ORILISSA Film-coated tablet Ref.[10902] Active ingredients: Elagolix
Source: FDA, National Drug Code (US) Revision Year: 2021
4. Contraindications
ORILISSA is contraindicated in women:
- Who are pregnant [see Use in Specific Populations (8.1)]. Exposure to ORILISSA early in pregnancy may increase the risk of early pregnancy loss.
- With known osteoporosis because of the risk of further bone loss [see Warnings and Precautions (5.1)]
- With severe hepatic impairment [see Use in Specific Populations (8.7), Clinical Pharmacology (12.3)]
- Taking inhibitors of organic anion transporting polypeptide (OATP)1B1 (a hepatic uptake transporter) that are known or expected to significantly increase elagolix plasma concentrations [see Drug Interactions (7.2)]
- With known hypersensitivity reaction to ORILISSA or any of its inactive components. Reactions have included anaphylaxis and angioedema [see Adverse Reactions (6.2)].
5. Warnings and Precautions
5.1 Bone Loss
ORILISSA causes a dose-dependent decrease in bone mineral density (BMD). BMD loss is greater with increasing duration of use and may not be completely reversible after stopping treatment [see Adverse Reactions (6.1)]. The impact of these BMD decreases on long-term bone health and future fracture risk are unknown.
ORILISSA is contraindicated in women with known osteoporosis [see Contraindications (4)]. Consider assessment of BMD in patients with a history of a low-trauma fracture or other risk factors for osteoporosis or bone loss. Limit the duration of use to reduce the extent of bone loss [see Dosage and Administration (2.2)]. Although the effect of supplementation with calcium and vitamin D was not studied, such supplementation may be beneficial for all patients.
5.2 Change in Menstrual Bleeding Pattern and Reduced Ability to Recognize Pregnancy
Women who take ORILISSA may experience a reduction in the amount, intensity or duration of menstrual bleeding, which may reduce the ability to recognize the occurrence of a pregnancy in a timely manner [see Adverse Reactions (6.1)]. Perform pregnancy testing if pregnancy is suspected, and discontinue ORILISSA if pregnancy is confirmed.
5.3 Suicidal Ideation, Suicidal Behavior, and Exacerbation of Mood Disorders
Suicidal ideation and behavior, including one completed suicide, occurred in subjects treated with ORILISSA in the endometriosis clinical trials. ORILISSA subjects had a higher incidence of depression and mood changes compared to placebo, and ORILISSA subjects with a history of suicidality or depression had a higher incidence of depression compared to subjects without such a history [see Adverse Reactions (6.1)]. Promptly evaluate patients with depressive symptoms to determine whether the risks of continued therapy outweigh the benefits [see Adverse Reactions (6.1)]. Patients with new or worsening depression, anxiety or other mood changes should be referred to a mental health professional, as appropriate. Advise patients to seek immediate medical attention for suicidal ideation and behavior. Reevaluate the benefits and risks of continuing ORILISSA if such events occur.
5.4 Hepatic Transaminase Elevations
In clinical trials, dose-dependent elevations of serum alanine aminotransferase (ALT) at least 3-times the upper limit of the reference range occurred with ORILISSA. Use the lowest effective dose of ORILISSA and instruct patients to promptly seek medical attention in case of symptoms or signs that may reflect liver injury, such as jaundice. Promptly evaluate patients with elevations in liver tests to determine whether the benefits of continued therapy outweigh the risks [see Adverse Reactions (6.1)].
5.5 Interactions with Hormonal Contraceptives
Advise women to use effective non-hormonal contraceptives during treatment with ORILISSA and for 28 days after discontinuing ORILISSA [see Use in Specific Populations (8.1, 8.3), Drug Interactions (7.1), Clinical Pharmacology (12.3)].
