NERLYNX Film-coated tablet Ref.[10146] Active ingredients: Neratinib
Source: FDA, National Drug Code (US) Revision Year: 2024
12.1. Mechanism of Action
Neratinib is an intracellular kinase inhibitor that irreversibly binds to epidermal growth factor receptor (EGFR), HER2, and HER4. In vitro, neratinib reduces EGFR and HER2 autophosphorylation, downstream MAPK and AKT signaling pathways, and showed antitumor activity in EGFR and/or HER2 expressing carcinoma cell lines. Neratinib human metabolites M3, M6, M7 and M11 inhibited the activity of EGFR, HER2, and HER4 in vitro. In vivo, oral administration of neratinib inhibited tumor growth in mouse xenograft models with tumor cell lines expressing HER2 and EGFR.
12.2. Pharmacodynamics
Neratinib exposure-response relationships and the time course of pharmacodynamic response are unknown.
Cardiac Electrophysiology
The effect of NERLYNX on the QTc interval was evaluated in a randomized, placebo, and positive-controlled, double-blind, single-dose, crossover study in 60 healthy subjects. At 140% the therapeutic exposures of NERLYNX, there was no clinically relevant effect on the QTc interval.
12.3. Pharmacokinetics
Neratinib AUC increases in less than dose proportional manner over a daily dose range of 40 to 400 mg (0.17 to 1.7 times the maximum approved recommended dosage).
Absorption
Peak concentrations of neratinib and major active metabolites M3, M6 and M7 are reached in the range of 2 to 8 hours after oral administration.
Effect of Food
A high-fat meal (approximately 55% fat, 31% carbohydrate, and 14% protein) increased neratinib Cmax and AUC infby 70% (90% CI: 1.1–2.7) and 120% (90% CI: 1.4–3.5), respectively, in healthy subjects compared to fasting conditions. A standard breakfast (approximately 50% carbohydrate, 35% fat, and 15% protein) increased the Cmax and AUC infby 20% (90% CI: 0.97–1.42) and 10% (90% CI: 1.02–1.24), respectively, in healthy subjects [see Dosage and Administration ( 2.2)] .
Distribution
The mean (%CV) apparent volume of distribution at steady state (V ss/F) was 6433 (19%) L in patients. In vitro protein binding of neratinib was greater than 99%, predominantly to serum albumin and alpha-1 acid glycoprotein, and was independent of concentration.
Elimination
The mean (%CV) plasma half-life of neratinib, M3, M6, and M7 was 14.6 (38%), 21.6 (77%), 13.8 (50%) and 10.4 (33%) hours, respectively, in healthy subjects. The mean elimination half-life of neratinib ranged from 7 to 17 hours following a single oral dose in patients. The mean (%CV) CL/F after first dose and at steady state (day 21) were 216 (34%) and 281 (40%) L/hour, respectively, in patients.
Metabolism
Neratinib is metabolized primarily in the liver by CYP3A4 and to a lesser extent by flavin-containing monooxygenase (FMO).
Neratinib represents the most prominent component in plasma. The systemic exposures (AUC) of the active metabolites M3, M6, M7 and M11 were 15%, 33%, 22%, and 4% of the systemic neratinib exposure, respectively, at steady state in healthy subjects.
Excretion
After oral administration of radiolabeled neratinib 200 mg (0.83 times of maximum approved recommended dosage), fecal excretion accounted for approximately 97% and urinary excretion accounted for 1.1% of the total dose. Sixty-one percent of the excreted radioactivity was recovered within 96 hours and 98% was recovered after 10 days.
Specific Populations
Age, sex, race, and renal function do not have a clinically significant effect on neratinib pharmacokinetics.
Patients With Hepatic Impairment
Neratinib exposures in patients with mild (Child Pugh A) and moderate hepatic impairment (Child Pugh B) were similar to that in healthy subjects with normal hepatic function. Neratinib Cmax and AUC increased by 173% and 181%, respectively, in patients with severe hepatic impairment (Child Pugh C) as compared to subjects with normal hepatic function [see Dosage and Administration (2.4) and Use in Specific Populations (8.6)].
