method of administration
Posology
The dose ranges given for oral administration are intended to serve as guidelines only.
The daily doses of Neoral should be given in two divided doses equally distributed throughout the day. It is recommended that Neoral be administered on a consistent schedule with regard to time of day and in relation to meals.
Neoral should only be prescribed by, or in close collaboration with, a physician with experience of immunosuppressive therapy and/or organ transplantation.
Transplantation
Solid organ transplantation
Treatment with Neoral should be initiated within 12 hours before surgery at a dose of 10 to 15 mg/kg given in 2 divided doses. This dose should be maintained as the daily dose for 1 to 2 weeks post-operatively, being gradually reduced in accordance with blood levels according to local immunosuppressive protocols until a recommended maintenance dose of about 2 to 6 mg/kg given in 2 divided doses is reached.
When Neoral is given with other immunosuppressants (e.g. with corticosteroids or as part of a triple or quadruple medicinal product therapy), lower doses (e.g. 3 to 6 mg/kg given in 2 divided doses for the initial treatment) may be used.
Bone marrow transplantation
The initial dose should be given on the day before transplantation. In most cases, Sandimmun concentrate for solution for infusion is preferred for this purpose. The recommended intravenous dose is 3 to 5 mg/kg/day. Infusion is continued at this dose level during the immediate post-transplant period of up to 2 weeks, before a change is made to oral maintenance therapy with Neoral at daily doses of about 12.5 mg/kg given in 2 divided doses.
Maintenance treatment should be continued for at least 3 months (and preferably for 6 months) before the dose is gradually decreased to zero by 1 year after transplantation.
If Neoral is used to initiate therapy, the recommended daily dose is 12.5 to 15 mg/kg given in 2 divided doses, starting on the day before transplantation.
Higher doses of Neoral, or the use of Sandimmun intravenous therapy, may be necessary in the presence of gastrointestinal disturbances which might decrease absorption.
In some patients, GVHD occurs after discontinuation of ciclosporin treatment, but usually responds favourably to re-introduction of therapy. In such cases an initial oral loading dose of 10 to 12.5 mg/kg should be given, followed by daily oral administration of the maintenance dose previously found to be satisfactory. Low doses of Neoral should be used to treat mild, chronic GVHD.
Non-transplantation indications
When using Neoral in any of the established non-transplantation indications, the following general rules should be adhered to:
Before initiation of treatment a reliable baseline level of renal function should be established by at least two measurements. The estimated glomerular filtration rate (eGFR) by the MDRD formula can be used for estimation of renal function in adults and an appropriate formula should be used to assess eGFR in paediatric patients. Since Neoral can impair renal function, it is necessary to assess renal function frequently. If eGFR decreases by more than 25% below baseline at more than one measurement, the dosage of Neoral should be reduced by 25 to 50%. If the eGFR decrease from baseline exceeds 35%, further reduction of the dose of Neoral should be considered. These recommendations apply even if the patient's values still lie within the laboratory's normal range. If dose reduction is not successful in improving eGFR within one month, Neoral treatment should be discontinued (see section 4.4).
Regular monitoring of blood pressure is required.
The determination of bilirubin and parameters that assess hepatic function are required prior to starting therapy and close monitoring during treatment is recommended. Determinations of serum lipids, potassium, magnesium and uric acid are advisable before treatment and periodically during treatment.
Occasional monitoring of ciclosporin blood levels may be relevant in non-transplant indications, e.g. when Neoral is co-administered with substances that may interfere with the pharmacokinetics of ciclosporin, or in the event of unusual clinical response (e.g. lack of efficacy or increased drug intolerance such as renal dysfunction).
The normal route of administration is by mouth. If the concentrate for solution for infusion is used, careful consideration should be given to administering an adequate intravenous dose that corresponds to the oral dose. Consultation with a physician with experience of use of ciclosporin is recommended.
Except in patients with sight-threatening endogenous uveitis and in children with nephrotic syndrome, the total daily dose must never exceed 5 mg/kg.
For maintenance treatment the lowest effective and well tolerated dosage should be determined individually.