Increase in Estrogen Exposure and Potential Associated Increased Risks When ORILISSA 200 mg Twice Daily is Taken With Combined Hormonal Contraceptives
Co-administration of a combined oral contraceptive (COC) (containing 20 mcg ethinyl estradiol/0.1 mg levonorgestrel) following administration of ORILISSA 200 mg twice daily for 14 days increases the plasma ethinyl estradiol concentration by 2.2-fold compared to this COC alone. ORILISSA 200 mg twice daily co-administered with a COC containing ethinyl estradiol may lead to increased risk of ethinyl estradiol-related adverse events including thromboembolic disorders and vascular events and is not recommended [see Drug Interactions (7.1), Clinical Pharmacology (12.3)].
Potential for Reduced Efficacy of Progestin-Containing Hormonal Contraceptives
Co-administration of ORILISSA 200 mg twice daily and a COC containing 0.1 mg levonorgestrel decreases the plasma concentrations of levonorgestrel by 27%, potentially affecting contraceptive efficacy. Co-administration of ORILISSA with COCs containing norethindrone acetate did not show reduction in plasma concentrations of norethindrone [see Drug Interactions (7.1), Clinical Pharmacology (12.3)].
Co-administration of ORILISSA with progestin-containing intrauterine contraceptive systems has not been studied.
Reduced efficacy of ORILISSA
Based on the mechanism of action of ORILISSA, estrogen-containing contraceptives are expected to reduce the efficacy of ORILISSA. The effect of progestin-only contraceptives on the efficacy of ORILISSA is unknown.
6. Adverse Reactions
The following serious adverse reactions are discussed elsewhere in labeling:
- Bone loss [see Warnings and Precautions (5.1)]
- Change in menstrual bleeding pattern and reduced ability to recognize pregnancy [see Warnings and Precautions (5.2)]
- Suicidal ideation, suicidal behavior, and exacerbation of mood disorders [see Warnings and Precautions (5.3)]
- Hepatic transaminase elevations [see Warnings and Precautions (5.4)]
6.1. Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of ORILISSA was evaluated in two six-month, randomized, double-blind, placebo-controlled clinical trials [EM-1 (NCT01620528) and EM-2 (NCT01931670)] in which a total of 952 adult women with moderate to severe pain associated with endometriosis were treated with ORILISSA (475 with 150 mg once daily and 477 with 200 mg twice daily) and 734 were treated with placebo. The population age range was 18-49 years old. Women who completed six months of treatment and met eligibility criteria continued treatment in two uncontrolled, blinded six-month extension trials [EM-3 (NCT01760954) and EM-4 (NCT02143713)], for a total treatment duration of up to 12 months.
Serious Adverse Events
Overall, the most common serious adverse events reported for subjects treated with ORILISSA in the two placebo-controlled clinical trials (Studies EM-1 and EM-2) included appendicitis (0.3%), abdominal pain (0.2%), and back pain (0.2%). In these trials, 0.2% of subjects treated with ORILISSA 150 mg once daily and 0.2% of subjects treated with ORILISSA 200 mg twice daily discontinued therapy due to serious adverse reactions compared to 0.5% of those given placebo.
Adverse Reactions Leading to Study Discontinuation
In the two placebo-controlled clinical trials (Studies EM-1 and EM-2), 5.5% of subjects treated with ORILISSA 150 mg once daily and 9.6% of subjects treated with ORILISSA 200 mg twice daily discontinued therapy due to adverse reactions compared to 6.0% of those given placebo. Discontinuations were most commonly due to hot flushes or night sweats (1.1% with 150 mg once daily and 2.5% with 200 mg twice daily) and nausea (0.8% with 150 mg once daily and 1.5% with 200 mg twice daily) and were dose-related. The majority of discontinuations due to hot flushes or night sweats (10 of 17, 59%) and nausea (7 of 11, 64%) occurred within the first 2 months of therapy.
In the two extension trials (Studies EM-3 and EM-4), discontinuations were most commonly due to decreased BMD and were dose-related. In these trials, 0.3% of subjects treated with ORILISSA 150 mg once daily and 3.6% of subjects treated with ORILISSA 200 mg twice daily discontinued therapy due to decreased BMD.
Common Adverse Reactions
Adverse reactions reported in ≥5% of women in the two placebo-controlled trials in either ORILISSA dose group and at a greater frequency than placebo are noted in the following table.
