OGSIVEO Film-coated tablet Ref.[107378] Active ingredients: Nirogacestat
Source: FDA, National Drug Code (US) Revision Year: 2023
12.1. Mechanism of Action
Nirogacestat is a gamma secretase inhibitor that blocks proteolytic activation of the Notch receptor. When dysregulated, Notch can activate pathways that contribute to tumor growth.
12.2. Pharmacodynamics
Exposure-Response Relationships
There is an exposure-response relationship between nirogacestat exposure and Grade 3 hypophosphatemia with a higher risk of Grade 3 hypophosphatemia at higher exposure.
Cardiac Electrophysiology
At the recommended dosage, a mean increase in the QTc interval > 20 ms was not observed.
12.3. Pharmacokinetics
Nirogacestat pharmacokinetic parameters in patients with desmoid tumors are summarized in Table 6.
Table 6. Pharmacokinetic Parameters and Characteristics of Nirogacestat:
| General Information | ||
| Steady state exposure [Mean (%CV)] | Cmax | 508 (62) ng/mL |
| AUC0-tau | 3370 (58) ng·h/mL | |
| Time to steady-state | Approximately 6 days | |
| Accumulation ratio [Median (Min, Max)] | 1.6 (1.3, 4.6) | |
| Absorption | ||
| Tmax [Median (Min, Max)] | 1.5 (0.5, 6.5) hours | |
| Absolute bioavailability | 19% | |
| Food effect [dose-normalized GMR% (90% CI)] | Cmax | 93 % (55%, 166%) |
| AUC | 114% (76%, 171%) | |
| Distribution | ||
| Protein Binding* | Serum protein binding | 99.6% |
| Human serum albumin | 94.6% | |
| α-1 acid glycoprotein | 97.9% | |
| Apparent volume of distribution (Vz/F) [Mean (%CV)] | 1430 (65) L | |
| Elimination | ||
| Apparent Systemic Clearance (CL/F) [Mean (%CV)] | 45 (58) L/hr | |
| Terminal elimination half-life (t1/2) [Mean (%CV)] | 23 (37) hr | |
| Metabolism | ||
| Primary pathway | N-dealkylation via CYP3A4 (85%) | |
| Secondary pathways | Metabolism by CYP 3A4, 2C19, 2C9, and 2D6 | |
| Excretion | ||
| Feces | 38% | |
| Urine | 17% (<1% unchanged) | |
| Expired air | 9.7% | |
* Protein binding values reflect results from separate assays.
Abbreviations: AUC0-tau = area under the time concentration curve to the dosing interval;
Cmax = maximum plasma concentration; Tmax = time to reach Cmax; GMR = geometric mean ratio
Specific Populations
No clinically significant differences in the pharmacokinetics of nirogacestat were observed based on age (18 to 80 years), sex, race (Asian, Black or African American, and White), or mild or moderate renal impairment (eGFR ≥41 mL/min/1.73m2).
Effects of Hepatic Impairment
The mean AUC increased by up to 16% and the mean Cmax decreased by up to 39% in subjects with moderate hepatic impairment identified by Child-Pugh Class B or NCI-ODWG Group C criteria compared to that of subjects with normal hepatic function.
Insufficient data are available to characterize nirogacestat PK in patients with severe hepatic impairment.
Drug Interaction Studies
Clinical Studies and Model-Informed Approaches
Strong CYP3A inhibitors: Nirogacestat Cmax increased by 2.5-fold and AUC by 8.2-fold following coadministration of a single dose of OGSIVEO (100 mg) with itraconazole (a strong CYP3A inhibitor). Nirogacestat AUC is predicted to increase by 6.33-, 5.19-, and 3.46-fold following coadministration of multiple doses of OGSIVEO (150 mg BID) with itraconazole, ketoconazole and clarithromycin (strong CYP3A inhibitors), respectively.
Moderate CYP3A inhibitors: Nirogacestat AUC is predicted to increase by 2.73- and 3.18-fold following coadministration of multiple doses of OGSIVEO (150 mg BID) with erythromycin (moderate CYP3A inhibitor) and fluconazole (moderate CYP3A inhibitor), respectively.