In patients in whom within a given time (for specific information see below) no adequate response is achieved or the effective dose is not compatible with the established safety guidelines, treatment with Neoral should be discontinued.
Endogenous uveitis
For inducing remission, initially 5 mg/kg/day orally given in 2 divided doses are recommended until remission of active uveal inflammation and improvement in visual acuity are achieved. In refractory cases, the dose can be increased to 7 mg/kg/day for a limited period.
To achieve initial remission, or to counteract inflammatory ocular attacks, systemic corticosteroid treatment with daily doses of 0.2 to 0.6 mg/kg prednisone or an equivalent may be added if Neoral alone does not control the situation sufficiently. After 3 months, the dose of corticosteroids may be tapered to the lowest effective dose.
For maintenance treatment, the dose should be slowly reduced to the lowest effective level. During the remission phases, this should not exceed 5 mg/kg/day.
Infectious causes of uveitis should be ruled out before immunosuppressants can be used.
Nephrotic syndrome
For inducing remission, the recommended daily dose is given in 2 divided oral doses.
If the renal function (except for proteinuria) is normal, the recommended daily dose is the following:
- adults: 5 mg/kg
- children: 6 mg/kg
In patients with impaired renal function, the initial dose should not exceed 2.5 mg/kg/day.
The combination of Neoral with low doses of oral corticosteroids is recommended if the effect of Neoral alone is not satisfactory, especially in steroid-resistant patients.
Time to improvement varies from 3 to 6 months depending on the type of glomerulopathy. If no improvement has been observed after this time to improvement period, Neoral therapy should be discontinued.
The doses need to be adjusted individually according to efficacy (proteinuria) and safety, but should not exceed 5 mg/kg/day in adults and 6 mg/kg/day in children.
For maintenance treatment, the dose should be slowly reduced to the lowest effective level.
Rheumatoid arthritis
For the first 6 weeks of treatment the recommended dose is 3 mg/kg/day orally given in 2 divided doses. If the effect is insufficient, the daily dose may then be increased gradually as tolerability permits, but should not exceed 5 mg/kg. To achieve full effectiveness, up to 12 weeks of Neoral therapy may be required.
For maintenance treatment the dose has to be titrated individually to the lowest effective level according to tolerability.
Neoral can be given in combination with low-dose corticosteroids and/or non-steroidal anti-inflammatory drugs (NSAIDs) (see section 4.4). Neoral can also be combined with low-dose weekly methotrexate in patients who have insufficient response to methotrexate alone, by using 2.5 mg/kg Neoral in 2 divided doses per day initially, with the option to increase the dose as tolerability permits.
Psoriasis
Neoral treatment should be initiated by physicians with experience in the diagnosis and treatment of psoriasis. Due to the variability of this condition, treatment must be individualised. For inducing remission, the recommended initial dose is 2.5 mg/kg/day orally given in 2 divided doses. If there is no improvement after 1 month, the daily dose may be gradually increased, but should not exceed 5 mg/kg. Treatment should be discontinued in patients in whom sufficient response of psoriatic lesions cannot be achieved within 6 weeks on 5 mg/kg/day, or in whom the effective dose is not compatible with the established safety guidelines (see section 4.4).
Initial doses of 5 mg/kg/day are justified in patients whose condition requires rapid improvement. Once satisfactory response is achieved, Neoral may be discontinued and subsequent relapse managed with re-introduction of Neoral at the previous effective dose. In some patients, continuous maintenance therapy may be necessary.
For maintenance treatment, doses have to be titrated individually to the lowest effective level, and should not exceed 5 mg/kg/day.
Atopic dermatitis
Neoral treatment should be initiated by physicians with experience in the diagnosis and treatment of atopic dermatitis. Due to the variability of this condition, treatment must be individualised. The recommended dose range is 2.5 to 5 mg/kg/day given in 2 divided oral doses. If a starting dose of 2.5 mg/kg/day does not achieve a satisfactory response within 2 weeks, the daily dose may be rapidly increased to a maximum of 5 mg/kg. In very severe cases, rapid and adequate control of the disease is more likely to occur with a starting dose of 5 mg/kg/day. Once satisfactory response is achieved, the dose should be reduced gradually and, if possible, Neoral should be discontinued. Subsequent relapse may be managed with a further course of Neoral.