Table 2. Percentage of Subjects in Studies EM-1 and EM-2 with Treatment-Emergent Adverse Reactions Occurring in at Least 5% of Subjects (either ORILISSA Dose Group) and at a Greater Incidence than with Placebo:
| ORILISSA 150 mg Once Daily N=475 | ORILISSA 200 mg Twice Daily N=477 | Placebo N=734 | |
|---|---|---|---|
| % | % | % | |
| Hot Flush | 24 | 46 | 9 |
| Headache | 17 | 20 | 12 |
| Nausea | 11 | 16 | 13 |
| Insomnia | 6 | 9 | 3 |
| Mood altered, mood swings | 6 | 5 | 3 |
| Amenorrhea | 4 | 7 | <1 |
| Depressed mood, depression, depressive symptoms and/or tearfulness | 3 | 6 | 2 |
| Anxiety | 3 | 5 | 3 |
| Arthralgia | 3 | 5 | 3 |
The most commonly reported adverse reactions in the extension trials (EM-3 and EM-4) were similar to those in the placebo-controlled trials.
Less Common Adverse Reactions
In Study EM-1 and Study EM-2, adverse reactions reported in ≥3% and <5% in either ORILISSA dose group and greater than placebo included: decreased libido, diarrhea, abdominal pain, weight gain, dizziness, constipation and irritability.
Bone Loss
The effect of ORILISSA on BMD was assessed by dual-energy X-ray absorptiometry (DXA).
In Studies EM-1 and EM-2, there was a dose-dependent decrease in BMD in ORILISSA-treated subjects compared to an increase in placebo-treated subjects.
In Study EM-1, compared to placebo, the mean change from baseline in lumbar spine BMD at 6 months was -0.9% (95% CI: -1.3, -0.4) with ORILISSA 150 mg once daily and -3.1% (95% CI: -3.6, -2.6) with ORILISSA 200 mg twice daily (Table 3). The percentage of subjects with greater than 8% BMD decrease in lumbar spine, total hip or femoral neck at any time point during the placebo-controlled treatment period was 2% with ORILISSA 150 mg once daily, 7% with ORILISSA 200 mg twice daily and <1% with placebo. In the blinded extension Study EM-3, continued bone loss was observed with 12 months of continuous treatment with ORILISSA. The percentage of subjects with greater than 8% BMD decrease in lumbar spine, total hip or femoral neck at any time point during the extension treatment period was 8% with continuous ORILISSA 150 mg once daily and 21% with continuous ORILISSA 200 mg twice daily.
In Study EM-2, compared to placebo, the mean change from baseline in lumbar spine BMD at 6 months was -1.3% (95% CI: -1.8, -0.8) with ORILISSA 150 mg once daily and -3.0% (95% CI: -3.5, -2.6) with ORILISSA 200 mg twice daily (Table 3). The percentage of subjects with greater than 8% BMD decrease in lumbar spine, total hip or femoral neck at any time point during the placebo-controlled treatment period was < 1% with ORILISSA 150 mg once daily, 6% with ORILISSA 200 mg twice daily and 0% with placebo. In the blinded extension Study EM-4, continued bone loss was observed with 12 months of continuous treatment with ORILISSA. The percentage of subjects with greater than 8% BMD decrease in lumbar spine, total hip or femoral neck at any time point during the extension treatment period was 2% with continuous ORILISSA 150 mg once daily and 21% with continuous ORILISSA 200 mg twice daily.