Drug Interaction Studies
Clinical Studies and Model-Informed Approaches
Gastric Acid Reducing Agents: Concomitant use with lansoprazole (proton pump inhibitor) decreased neratinib Cmax by 71% and AUC by 65%. When NERLYNX was administered 2 hours after ranitidine (H2receptor antagonist), the neratinib Cmax was reduced by 57% and AUC by 48%. When NERLYNX was administered 2 hours prior to ranitidine, neratinib Cmax was reduced by 44% and AUC by 32% [see Dosage and Administration (2.5) and Drug Interactions (7.1)].
Strong CYP3A4 Inhibitors: Concomitant use of ketoconazole (strong inhibitor of CYP3A4 and P-gp inhibitor) increased neratinib Cmax by 221% and AUC by 381% [see Drug Interactions (7.1)].
P-gp and moderate CYP3A4 Dual Inhibitors: Verapamil (moderate CYP3A4 and P-gp dual inhibitor) increased the Cmax and AUC of neratinib by 203% and 299%, respectively [see Drug Interactions (7.1)].
Moderate CYP3A4 Inhibitors: Fluconazole (moderate CYP3A4 inhibitor) increased the Cmax and AUC of neratinib by 30% and 68%, respectively.
Strong and Moderate CYP3A4 Inducers: Concomitant use of rifampin (strong CYP3A4 inducer) decreased neratinib Cmax by 76% and AUC by 87%. The AUC of active metabolites M6 and M7 were also reduced by 37–49% when compared to NERLYNX administered alone. Efavirenz (moderate CYP3A4 inducer) decreased the Cmax of neratinib by 36% and AUC by 52% [see Drug Interactions (7.1)].
Effect of NERLYNX on P-gp Transporters: Concomitant use of NERLYNX increased the mean digoxin (P-gp substrate) Cmax by 54% and AUC by 32% [see Drug Interactions (7.2)].
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
A two-year carcinogenicity study was conducted in rats at oral neratinib doses of 1, 3, and 10 mg/kg/day. Neratinib was not carcinogenic in male and female rats at exposure levels >25 times the AUC in patients receiving the maximum recommended dose of 240 mg/day. Neratinib was not carcinogenic in a 26-week study in Tg.rasH2 transgenic mice when administered daily by oral gavage at doses up to 50 mg/kg/day in males and 125 mg/kg/day in females.
Neratinib was not mutagenic in an in vitro bacterial reverse mutation (AMES) assay or clastogenic in an in vitro human lymphocyte chromosomal aberration assay or an in vivo rat bone marrow micronucleus assay.
In a fertility study in rats, neratinib administration up to 12 mg/kg/day (approximately 0.5 times the maximum recommended dose of 240 mg/day in patients on a mg/m² basis) caused no effects on mating or the ability of animals to become pregnant. In repeat-dose toxicity studies in dogs with oral administration of neratinib daily for up to 39 weeks, tubular hypoplasia of the testes was observed at ≥0.5 mg/kg/day. This finding was observed at AUCs that were approximately 0.4 times the AUC in patients at the maximum recommended dose of 240 mg.
14. Clinical Studies
14.1 Extended Adjuvant Treatment of Early Stage Breast Cancer
The safety and efficacy of NERLYNX were investigated in the ExteNET trial (NCT00878709), a multicenter, randomized, double-blind, placebo-controlled study of NERLYNX after adjuvant treatment with a trastuzumab based therapy in women with HER2-positive breast cancer.
A total of 2840 patients with early-stage (Stage 1 to 3c) HER2-positive breast cancer within two years of completing treatment with adjuvant trastuzumab was randomized to receive either NERLYNX (n=1420) or placebo (n=1420). Randomization was stratified by the following factors: hormone receptor status, nodal status (0, 1–3 vs 4 or more positive nodes) and whether trastuzumab was given sequentially versus concurrently with chemotherapy. NERLYNX 240 mg or placebo was given orally once daily for one year. The major efficacy outcome measure was invasive disease-free survival (iDFS) defined as the time between the date of randomization to the first occurrence of invasive recurrence (local/regional, ipsilateral, or contralateral breast cancer), distant recurrence, or death from any cause, with 2 years and 28 days of follow-up.