Although an 8-week course of therapy may be sufficient to achieve clearing, up to 1 year of therapy has been shown to be effective and well tolerated, provided the monitoring guidelines are followed.
Switching from Sandimmun oral formulations to Neoral
The available data indicate that after a 1:1 switch from oral Sandimmun to Neoral, the trough concentrations of ciclosporin in whole blood are comparable. In many patients, however, higher peak concentrations (Cmax) and increased exposure to the active substance (AUC) may occur. In a small percentage of patients these changes are more marked and may be of clinical significance. In addition, the absorption of ciclosporin from Neoral is less variable and the correlation between ciclosporin trough concentrations and exposure (in terms of AUC) is stronger than with oral Sandimmun.
Since the switch from oral Sandimmun to Neoral may result in increased exposure to ciclosporin, the following rules must be observed:
In transplant patients, Neoral should be started at the same daily dose as was previously used with oral Sandimmun. Ciclosporin trough concentrations in whole blood should be monitored initially within 4 to 7 days after the switch to Neoral. In addition, clinical safety parameters such as renal function and blood pressure must be monitored during the first 2 months after the switch. If the ciclosporin trough blood levels are beyond the therapeutic range, and/or worsening of the clinical safety parameters occurs, the dosage must be adjusted accordingly.
In patients treated for non-transplantation indications, Neoral should be started with the same daily dose as was used with oral Sandimmun. Two, 4 and 8 weeks after the switch, renal function and blood pressure should be monitored. If blood pressure significantly exceed the pre-switch levels or if eGFR decreases by more than 25% below the value measured prior to Sandimmun therapy at more than one measurement, the dose should be reduced (see also 'Additional precautions' in section 4.4). In the event of unexpected toxicity or inefficacy of ciclosporin, blood trough levels should also be monitored.
Switching between oral ciclosporin formulations
The switch from one oral ciclosporin formulation to another should be made under physician supervision, including monitoring of blood levels of ciclosporin for transplantation patients.
Special populations
Patients with renal impairment
All indications
Ciclosporin undergoes minimal renal elimination and its pharmacokinetics are not extensively affected by renal impairment (see section 5.2). However, due to its nephrotoxic potential (see section 4.8), careful monitoring of renal function is recommended (see section 4.4).
Non-transplantation indications
With the exception of patients being treated for nephrotic syndrome, patients with impaired renal function should not receive ciclosporin (see subsection on additional precautions in non-transplantation indications in section 4.4). In nephrotic syndrome patients with impaired renal function, the initial dose should not exceed 2.5 mg/kg/day.
Patients with hepatic impairment
Ciclosporin is extensively metabolised by the liver. An approximate 2- to 3-fold increase in ciclosporin exposure may be observed in patients with hepatic impairment. Dose reduction may be necessary in patients with severe liver impairment to maintain blood levels within the recommended target range (see sections 4.4 and 5.2) and it is recommended that ciclosporin blood levels are monitored until stable levels are reached.
Paediatric population
Clinical studies have included children from 1 year of age. In several studies, paediatric patients required and tolerated higher doses of ciclosporin per kg body weight than those used in adults.
Use of Neoral in children for non-transplantation indications other than nephrotic syndrome cannot be recommended (see section 4.4).
Elderly population (age 65 years and above)
Experience with Neoral in the elderly is limited.
In rheumatoid arthritis clinical trials with ciclosporin, patients aged 65 or older were more likely to develop systolic hypertension on therapy, and more likely to show serum creatinine rises ≥50% above the baseline after 3 to 4 months of therapy.
Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or medication and increased susceptibility for infections.
Method of administration
Oral use.
Neoral Oral Solution should be diluted, preferably with orange or apple juice. However, other drinks, such as soft drinks, can be used accordingly to individual taste. The solution should be stirred well immediately before it is taken. Owing to its possible interference with the cytochrome P450-dependent enzyme system, grapefruit or grapefruit juice should be avoided for dilution (see section 4.5). The syringe should not come in contact with the diluent. If the syringe is to be cleaned, do not rinse it but wipe the outside with a dry tissue (see section 6.6).