Table 3. Percent Change from Baseline in Lumbar Spine BMD at Month 6:
| ORILISSA 150 mg Once Daily | ORILISSA 200 mg Twice Daily | Placebo | |
|---|---|---|---|
| EM-1 | |||
| N | 183 | 180 | 277 |
| Percent Change from Baseline, % | -0.3 | -2.6 | 0.5 |
| Treatment Difference, % (95% CI) | -0.9 (-1.3, -0.4) | -3.1 (-3.6, -2.6) | |
| EM-2 | |||
| N | 174 | 183 | 271 |
| Percent Change from Baseline, % | -0.7 | -2.5 | 0.6 |
| Treatment Difference, % (95% CI) | -1.3 (-1.8, -0.8) | -3.0 (-3.5, -2.6) | |
To assess for recovery, the change in lumbar spine BMD over time was analyzed for subjects who received continuous treatment with ORILISSA 150 mg once daily or ORILISSA 200 mg twice daily for up to 12 months and who were then followed after cessation of therapy for an additional 6 months. Partial recovery of BMD was seen in these subjects (Figure 1).
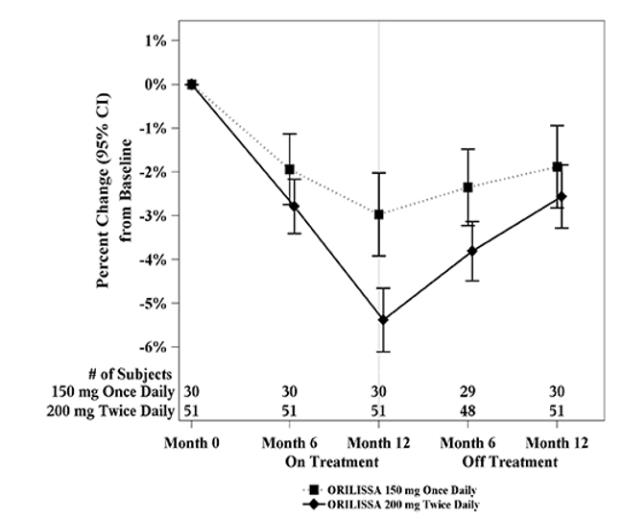
In Study EM-3, if a subject had BMD loss of more than 1.5% at the lumbar spine or more than 2.5% at the total hip at the end of treatment, follow-up DXA was required after 6 months off-treatment. In Study EM-4, all subjects were required to have a follow-up DXA 6 months off treatment regardless of change in BMD and if a subject had BMD loss of more than 1.5% at the lumbar spine or more than 2.5% at the total hip after 6 months off treatment, follow-up DXA was required after 12 months off-treatment. Figure 2 shows the change in lumbar spine BMD for the subjects in Study EM-2/EM-4 who completed 12 months of treatment with ORILISSA and who had a follow-up DXA 12-months off treatment.
Figure 1. Percent Change from Baseline in Lumbar Spine BMD in Subjects Who Received 12 Months of ORILISSA and Had Follow-up BMD 6 Months off Therapy in Studies EM-2/EM-4:
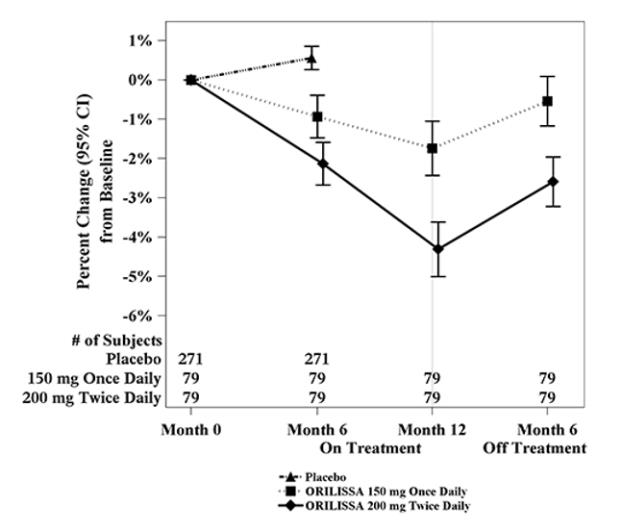
Figure 2. Percent Change from Baseline in Lumbar Spine BMD in Subjects Who Received 12 Months of ORILISSA and Had Follow-up BMD 12 Months off Therapy in Studies EM-2/EM-4:
Suicidal Ideation, Suicidal Behavior and Exacerbation of Mood Disorders
In the placebo-controlled trials (Studies EM-1 and EM-2), ORILISSA was associated with adverse mood changes (see Table 2 and Table 4), particularly in those with a history of depression.