Patient demographics and tumor characteristics were generally balanced between treatment arms. Patients had a median age of 52 years (range 23 to 83) and 12% of patients were 65 or older. The majority of patients were White (81%), and most patients (99.7%) had an ECOG performance status of 0 or 1. Fifty-seven percent (57%) of patients had hormone receptor positive disease (defined as ER-positive and/or PR-positive), 24% were node negative, 47% had one to three positive nodes and 30% had four or more positive nodes. Ten percent (10%) of patients had Stage I disease, 41% had Stage II disease and 31% had Stage III disease. The majority of patients (81%) were enrolled within one year of completion of trastuzumab treatment. Median time from the last adjuvant trastuzumab treatment to randomization was 4.4 months in the NERLYNX arm versus 4.6 months in the placebo arm. Median duration of treatment was 11.6 months in the NERLYNX arm vs 11.8 months in the placebo arm.
The efficacy results from the ExteNET trial are summarized in Table 11 and Figure 1.
Table 11. Efficacy iDFS Results for the ITT Population:
| Number of Events/Total N (%) | iDFS at 24 months,* % (95% CI) | Stratified† HR (95% CI) | P-value‡ | ||
|---|---|---|---|---|---|
| NERLYNX | Placebo | NERLYNX | Placebo | ||
| 67/1420 (4.7) | 106/1420 (7.5) | 94.2 (92.6, 95.4) | 91.9 (90.2, 93.2) | 0.66 (0.49, 0.90) | 0.008 |
CI=Confidence Interval; HR=Hazard Ratio; iDFS=Invasive Disease Free-Survival; ITT=Intent to Treat
* Kaplan-Meier estimate
† Stratified by prior trastuzumab (concurrent vs sequential), nodal status (0–3 positive nodes vs ≥4 positive nodes), and ER/PR status (positive vs negative)
‡ Stratified log-rank test
Figure 1. iDFS in the ExteNET Trial - ITT Population:
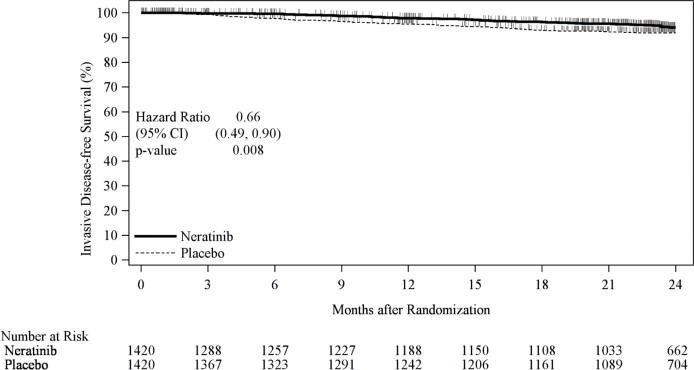
CI=Confidence Interval; HR=Hazard Ratio; iDFS=Invasive Disease Free-Survival; ITT=Intent to Treat
Table 12. Subgroup Analyses*:
| Population | Number of Events/Total N (%) | iDFS at 24 Months,† % (95% CI) | nstratified HR (95% CI) | ||
|---|---|---|---|---|---|
| NERLYNX | Placebo | NERLYNX | Placebo | ||
| Hormone Receptor Status | |||||
| Positive | 29/816 (3.6) | 63/815 (7.7) | 95.6 (93.8, 96.9) | 91.5 (89.2, 93.3) | 0.49 (0.31, 0.75) |
| Negative | 38/604 (6.3) | 43/605 (7.1) | 92.2 (89.4, 94.3) | 92.4 (89.8, 94.3) | 0.93 (0.60, 1.43) |
| Nodal Status | |||||
| Negative | 7/335 (2.1) | 11/336 (3.3) | 97.2 (94.1, 98.7) | 96.5 (93.7, 98.0) | 0.72 (0.26, 1.83) |
| 1–3 Positive Nodes | 31/664 (4.7) | 47/664 (7.1) | 94.4 (92.2, 96.1) | 92.4 (90.0, 94.2) | 0.68 (0.43, 1.07) |
| ≥4 Positive Nodes | 29/421 (6.9) | 48/420 (11.4) | 91.4 (87.9, 94.0) | 87.3 (83.4, 90.2) | 0.62 (0.39, 0.97) |
| Prior Trastuzumab | |||||
| Concurrent | 49/884 (5.5) | 66/886 (7.4) | 93.2 (91.0, 94.8) | 92.0 (89.9, 93.7) | 0.80 (0.55, 1.16) |
| Sequential | 18/536 (3.4) | 40/534 (7.5) | 95.8 (93.4, 97.3) | 91.6 (88.7, 93.8) | 0.46 (0.26, 0.78) |
| Completion of Prior Trastuzumab | |||||
| ≤1 year | 58/1152 (5.0) | 95/1145 (8.3) | 93.8 (92.0, 95.2) | 90.9 (89.0, 92.5) | 0.63 (0.45, 0.88) |
| 1–2 years | 9/262 (3.4) | 11/270 (4.1) | 95.8 (92.0, 97.8) | 95.7 (92.3, 97.6) | 0.92 (0.37, 2.22) |
CI= Confidence Interval; HR=Hazard Ratio; iDFS=Invasive Disease Free-Survival; ITT=Intent to Treat