Precautions to be taken before handling or administering the medicinal product
For instructions on dilution of the medicinal product before administration, see section 6.6.
Overdose
The oral LD50 of ciclosporin is 2,329 mg/kg in mice, 1,480 mg/kg in rats and >1,000 mg/kg in rabbits. The intravenous LD50 is 148 mg/kg in mice, 104 mg/kg in rats, and 46 mg/kg in rabbits.
Symptoms
Experience with acute overdosage of ciclosporin is limited. Oral doses of ciclosporin of up to 10 g (about 150 mg/kg) have been tolerated with relatively minor clinical consequences, such as vomiting, drowsiness, headache, tachycardia and in a few patients moderately severe, reversible impairment of renal function. However, serious symptoms of intoxication have been reported following accidental parenteral overdosage with ciclosporin in premature neonates.
Treatment
In all cases of overdosage, general supportive measures should be followed and symptomatic treatment applied. Forced emesis and gastric lavage may be of value within the first few hours after oral intake. Ciclosporin is not dialysable to any great extent, nor is it well cleared by charcoal haemoperfusion.
Shelf life
36 months.
Special precautions for storage
NEORAL Oral Solution should be stored between 15 and 30°C, but preferably not below 20°C for more than 1 month as it contains oily components of natural origin which tend to solidify at low temperatures. A jelly-like formation may occur below 20°C, which is however reversible at temperatures up to 30°C. Minor flakes or slight sediment may still be observed. These phenomena do not affect the efficacy and safety of the product and the dosing by means of the pipette remains accurate. After opening, NEORAL Oral Solution should be used within 2 months.
Nature and contents of container
NEORAL Oral Solution is available in 20 mL and 50 mL amber glass bottles with a rubber stopper and aluminium tear-off cap. The tear-off cap indicates if the bottle has been previously opened. A white polypropylene cap is provided for closure of the bottle during the in-use period.
Not all pack sizes may be marketed.
Special precautions for disposal and other handling
Neoral Oral Solution is provided with two syringes for measuring the doses. The 1-ml syringe is used to measure doses less than or equal to 1 ml (each graduation of 0.05 ml corresponds to 5 mg of ciclosporin). The 4-ml syringe is used to measure doses greater than 1 ml and up to 4 ml (each graduation of 0.1 ml corresponds to 10 mg of ciclosporin).
Initial use of Neoral Oral Solution
1. Raise the flap in the centre of the metal sealing ring.

2. Tear off the sealing ring completely.
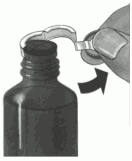
3. Remove the black stopper and throw it away.

4. Push the tube unit with the white stopper firmly into the neck of the bottle.
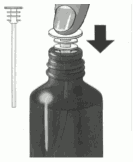
5. Choose the syringe depending on the prescribed volume. For volume less than 1 ml or equal to 1 ml, use the 1-ml syringe. For volume greater than 1 ml, use the 4-ml syringe. Insert the nozzle of the syringe into the white stopper.

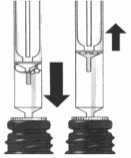
6. Draw up the prescribed volume of solution (position the lower part of the plunger ring in front of the graduation corresponding to the prescribed volume).

7. Expel any large bubbles by depressing and withdrawing the plunger a few times before removing the syringe containing the prescribed dose from bottle. The presence of a few tiny bubbles is of no importance and will not affect the dose in any way.
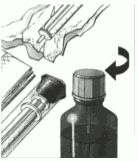
8. Push the medicine out of the syringe into a small glass with some liquid (not grapefruit juice). Avoid any contact between the syringe and the liquid in the glass. The medicine can be mixed just before it is taken. Stir and drink the entire mixture right away. Once mixed it should be taken immediately after preparation.

9. After use, wipe the syringe on the outside only with a dry tissue and replace it in its cover. The white stopper and tube should remain in the bottle. Close the bottle with the cap provided.
Subsequent use
Commence at point 5.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.