Table 4. Suicidal Ideation and Suicidal Behavior in Studies EM-1 and EM-2:
| ORILISSA | Placebo (N=734) n (%) | ||
|---|---|---|---|
| Adverse Reactions | 150 mg Once Daily (N=475) n (%) | 200 mg Twice Daily (N=477) n (%) | |
| Completed suicide | 1 (0.2) | 0 | 0 |
| Suicidal ideation | 1 (0.2) | 1 (0.2) | 0 |
A 44-year-old woman received 31 days of ORILISSA 150 mg once daily then completed suicide 2 days after ORILISSA discontinuation. She had no relevant past medical history; life stressors were noted.
Among the 2090 subjects exposed to ORILISSA in the endometriosis Phase 2 and Phase 3 studies, there were four reports of suicidal ideation. In addition to the two subjects in Table 4, there were two additional reports of suicidal ideation: one subject in EM-3 (150 mg once daily) and one in a Phase 2 study (75 mg once daily, an unapproved dose). Three of these subjects had a history of depression. Two subjects discontinued ORILISSA and two completed the clinical trial treatment periods.
Hepatic Transaminase Elevations
In the placebo-controlled clinical trials (Studies EM-1 and EM-2), dose-dependent asymptomatic elevations of serum ALT to at least 3-times the upper limit of the reference range occurred during treatment with ORILISSA (150 mg once daily – 1/450, 0.2%; 200 mg twice daily – 5/443, 1.1%; placebo – 1/696, 0.1%). Similar increases were seen in the extension trials (Studies EM-3 and EM-4).
Changes in Lipid Parameters
Dose-dependent increases in total cholesterol, low-density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and serum triglycerides were noted during ORILISSA treatment in EM-1 and EM-2. In EM-1 and EM-2, 12% and 1% of subjects with mildly elevated LDL-C (130-159 mg/dL) at baseline had an increase in LDL-C concentrations to 190 mg/dL or higher during treatment with ORILISSA and placebo, respectively. In EM-1 and EM-2, 4% and 1% of subjects with mildly elevated serum triglycerides (150-300 mg/dL) at baseline had an increase in serum triglycerides to at least 500 mg/dL during treatment with ORILISSA and placebo, respectively. The highest measured serum triglyceride concentration during treatment with ORILISSA was 982 mg/dL.
Table 5. Mean Change and Maximum Increase from Baseline in Serum Lipids in Studies EM-1 and EM-2:
| ORILISSA 150 mg Once Daily N=475 | ORILISSA 200 mg Twice Daily N=477 | Placebo N=734 | |
|---|---|---|---|
| LDL-C (mg/dL) | |||
| Mean change at Month 6 | 5 | 13 | -3 |
| Maximum increase during Treatment Period | 137 | 107 | 122 |
| HDL-C (mg/dL) | |||
| Mean change at Month 6 | 2 | 4 | 1 |
| Maximum increase during Treatment Period | 43 | 52 | 45 |
| Triglycerides (mg/dL) | |||
| Mean change at Month 6 | <1 | 11 | -3 |
| Maximum increase during Treatment Period | 624 | 484 | 440 |
Lipid increases occurred within 1 to 2 months after the start of ORILISSA and remained stable thereafter over 12 months.
Hypersensitivity Reactions
In Studies EM-1 and EM-2, non-serious hypersensitivity reactions including rash occurred in 5.8% of ORILISSA treated-subjects and 6.1% of placebo-treated subjects. These events led to study drug discontinuation in 0.4% of ORILISSA-treated subjects and 0.5% of placebo-treated subjects.
Effects on Menstrual Bleeding Patterns
The effects of ORILISSA on menstrual bleeding were evaluated for up to 12 months using an electronic daily diary where subjects classified their flow of menstrual bleeding (if present in the last 24 hours) as spotting, light, medium, or heavy. ORILISSA led to a dose-dependent reduction in mean number of bleeding and spotting days and bleeding intensity in those subjects who reported menstrual bleeding.