Strong CYP3A inducers: Nirogacestat AUC is predicted to decrease by 85% following coadministration of multiple doses of OGSIVEO (150 mg BID) with rifampin (strong CYP3A inducer).
Moderate CYP3A inducers: Nirogacestat AUC is predicted to decrease by 67% following coadministration of multiple doses of OGSIVEO (150 mg BID) with efavirenz (moderate CYP3A inducer).
CYP3A substrates: Midazolam (CYP3A substrate) Cmax is predicted to increase by 1.77-fold and AUC by 2.07-fold following concomitant use with multiple doses of OGSIVEO (150 mg BID).
CYP2C19 substrates: Concomitant use of multiple doses of OGSIVEO (150 mg BID) with a drug that is a sensitive substrate of CYP2C19 decreases the plasma concentrations of these substrates.
P-gp substrates: Exposure to dabigatran (P-gp substrate) Cmax and AUC were not affected by concomitant use with nirogacestat.
Drugs that increase gastric pH: Concomitant administration of proton pump inhibitors (e.g., omeprazole), histamine type 2 (H2)-receptor antagonists (e.g., famotidine), or antacids (e.g., calcium) is expected to reduce concentrations of nirogacestat.
Other Drugs
No clinically significant differences in nirogacestat pharmacokinetics were predicted when used concomitantly with cimetidine (weak CYP3A inhibitor).
No clinically significant differences were predicted in the pharmacokinetics of the following drugs when used concomitantly with nirogacestat: rosiglitazone (CYP2C8 substrate) or S-warfarin (CYP2C9 substrate).
In Vitro Studies
Nirogacestat does not inhibit CYP 1A2, 2B6, 2C8, 2C9, 2C19, and 2D6.
Nirogacestat is an inducer of CYP2B6, CYP2C8, CYP2C9, and CYP2C19, but does not induce CYP 1A2.
Transporter systems: Nirogacestat is a P-gp substrate, but not a substrate of BCRP, OATP1B1, and OATP1B3.
Nirogacestat is a P-gp inhibitor, but not an inhibitor of BCRP, MATE1, MATE2-K, OATP1B1, OATP1B3, OAT1, OAT2 and OAT3.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a 6-month carcinogenicity study, transgenic rasH2 mice received up to 100 mg/kg/day of oral nirogacestat, resulting in mean exposure levels (AUC) less than those in humans at the recommended dose of 150 mg twice daily. No statistically significant neoplastic findings occurred. The carcinogenic potential of nirogacestat in rats has not been assessed.
Mutagenesis
Nirogacestat was not mutagenic in a bacterial reverse mutation (Ames) assay and was not clastogenic in an in vitro chromosome aberration assay in human lymphocytes or in vivo rat bone marrow micronucleus study.
Impairment of Fertility
Nirogacestat resulted in reduced fertility when administered to male and female rats at doses ≥5 mg/kg/day (approximately 0.16 times the recommended dose of 150 mg twice daily based on body surface area (BSA), and a lack of fertility when administered to male and female rats at doses ≥ 40 mg/kg/day (approximately 1.3 times the recommended dose of 150 mg twice daily based on BSA). Adverse findings in rats included ovarian atrophy, reduced testes weights, and decreased sperm concentration and motility.
14. Clinical Studies
14.1 Desmoid Tumor
The efficacy of OGSIVEO was evaluated in DeFi (NCT03785964), an international, multicenter, randomized (1:1), double-blind, placebo-controlled trial in 142 adult patients with progressing desmoid tumors not amenable to surgery. Patients were eligible if the desmoid tumor had progressed within 12 months of screening. Patients with progressing desmoid tumor that would result in immediate risk to the patient were not eligible.