CI=Confidence Interval; HR=Hazard Ratio
* Exploratory analyses without adjusting multiple comparisons
† Kaplan-Meier estimate
Approximately 75% of patients were re-consented for extended follow-up beyond 24 months. Observations with missing data were censored at the last date of assessment. This exploratory analysis suggests that the iDFS results at 5 years are consistent with the 2-year iDFS results observed in ExteNET. After a median follow-up of 8. years, there was no statistically significant difference in OS between the NERLYNX and the placebo arm [HR 0.95 (95% CI: 0.75, 1.21)]. The 5-year estimate of OS was 94.1% (95% CI, 92.7%, 95.3%) in the NERLYNX arm and 93.3% (95% CI, 91.8%, 94.5%) in the placebo arm.
14.2 Advanced or Metastatic Breast Cancer
The safety and efficacy of NERLYNX in combination with capecitabine was studied in NALA (NCT01808573), a randomized, multicenter, open-label clinical trial in patients (n=621) with metastatic HER2 positive breast cancer who had received 2 or more prior anti-HER2 based regimens in the metastatic setting. HER2 expression was based on archival tissue tested at a central laboratory prior to enrollment. HER2 positivity was defined as a HER2 immunohistochemistry (IHC) score of 3+ or IHC 2+ with confirmatory in situ hybridization (ISH) positive. Fifty-nine percent of these patients were hormone receptor positive (HR+) and 41% were hormone receptor negative (HR-); 69% had received two prior anti-HER2 based regimens, 31% had received three or more prior anti-HER2 based regimens, 81% had visceral disease, and 19% had non-visceral-only disease. Patients with asymptomatic or stable brain metastases were included in NALA trial (16%).
Patients were randomized (1:1) to receive NERLYNX 240 mg orally once daily on Days 1–21 in combination with capecitabine 750 mg/m² given orally twice daily on Days 1–14 for each 21–day cycle (n=307) or lapatinib 1250 mg orally once daily Days 1–21 in combination with capecitabine 1000 mg/m² given orally twice daily on Days 1-14 for each 21-day cycle (n=314). Patients were treated until disease progression or unacceptable toxicity.
The efficacy results from the NALA trial are summarized in Table 13, Figure 2, and Figure 3.
Table 13. Efficacy Results – NALA Trial (Central Assessment):
| NERLYNX + Capecitabine (n=307) | Lapatinib + Capecitabine (n=314) | |
|---|---|---|
| Progression Free Survival (PFS) | ||
| Number of Events (%) | 210 (68.4) | 223 (71.0) |
| Median PFS, months (95% CI) | 5.6 (4.9, 6.9) | 5.5 (4.3, 5.6) |
| HR (95% CI)* | 0.76 (0.63,0.93) | |
| p-value† | 0.0059 | |
| PFS rates at 12 months, % (95% CI)α | 29 (23, 35) | 15 (10, 20) |
| PFS rates at 24 months, % (95% CI)‡,α | 12 (7, 18) | 3 (1, 8) |
| Overall Survival (OS) | ||
| Number of Events (%) | 192 (62.5) | 218 (69.4) |
| Median OS, months (95% CI) | 21.0 (17.7, 23.8) | 18.7 (15.5, 21.2) |
| HR (95% CI)* | 0.88 (0.72, 1.07) | |
| p-value† | 0.2086 | |
| Objective Response Rate (ORR)§ | ||
| ORR, % (95% CI) | 32.8 (27.1, 38.9) | 26.7 (21.5, 32.4) |
| Duration of Response (DOR) | ||
| Median DOR, months (95% CI) | 8.5 (5.6, 11.2) | 5.6 (4.2, 6.4) |
HR=Hazard Ratio
* Hazard ratio is presented as NERLYNX plus Capecitabine (N+C) vs Lapatinib plus Capecitabine (L+C).