Table 6. Mean Bleeding/Spotting Days and Mean Intensity Scores at Month 3:
| ORILISSA 150mg Once Daily | ORILISSA 200mg Twice Daily | Placebo | ||||
|---|---|---|---|---|---|---|
| Baseline | Month 3 | Baseline | Month 3 | Baseline | Month 3 | |
| Mean bleeding/ spotting days in prior 28 days | 5.3 | 2.8 | 5.7 | 0.8 | 5.4 | 4.6 |
| Mean Intensity scorea | 2.6 | 2.2 | 2.5 | 2.0 | 2.6 | 2.4 |
a Intensity for subjects who reported at least 1 day of bleeding or spotting during 28 day interval. Scale ranges from 1 to 4, 1 = spotting, 2 = light, 3 = medium, 4 = heavy
ORILISSA also demonstrated a dose-dependent increase in the percentage of women with amenorrhea (defined as no bleeding or spotting in a 56-day interval) over the treatment period. The incidence of amenorrhea during the first six months of treatment ranged from 6-17% for ORILISSA 150 mg once daily, 13-52% for ORILISSA 200 mg twice daily and less than 1% for placebo. During the second 6 months of treatment, the incidence of amenorrhea ranged from 11-15% for ORILISSA 150 mg once daily and 46-57% for ORILISSA 200 mg twice daily.
After 6 months of therapy with ORILISSA 150 mg once daily, resumption of menses after stopping treatment was reported by 59%, 87% and 95% of women within 1, 2, and 6 months, respectively. After 6 months of therapy with ORILISSA 200 mg twice daily, resumption of menses after stopping treatment was reported by 60%, 88%, and 97% of women within 1, 2, and 6 months, respectively.
After 12 months of therapy with ORILISSA 150 mg once daily resumption of menses after stopping treatment was reported by 77%, 95% and 98% of women within 1, 2, and 6 months respectively. After 12 months of therapy with ORILISSA 200 mg twice daily resumption of menses after stopping treatment was reported by 55%, 91% and 96% of women within 1, 2, and 6 months respectively.
6.2. Postmarketing Experience
The following adverse reactions have been identified during post-approval use of ORILISSA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune system disorders: hypersensitivity reactions (including anaphylaxis, angioedema, and urticaria).
7. Drug Interactions
7.1 Potential for ORILISSA to Affect Other Drugs
Elagolix is:
- A weak to moderate inducer of cytochrome P450 (CYP) 3A. Co-administration with ORILISSA may decrease plasma concentrations of drugs that are substrates of CYP3A (see Table 7).
- A weak inhibitor of CYP 2C19. Co-administration with ORILISSA may increase plasma concentrations of drugs that are substrates of CYP2C19 (see Table 7).
- An inhibitor of efflux transporter P-glycoprotein (P-gp). Co-administration with ORILISSA may increase plasma concentrations of drugs that are substrates of P-gp (see Table 7).
The effects of co-administration of ORILISSA on concentrations of concomitant drugs and the clinical recommendations for these drug interactions are summarized in Table 7.
Table 7. Drug Interactions: Effects of ORILISSA on Other Drugs
| Concomitant Drug Class: Drug Name | Effect on Plasma Exposure of Concomitant Drug | Clinical Recommendations |
|---|---|---|
| Cardiac glycosides: digoxin | ↑ digoxin | Increase monitoring of digoxin concentrations and potential signs and symptoms of clinical toxicity when initiating ORILISSA in patients who are taking digoxin. If ORILISSA is discontinued, increase monitoring of digoxin concentrations. |
| Benzodiazepines: oral midazolam | ↓ midazolam | Consider increasing the dose of midazolam by no more than 2-fold and individualize midazolam therapy based on the patient's response. |
| Statins: rosuvastatin | ↓ rosuvastatin | Monitor lipid levels and adjust the dose of rosuvastatin, if necessary. |
| Proton pump inhibitors: omeprazole | ↑ omeprazole | No dose adjustment needed for omeprazole 40 mg once daily when co-administered with ORILISSA. When ORILISSA is used concomitantly with higher doses of omeprazole, consider dosage reduction of omeprazole. |
| Combined hormonal contraceptives: oral ethinyl estradiol/levonorgestrel | ↑ethinyl estradiol ↓levonorgestrel | Advise women to use effective non-hormonal contraception during treatment with ORILISSA and for 28 days after discontinuing ORILISSA. |
See Tables 10 and 11 [see Clinical Pharmacology (12.3)].