Patients were randomized to receive 150 mg OGSIVEO or placebo orally twice daily until disease progression or unacceptable toxicity. Patients were stratified by primary tumor(s) location (intra-abdominal versus extra-abdominal). Tumor imaging occurred every 3 months. Crossover was permitted at the time of radiographic progression. The major efficacy outcome was progression-free survival (PFS) based on RECIST v1.1 as assessed by blinded independent central review or on clinical progression by the investigator (and confirmed by independent review). Clinical progression required worsening of symptoms resulting in a global deterioration of health status causing the permanent discontinuation from trial treatment and the initiation of emergent treatment (e.g., radiotherapy, surgery, or systemic therapy including chemotherapy or tyrosine kinase inhibitors) for desmoid tumors. Objective response rate (ORR) was an additional efficacy outcome measure. Worst pain (item 3) was assessed daily using Brief Pain Inventory-Short Form (BPI-SF), an 11-point numerical rating scale ranging from 0 ("no pain") to 10 ("pain as bad as you can imagine") and averaged over 7 days prior to each visit.
A total of 142 patients were randomized. The median age was 34 years (range: 18 to 76); 65% were female; race was 83% White, 6% Black, 3% Asian, and other or not reported in 8%; and 73% had an ECOG performance status (PS) of 0, 27% had an ECOG PS of 1, and 0.7% had an ECOG PS of 2. Twenty-three percent of patients had intra-abdominal disease or both intra- and extra-abdominal disease, and 77% had only extra-abdominal disease. Forty-one percent of patients had multifocal disease and 59% had single focal disease. Of 105 patients with known tumor mutation status, 81% had a CTNNB1 mutation and 21% had an APC mutation. Seventeen percent of patients had a family history of familial adenomatous polyposis (FAP). Twenty-three percent of patients received no prior therapy, and 44% received ≥3 prior lines of therapy. Prior therapy included surgery (53%), radiotherapy (23%), and systemic therapy (61%). Thirty-three percent of patients were previously treated with a tyrosine kinase inhibitor and 36% were previously treated with chemotherapy. Fifty percent had a BPI-SF item 3 (worst pain) score of ≥2.
Efficacy results are summarized in Table 7 and Figure 1.
Table 7. Efficacy Results of DeFi:
| OGSIVEO N=70 | Placebo N=72 | |
|---|---|---|
| Progression-free Survival | ||
| Number (%) of patients with event | 12 (17) | 37 (51) |
| Radiographic progressiona | 11 (16) | 30 (42) |
| Clinical progressiona | 1 (1) | 6 (8) |
| Death | 0 | 1 (1) |
| Median (months) (95% CI) b | NR (NR, NR) | 15.1 (8.4, NR) |
| Hazard ratio (95% CI) | 0.29 (0.15, 0.55) | |
| p-valuec | < 0.001 | |
| Objective Response Ratea | ||
| ORR, n (%) 95% CId | 29 (41) (29.8, 53.8) | 6 (8) (3.1, 17.3) |
| CR | 5 (7) | 0 |
| PR | 24 (34) | 6 (8) |
| p-valuee | <0.001 | |
Abbreviations: CI: confidence interval; CR: complete response; ORR: objective response rate; PR: partial response; NR: Not Reached
a Assessed by blinded independent central review.
b Obtained using Kaplan-Meier Methodology.
c p-value was from a one-sided stratified log-rank test with placebo as reference.
d Obtained using exact method based on binomial distribution.
e p-value was from a two-sided Cochran-Mantel-Haenszel test.
Figure 1. Kaplan-Meier Curve of PFS in DeFi:
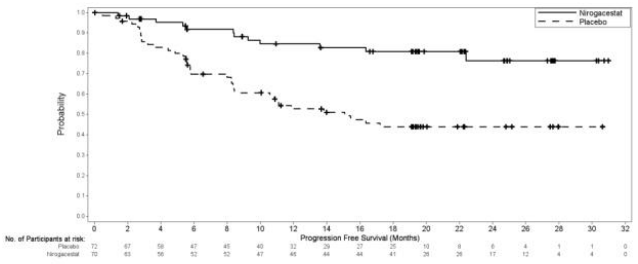
PFS results were supported by change from baseline in patient-reported worst pain favoring the OGSIVEO arm.
An exploratory analysis of PFS based on only radiographic progression demonstrated a hazard ratio of 0.31 (95% CI: 0.16, 0.62).
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.