† Stratified log-rank test
‡ The total number of patients remaining on study at 24 months is 11; with 9 patients on N+C and 2 patients on L+C.
α Exploratory analysis
§ Confirmed ORR
Figure 2. Progression Free Survival (Central Assessment - ITT Population):
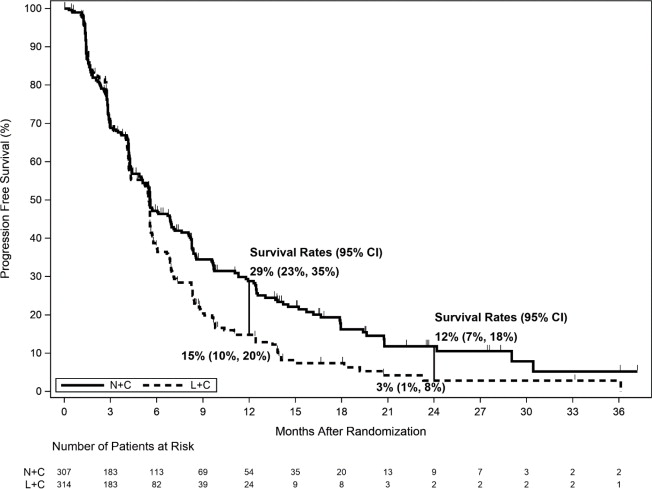
Figure 3. Overall Survival (ITT Population):
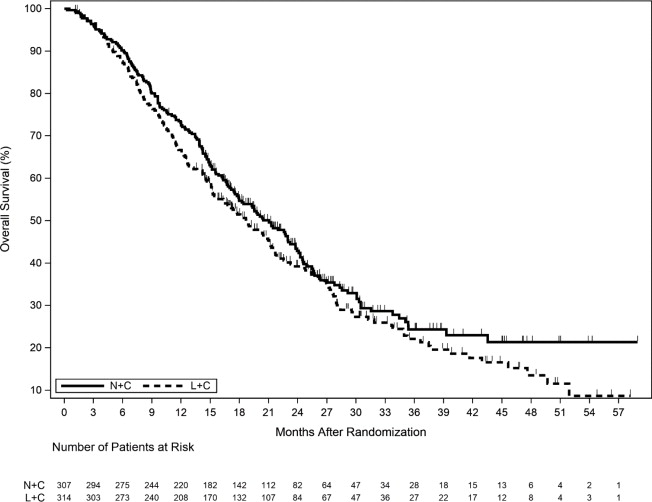
Table 14. Progression-Free Survival Rates - Subgroup Analysesα:
| Population | Number of Events/Total N (%) | PFS Rates (%) at 12 Months (95% CI) | ||
|---|---|---|---|---|
| NERLYNX + Capecitabine | Lapatinib + Capecitabine | NERLYNX + Capecitabine | Lapatinib + Capecitabine | |
| Disease Location | ||||
| Visceral | 181/247 (73.3) | 185/253 (73.1) | 23 (17, 30) | 14 (10, 20) |
| Non Visceral | 29/60 (48.3) | 38/61 (62.3) | 53 (38, 66) | 18 (7, 32) |
| Hormone Receptor Status | ||||
| Positive | 128/181 (70.7) | 115/186 (61.8) | 27 (19, 34) | 23 (15, 31) |
| Negative | 82/126 (65.1) | 108/128 (84.4) | 32 (23, 41) | 5 (2, 11) |
| Previous HER2 regimens | ||||
| 2 regimens | 148/215 (68.8) | 151/215 (70.2) | 26 (20, 33) | 13 (8, 19) |
| ≥3 regimens | 62/92 (67.4) | 72/99 (72.7) | 34 (24, 45) | 19 (11, 29) |
CI=Confidence Interval; PFS=Progression-Free Survival
α Exploratory Analysis
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.