The direction of the arrow indicates the direction of the change in the area under the curve (AUC) (↑= increase, ↓ = decrease).
7.2 Potential for Other Drugs to Affect ORILISSA
Elagolix is a substrate of CYP3A, P-gp, and OATP1B1.
Concomitant use of ORILISSA 200 mg twice daily and strong CYP3A inhibitors for more than 1 month is not recommended. Limit concomitant use of ORILISSA 150 mg once daily and strong CYP3A inhibitors to 6 months.
Co-administration of ORILISSA with strong CYP3A inducers may decrease elagolix plasma concentrations and may result in a decrease of the therapeutic effects of ORILISSA.
Concomitant use of ORILISSA 200 mg twice daily and rifampin is not recommended. Limit concomitant use of ORILISSA 150 mg once daily and rifampin to 6 months.
The effect of concomitant use of P-gp inhibitors or inducers on the pharmacokinetics of ORILISSA is unknown. OATP1B1 inhibitors that are known or expected to significantly increase elagolix plasma concentrations are contraindicated due to increased risk of elagolix-associated adverse reactions [see Contraindications (4)].
8.1. Pregnancy
Pregnancy Exposure Registry
There is a pregnancy registry that monitors outcomes in women who become pregnant while treated with ORILISSA. Pregnant patients should be encouraged to enroll by calling 1-833-782-7241.
Risk Summary
Use of ORILISSA is contraindicated in pregnant women. Exposure to ORILISSA early in pregnancy may increase the risk of early pregnancy loss. Discontinue ORILISSA if pregnancy occurs during treatment.
The limited human data with the use of ORILISSA in pregnant women are insufficient to determine whether there is a risk for major birth defects or miscarriage. Although two cases of congenital malformations were reported in clinical trials with ORILISSA, no pattern was identified and miscarriages were reported at a similar incidence across treatment groups (see Data).
When pregnant rats and rabbits were orally dosed with elagolix during the period of organogenesis, postimplantation loss was observed in pregnant rats at doses 20 times the maximum recommended human dose (MRHD). Spontaneous abortion and total litter loss was observed in rabbits at doses 7 and 12 times the MRHD. There were no structural abnormalities in the fetuses at exposures up to 40 and 12 times the MRHD for the rat and rabbit, respectively (see Data).
Data
Human Data
There were 49 pregnancies reported in clinical trials of more than 3,500 women (of whom more than 2,000 had endometriosis) treated with ORILISSA for up to 12 months. These pregnancies occurred while the women were receiving ORILISSA or within 30 days after stopping ORILISSA. Among these 49 pregnancies, two major congenital malformations were reported. In one case of infant cleft palate, the mother was treated with ORILISSA 150 mg daily and the estimated fetal exposure to ORILISSA occurred during the first 30 days of pregnancy. In one case of infant tracheoesophageal fistula, the mother was treated with ORILISSA 150 mg daily and the estimated fetal exposure to ORILISSA occurred during the first 15 days of pregnancy.
Among these 49 pregnancies, there were five cases of spontaneous abortion (miscarriage) compared to five cases among the 20 pregnancies that occurred in more than 1100 women treated with placebo. Although the duration of fetal exposure was limited in ORILISSA clinical trials, there were no apparent decreases in birth weights associated with ORILISSA in comparison to placebo.
Animal Data
Embryofetal development studies were conducted in the rat and rabbit. Elagolix was administered by oral gavage to pregnant rats (25 animals/dose) at doses of 0, 300, 600 and 1200 mg/kg/day and to rabbits (20 animals/dose) at doses of 0, 100, 150, and 200 mg/kg/day, during the period of organogenesis (gestation day 6-17 in the rat and gestation day 7-20 in the rabbit).
In rats, maternal toxicity was present at all doses and included six deaths and decreases in body weight gain and food consumption. Increased postimplantation losses were present in the mid dose group, which was 20 times the MRHD based on AUC. In rabbits, three spontaneous abortions and a single total litter loss were observed at the highest, maternally toxic dose, which was 12 times the MRHD based on AUC. A single total litter loss occurred at a lower non-maternally toxic dose of 150 mg/kg/day, which was 7 times the MRHD.
No fetal malformations were present at any dose level tested in either species even in the presence of maternal toxicity. At the highest doses tested, the exposure margins were 40 and 12 times the MRHD for the rat and rabbit, respectively. However, because elagolix binds poorly to the rat gonadotropin-releasing hormone (GnRH) receptor (~1000 fold less than to the human GnRH receptor), the rat study is unlikely to identify pharmacologically mediated effects of elagolix on embryofetal development. The rat study is still expected to provide information on potential non-target-related effects of elagolix.
In a pre- and postnatal development study in rats, elagolix was given in the diet to achieve doses of 0, 100 and 300 mg/kg/day (25 per dose group) from gestation day 6 to lactation day 20. There was no evidence of maternal toxicity. At the highest dose, two dams had total litter loss, and one failed to deliver. Pup survival was decreased from birth to postnatal day 4. Pups had lower birth weights and lower body weight gains were observed throughout the pre-weaning period at 300 mg/kg/day. Smaller body size and effect on startle response were associated with lower pup weights at 300 mg/kg/day. Post-weaning growth, development and behavioral endpoints were unaffected.
Maternal plasma concentrations in rats on lactation day 21 at 100 and 300 mg/kg/day (47 and 125 ng/mL) were 0.06-fold and 0.16-fold the maximal elagolix concentration (Cmax) in humans at the MRHD. Because the exposures achieved in rats were much lower than the human MRHD, this study is not predictive of potentially higher lactational exposure in humans.
8.2. Lactation
Risk Summary
There is no information on the presence of elagolix or its metabolites in human milk, the effects on the breastfed child, or the effects on milk production. There are no adequate animal data on the excretion of ORILISSA in milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for ORILISSA and any potential adverse effects on the breastfed child from ORILISSA.
Data
There are no adequate animal data on excretion of ORILISSA in milk.
8.3. Females and Males of Reproductive Potential
Based on the mechanism of action, there is a risk of early pregnancy loss if ORILISSA is administered to a pregnant woman [see Use in Specific Populations (8.1), Clinical Pharmacology (12.1)].
Pregnancy Testing
ORILISSA may delay the ability to recognize the occurrence of a pregnancy because it may reduce the intensity, duration, and amount of menstrual bleeding. Exclude pregnancy before initiating treatment with ORILISSA. Perform pregnancy testing if pregnancy is suspected during treatment with ORILISSA and discontinue treatment if pregnancy is confirmed [see Contraindications (4) and Warnings and Precautions (5.2)].
Contraception
Advise women to use effective non-hormonal contraception during treatment with ORILISSA and for 28 days after discontinuing ORILISSA [see Warnings and Precautions (5.5)].
8.4. Pediatric Use
Safety and effectiveness of ORILISSA in pediatric patients have not been established.
8.6. Renal Impairment
No dose adjustment of ORILISSA is required in women with any degree of renal impairment or end-stage renal disease (including women on dialysis) [see Clinical Pharmacology (12.3)].
8.7. Hepatic Impairment
No dosage adjustment of ORILISSA is required for women with mild hepatic impairment (Child-Pugh A). Only the 150 mg once daily regimen is recommended for women with moderate hepatic impairment (Child-Pugh B) and the duration of treatment should be limited to 6 months.
ORILISSA is contraindicated in women with severe hepatic impairment (Child-Pugh C) [see Contraindications (4), and Clinical Pharmacology (12.3)].
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.